


To describe the clinical history of a child with aggressive behavior and recurring death-theme speech, and report the experience of the team of authors, who proposed an alternative to medication through the establishment of a protection network and the inter-sector implementation of the circle of security concept.
Case descriptionA 5-year-old child has a violent and aggressive behavior at the day-care. The child was diagnosed by the healthcare center with depressive disorder and behavioral disorder, and was medicated with sertraline and risperidone. Side effects were observed, and the medications were discontinued. Despite several actions, such as talks, teamwork, psychological and psychiatric follow-up, the child's behavior remained unchanged.
RemarksA unique therapeutic project was developed by Universidade Estadual de Campinas' Medical School students in order to establish a connection between the entities responsible for the child's care (daycare center, healthcare center, and family). Thus, the team was able to develop a basic care protection network. The implementation of the inter-sector circle of security, as well as the communication and cooperation among the teams, produced very favorable results in this case. This initiative was shown to be a feasible and effective alternative to the use of medication for this child.
Descrever o caso clínico de uma criança que apresenta comportamento agressivo e fala recorrente do tema de morte, e relatar a experiência da equipe de autores na proposição de uma alternativa à medicalização por meio da formação de uma Rede de Proteção e da aplicação Intersetorial do conceito de Círculo de Segurança da Criança.
Descrição do casoCriança de 5 anos apresenta comportamento violento e agressivo na creche que frequenta. Foi diagnosticado pelo Centro de Saúde com Transtorno Depressivo e Transtorno de Conduta, sendo medicado com Sertralina e Risperidona. Apresentou efeitos colaterais, interrompendo o uso das medicações. Apesar de ações como conversas, trabalho em grupos, acompanhamento psicológico e psiquiátrico, a criança manteve esse comportamento.
ComentáriosFoi desenvolvido um Projeto Terapêutico Singular por alunos do curso de Medicina da Universidade Estadual de Campinas (UNICAMP) com o objetivo de criar um vínculo entre as instituições responsáveis pelo cuidado da criança (Creche, Centro de Saúde e família), o que possibilitou o desenvolvimento de uma rede de proteção para o cuidado na Atenção Básica. A aplicação intersetorial do Círculo de Segurança, assim como a comunicação e a colaboração entre as equipes, mostrou resultados muito positivos neste caso, configurando-se como uma alternativa acessível e eficaz à Medicalização da criança.
The medicalization of childhood is one of the most discussed topics in the current pediatric setting. Children whose behavior does not correspond to that expected by school and society are perceived as suffering from organic diseases, including psychotic disorders.1
Collares and Moysés2 define pathologization as “the search for medical causes and solutions, at an organicistic and individual level, to problems eminently of social origin”, and medicalization as “the process of transforming non-medical issues, eminently of social and political origin, into medical issues, that is, trying to find in the medical field causes and solutions for problems of this nature”. They state that the medicalization “occurs according to a conception of medical science that discusses the health-disease process as focused on the individual, favoring the biological, organicistic approach”.2 It is, therefore, an omission on the part of medical institutions, school, and family in relation to problems of emotional and psychological nature. As a result of stigmatization, blaming and authoritarian attitudes are taken, attributing to the behavioral problem purely organic causes, without having investigated the real reason for the aggressive posture or hyperactivity.1,3
The concept of “circle of security”, proposed by Marvin et al,4 corresponds to an early intervention in the relationships between the child and their caregivers in order to provide adequate emotional support during childhood. The theory helps in the observation of the different ways in which children approach adults when demanding support and attention, and how to teach them to make good use of the help they receive. Moreover, the circle contributes to the perception of the real emotional issues present at the moment when the child modifies their behavior, helping the caregiver to identify the psychological and emotional demands that the child has difficulty expressing.
The circle of security diagram provides instructions to parents and professionals regarding the fundamental attitudes in creating a stable and safe environment for children to develop their emotions. They must have a safety base to be able to explore the world, with support for playing and protection. Then, a safe haven is necessary, to which the child can return when experiencing frustrating situations. At this moment, the adults should welcome the child and help them organize their feelings.4 This theory is very useful for professionals who work with children of all ages, as it helps to create safe opportunities for the development of interpersonal relationships, and teaches strategies to help professionals to present themselves as more emotionally available when approached by children.
The concept of protection network,5 in turn, must be understood as an integrated action among institutions to treat children and adolescents at personal risk situations - for instance, under threat and violation of rights by abandonment, physical and psychological violence, or neglect situations that cause physical and emotional damage. Thus, a functional and effective network protection gives the child the possibility of growing, free from social risks and domestic violence.
In this context, this study consisted of the report of an individual therapeutic project aimed to investigate and intervene on the different aspects of the management in the care of the child in question, focusing on the creation of an intersectorial link between health (healthcare center [HC]), education (daycare center), and family, aiming to establish an articulated protection network and apply the concept of circle of security as an alternative to pathologization and medicalization.
This experience was a mandatory training for students of the fifth year of Universidade Estadual de Campinas (UNICAMP) Medical School, as part of the discipline of Public Health. It was approved by the Undergraduate School Council of Medical Sciences and authorized by the Municipal Health Secretariat of Campinas.
Case reportThe case of a 5-year-old male child that lives with his mother (28 years), father (36 years), and a younger brother is reported. The daycare center, which the child attends full time, has made constant complaints since he started attending it due to his aggressive and violent behavior.
Initially, the problems were restricted to constant verbalization about the wish to die and the intent to kill himself and his classmates. Later, he began to display attitudes such as spitting at and kicking teachers and classmates; isolating himself from the other children and talking to himself; throwing feces at the other children; hiding knives in his backpack (“I'll take it to kill,” the boy said to his mother); and physically threatening another child by putting a knife to their neck during lunch at school.
The daycare center sought help at the Basic Health Unit of the area where it is located, believing it to be a pathological condition. The HC chose to include the child and his mother in a group of parents and children with learning problems, a solution that proved to be ineffective, as the child's behavior persisted. The team then chose to use medications to treat him. The medical record contained two consultations with a psychiatrist, who gave a diagnosis of behavioral disorder and depressive disorder. He was initially treated with sertraline 25mg, later replaced by risperidone 0.5 mg, but side effects were observed, and the mother chose to discontinue the medication use.
The problem was reported to the UNICAMP's team of students due to the complexity of the case, the strained relationship between the daycare center team and the HC, and the failure of the applied therapeutic proposals; in spite of conversations, inclusion in groups, psychological counseling, and use of psychiatric medications, the child's behavior, considered by the teams as a pathological issue, persisted.
The group used tools such as drawings as a projective resource for the child approach and family genogram after interviews with the mother. The decision to focus the discussions with the daycare center and the HC on the problematization of the situation, instead of discussing the prescriptions, showed to be a more effective approach to include teams in the dialogue and get them involved in the case. In addition to interviews with the different individuals involved and visits to the family and daycare center to increase the understanding of the case, the concept of circle of security was implemented during meetings with the teams, enabling them to apply this concept as a strategy for the intersectorial care of the child.
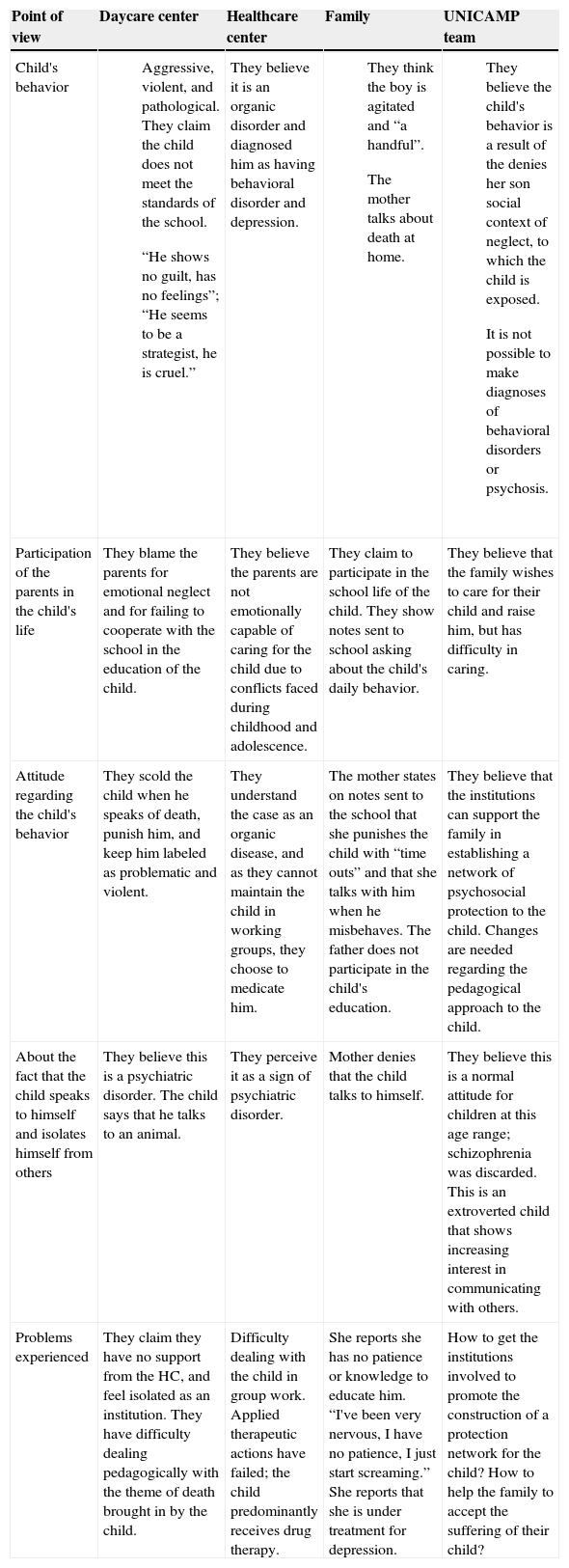
DiscussionTable 1 presents the different points of view of the teams involved in the care of the child regarding certain topics relevant to the clinical case. The opinions were collected by the group of students during a family interview, individual interviews, visits to the family home, visit to the daycare center, and meeting with the staff of the HC. The opinion of the UNICAMP team is the result of discussions among the students, guided by a psychologist, a pediatrician, and a child psychiatrist.
Viewpoints of the different groups involved in the child's care in relation to his behavior, family involvement, and attitudes regarding the experienced problems
| Point of view | Daycare center | Healthcare center | Family | UNICAMP team |
|---|---|---|---|---|
| Child's behavior |
| They believe it is an organic disorder and diagnosed him as having behavioral disorder and depression. |
|
|
| Participation of the parents in the child's life | They blame the parents for emotional neglect and for failing to cooperate with the school in the education of the child. | They believe the parents are not emotionally capable of caring for the child due to conflicts faced during childhood and adolescence. | They claim to participate in the school life of the child. They show notes sent to school asking about the child's daily behavior. | They believe that the family wishes to care for their child and raise him, but has difficulty in caring. |
| Attitude regarding the child's behavior | They scold the child when he speaks of death, punish him, and keep him labeled as problematic and violent. | They understand the case as an organic disease, and as they cannot maintain the child in working groups, they choose to medicate him. | The mother states on notes sent to the school that she punishes the child with “time outs” and that she talks with him when he misbehaves. The father does not participate in the child's education. | They believe that the institutions can support the family in establishing a network of psychosocial protection to the child. Changes are needed regarding the pedagogical approach to the child. |
| About the fact that the child speaks to himself and isolates himself from others | They believe this is a psychiatric disorder. The child says that he talks to an animal. | They perceive it as a sign of psychiatric disorder. | Mother denies that the child talks to himself. | They believe this is a normal attitude for children at this age range; schizophrenia was discarded. This is an extroverted child that shows increasing interest in communicating with others. |
| Problems experienced | They claim they have no support from the HC, and feel isolated as an institution. They have difficulty dealing pedagogically with the theme of death brought in by the child. | Difficulty dealing with the child in group work. Applied therapeutic actions have failed; the child predominantly receives drug therapy. | She reports she has no patience or knowledge to educate him. “I've been very nervous, I have no patience, I just start screaming.” She reports that she is under treatment for depression. | How to get the institutions involved to promote the construction of a protection network for the child? How to help the family to accept the suffering of their child? |
There was a clear attempt at the individualization of the problem by the staff of the daycare center and HC, attributing to the child an organic disease associated with personality alteration, which would explain his unconventional and inappropriate behavior as per school parameters. This is a hurried and guilt-inducing evaluation that contradicts the proposal by Dolto:6,7 “Before receiving more information, we do not accept the proposed alternative: illness or evilness. The first of these interpretations removes all responsibility from the child; the second gives him all the responsibility.” The daycare center believed that the attitudes of the child were due to his being evil, as the child did not demonstrate guilt nor emotions. The HC believed that the child has a disease and, therefore, treated him with medication.
It is an established idea that interpersonal relationships and the events occurring in everyday family life influence the individual's development.8-10 A more careful and detailed analysis of the whole context allows for the conclusion that the child's behavior is due more to structural problems of the family dynamics and the pedagogical model of the daycare center than to an organic illness or personality disorder.
It is believed that the child in question would benefit from individual psychotherapy to address family issues, emotional development, and socialization skills. Moreover, it would be essential to modify the pedagogical approach, without the prevailing of purely normative attitudes, so there is encouragement to the assimilation of rules by using playful and dialogical strategies. When he voices the topic of death, it would be preferable to confront him with affectionate words and propose activities to enhance his self-esteem.
According to Junqueira,11 intersectoriality is the articulation of knowledge and experiences from different sectors in planning, conducting, and evaluating actions in order to achieve integrated results in complex situations, seeking a synergistic effect in social development. In this context, it is essential to develop a network of protection comprised by the healthcare system, the school, and family so that the child is provided with a healthy environment in which he can adequately develop affectivity and learn to cope with his frustrations during the growth process, as recommended by Marvin et al4 and Cooper et al12
Moreover, the problematization approach implemented with the involved institutions on the practical application of the circle of security, as well as the possibilities of developing a protection network, based on the communication and collaboration between the teams, demonstrated to be a very positive strategy in this case, as the teams were able to recognize these resources as an accessible and effective alternative to the pathologization and the medicalization of the child.
Conflict of interestThe authors declare no conflicts of interest.
