





The aim of this article is to present a treatment alternative for microdontia rehabilitation and dental retention. The concept of ideal intercuspation assumes a strict relationship between tooth size and the size of the maxillary and mandibular arches. An impacted maxillary central incisor in a child poses a disturbing esthetic dilemma because of its prominent location. This report presents a 13 year-old patient with microdontia of the upper lateral incisors and retention of the upper right central incisor. Treatment began with the surgical exposure of the retained incisor using light biomechanical traction forces and planning the prosthetic rehabilitation of the lateral incisors by setting up a functional occlusion. Therefore, orthodontics-periodontics-prosthesis interdisciplinary relationship provides an optimal combination for the integral rehabilitation of these patients.
El objetivo de este estudio es brindar una alternativa de tratamiento en la rehabilitación de la microdoncia y la retención dental. El concepto de una intercuspidación ideal implica una relación estricta entre el tamaño dental, el número de órganos dentales y el tamaño de los arcos maxilar y mandibular. Un incisivo central maxilar impactado en un niño, representa un dilema estético complejo debido a su localización prominente. Este reporte presenta un paciente de 13 años de edad con microdoncia de los incisivos laterales superiores y retención del incisivo central superior derecho. El tratamiento inicia con la exposición quirúrgica del incisivo retenido usando fuerzas biomecánicas ligeras para traccionarlo; planeando la rehabilitación protésica de los incisivos laterales al establecer una oclusión funcional. Por lo tanto, la interdisciplina en ortodoncia, periodoncia y prótesis bucal se convierte en una combinación óptima para la rehabilitación integral de estos pacientes.
In human dentition characteristics, complex processes intervene that have a close relationship with the growth and development of the whole craniofacial complex mainly in bones such as the maxilla and the mandible. Dental morphology is determined by environmental and genetic factors which are in a dynamic relationship that may cause single, partial or complete anomalies in dental development.
Dental anomalies affect not only form, size, position, number and developmental time but modify their histologic structure as well.1 Microdontia is an anomaly in which the affected teeth are smaller than normal.2
Teeth afflicted by size anomalies constitute cases of interest for the professional due to the problems in arch length that they may cause as well as to the facial esthetics challenge they pose; they may cause misalignment and undesirable dental drifts which support further, more serious problems (i.e. dental retention). Each microdontia case must be diagnosed and assessed according to its particularities.3,4 Radiographic imaging constitutes a valuable auxiliary for the identification of growth and development anomalies, since they may be detected by this method before the tooth's eruption. The consulted statistical data has established that microdontia is more common in the incisor area, specifically in lateral incisors, but may appear in any area of the dental arches.5
The microdontia can cause dimensional changes compressing the arch and they could be treated through restorative procedures to preserve aesthetics and occlusion. In this kind of disorders, the prosthetic procedures are the treatment of choice.6
The aim of this study was to provide a treatment alternative for microdontia rehabilitation and dental retention. The concept of ideal intercupation implies a strict relationship between tooth size and number of dental organs and the size of the maxillary and mandibular arches. A maxillary central incisor impaction in a child represents a complex esthetic dilemma due to its prominent location.
This case report presents a 13- year-old male patient with lateral incisor microdontiaand upper right central incisor retention. Orthodontic treatment began at the Periodontics clinic with the surgical exposure of the retained incisor. 0.022” Roth appliances were used with the conventional archwire sequence. In order to perform the orthodontic traction of the retained incisor light biomechanical forces were employed (approximation with wire ligature to the main archwire) and attachments to open space (NiTi open coils) to accommodate the microdontic lateral incisors in place. All this was planned for the prosthetic rehabilitation of the lateral incisors while trying to achieve functional occlusion.
Therefore, interdisciplinary treatment between orthodontics, periodontics and prosthetics becomes an optimal combination for the integral rehabilitation of these patients in whom not only esthetics is important but also the stomathognathic system function and leads us to success in dental treatments.
There is little research on microdontia in Orthodontics. However this problem afflicts a vast majority of the world's population. Nevertheless, this case report coincides with the findings of several authors who claim that the most susceptible area for tooth size anomalies of the microdontia kind is the upper anterior area, more specifically, the upper lateral incisors.1,7–9
In the same manner, our results coincide with many more authors who affirm that dental retention is hard to find in the anterior zone, but when diagnosed and treated early, it may be resolved and optimal and satisfying results may be achieved regarding esthetics and occlusal function.10–13
CASE REPORTThis case report describes a 13- year-old patient who was referred from the peripheral clinic «Las Águilas UNAM-FO» because he presented microdontia of the upper lateral incisors and retention of the upper right central incisor. In his past medical history, no relevant data was found and in his non-medical history he declared to be a 5th grade student born in Mexico City.
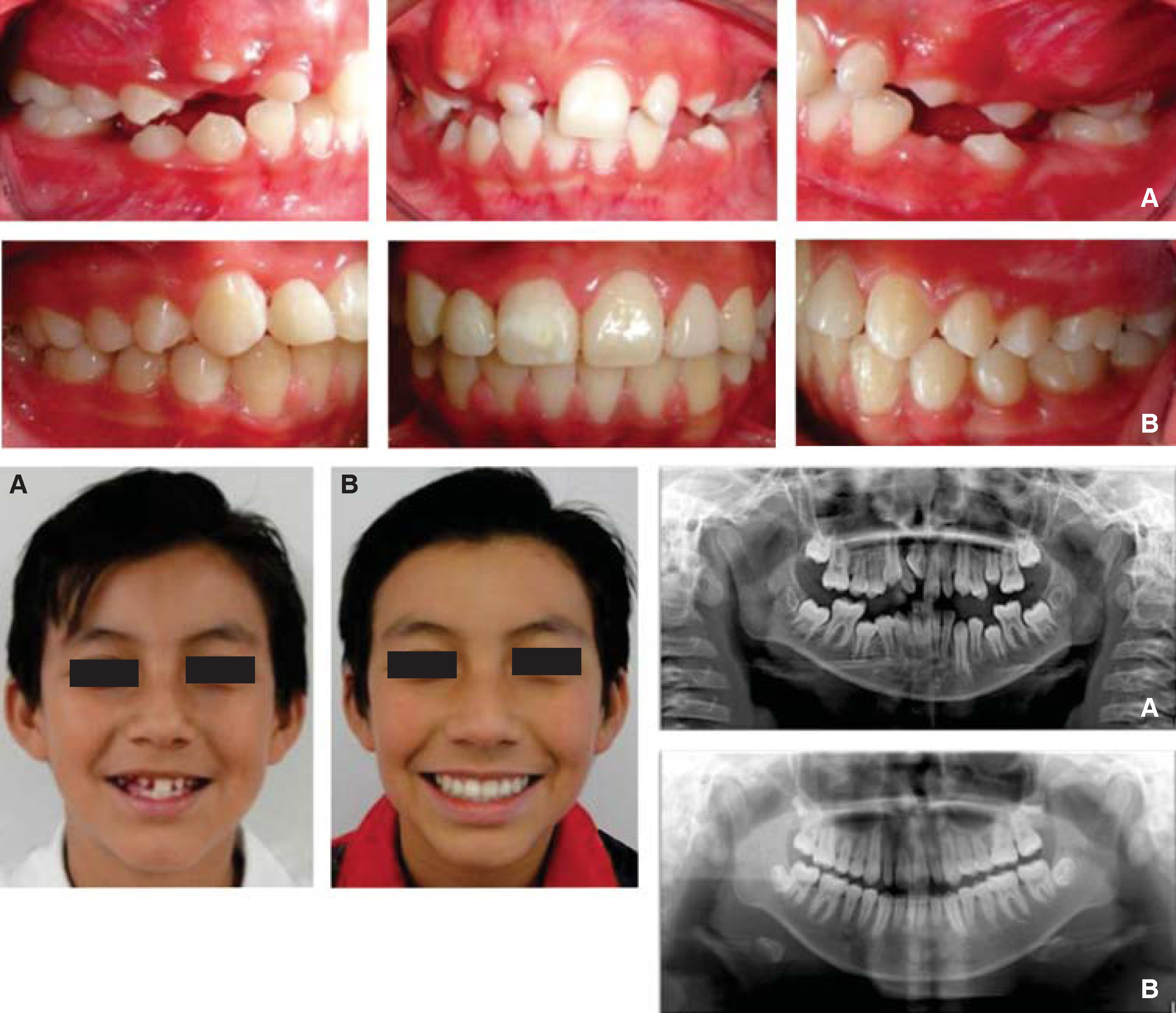
Upon clinical exploration 21 permanent teeth were observed as well as the clinical absence of the upper right central incisor and microdontia of the upper lateral incisors (Figure 1).

In the ortopantomography 28 permanent teeth were observed as well as the tooth germs of the lower third molars. The central incisor retention and the lateral incisor microdontia were confirmed (Figure 2). The study models revealed a bilateral molar class II, a non-assessable canine relationship, non-matching dental midlines, a 2mm overjet and a 3mm overbite. With the lateral headfilm the cephalometric diagnosis was concluded as a skeletal class II patient with vertical growth tendency (dolichofacial) an upper incisor retroclination.

Orthodontic treatment was initiated with the surgical exposure of the retained incisor at the Periodontics clinic in February of 2010. 0.022” Roth appliances was placed following a conventional archwire sequence (0.014” NiTi, 0.016” NiTi, 0.016” × 0.022” NiTi, 0.017” × 0.025” SS, 0.019” × 0.025” NiTi, 0.019” × 0.025” SS). For the upper incisor orthodontic traction light biomechanical forces were used (approximation to the main archwire with wire ligature and accessory archwires such as Overlay) and attachments for space opening (NiTi open coils) to place the lateral incisors in their correct position.
All of the above was performed planning for the prosthetic rehabilitation of the lateral incisors with ceromer crowns upon establishment of a functional occlusion at the end of treatment. Lastly, removable retainers (Hawley circumferential) would be used 24hours for a period of six months and 12hours the following 6 months with check-ups every three months for their adjustment.
Therefore, interdisciplinary treatment between orthodontics, periodontics and prosthetics becomes an optimal combination for the integral rehabilitation of these patients in whom not only esthetics is important but the function of the sotmatognathic system as well and which will lead us to success in dental treatments.
MATERIAL AND METHODSIn order to perform the patient's treatment, an interdisciplinary team formed by the specialties of orthodontics, periodontics and prosthodontics was required; each specialty team consisted of a student and a teacher.
The patient attended the orthodontics clinic claiming to have a retained tooth. This case report presents a 13 year old patient with microdontia of the upper lateral incisors and retention of the upper right central incisor.
For diagnosis elaboration, several auxiliaries were used: study models, extra and intraoral photgraphs, lateral headfilm, ortopantomography and periapical, occlusal and carpal radiographs.
Interdisciplinary treatment began at the Orthodontics clinic where he was diagnosed as a Skeletal class II due to a maxillary protrusion with a vertical growth tendency and microdontia of both upper lateral incisors and retention of the upper right central incisor.
Fixed appliances were placed with 0.022” Roth braces (GAC®) with a 0.014” NiTi archwire from the same brand for initial alignment and leveling. Afterwards, the patient was referred to the Periodontics clinic where the surgical exposure of the retained incisor was performed with a complete surgical flap and osteotomy with chisels. In the surgical process a lingual button was bonded with Heliosit orthodontic resin (Ivoclar). The patient was sutured with 000silk.
Orthodontic traction of the tooth was performed with the use of elastics and elastomeric chains to an accessory 0.028 stainless steel arc. Orthodontic treatment was continued with the conventional Roth archwire sequence: 0.016” NiTi, 0.016” × 0.022”NiTi, 0.017” × 0.025” SS, 0.019” × 0.025” NiTi, 0.019” × 0.025” SS (Ah Kim Pech brand®).
For vertical control, a high pull headgear from Ah Kim Pech® brand was used. All accessories used (elastomeric modules, elastomeric chains, wire ligature, open coils) were from Ah Kim Pech brand®.
Once a correct anterior and canine guide and posterior occlusal settling was achieved, a new interconsultation was made with the Prosthodontics clinic where a diagnostic wax-up was performed for the ceromer crown fabrication with Ivoclarint the microdontic upper lateral incisors.
The appliances were removed and retainers were placed: in the lower arch, a Hawley retainer with a 0.032” SS circumferential archwire and acrylic. In the upper arch a temporary retainer was made with a 0.040” rigid acetate.
Once the appliances were removed, the lateral incisors were reduced slightly at the tooth's neck with a conical bur. A silicone impression was obtained. Ceromer crowns were fabricated and cemented with light-curing dual resin from Ivoclarbrand and occlusal adjustments were made.
In the orthodontics clinic, final retainers made from 0.032” SS wire and acrylic, Hawley-shaped and with circumferential arc were placed.
Final records were obtained: panoramic radiograph and lateral headfilm; study models and facial and intraoral photographs.
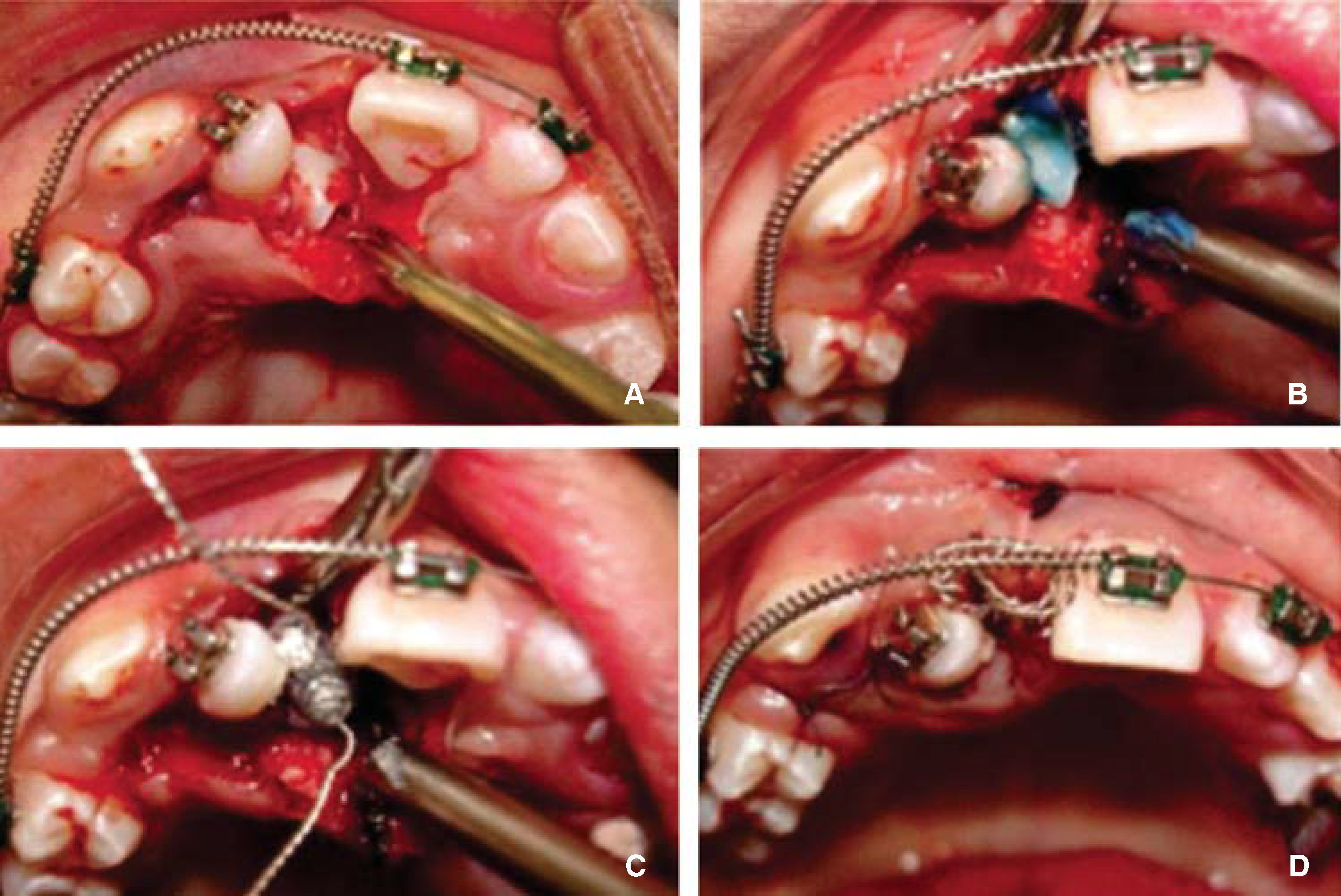
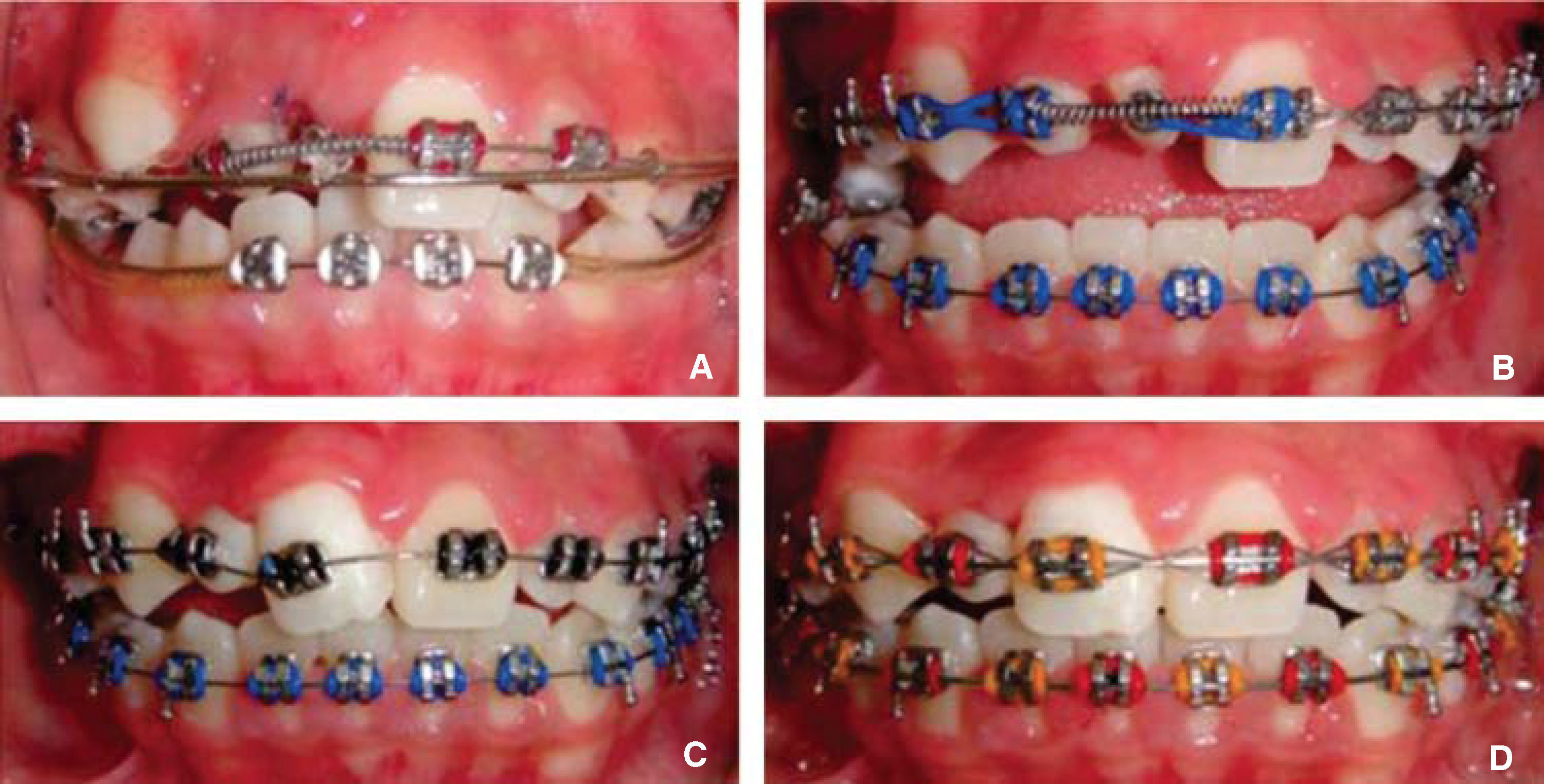
RESULTSThe patient's multidisciplinary treatment was divided in three phases: Phase 1 consisted in periodontal surgery for exposing the retained upper central incisor (Figure 3); Phase 2 in which traction of the retained incisor was performed through elastics and accessory archwires and the teeth were brought to an ideal position in order to establish a good occlusal settling as well as anterior guidance (Figure 4); and phase 3 in which preparations of the microdontic teeth were completed for placing ceromer crowns (Figure 5).14,15
 surgical flap, B) enamel conditioning with etching acid, C) placement and polymerization of the lingual button for traction, D) The flap is repositioned.")
 Accesory arch 0.032” SS. B) Placing occlusal stops in order to avoid occlusal interference. C) Brace placing on the tooth to its correct level. D) Tooth in its final position.")

Approximate rehabilitation treatment time was 2 weeks in the Periodontics area, 24 months in Orthodontics and 1 month in Oral Prosthetics summing a total of 25 months overall rehabilitation time for a patient with microdontia of the upper lateral incisors and retention of the upper central incisor (Figure 6).16,17
DISCUSSION Initial. B) Final.")
For deciding the treatment plan, the Journal of Orthodontics database was searched for patients with retention of the upper anteriors and treatment alternatives for microdontic teeth; each anomaly was searched separately and combined.
In the consulted articles it was found that dental retention is very frequent. Authors such as Johnston, McDonald, Proffit, Sapp among others have determined that the upper right canine is the tooth that most frequently becomes retained in the maxilla.1,13,14 However, other authors such as Tanaka, Figueredo and Vermette join other authors in stating that the upper right central incisor is the least frequent dental retention.9,10,15 This may be due to different anomalies in maxillary growth, tooth eruption guide deviation because of supernumerary teeth, premature loss of a deciduous tooth as well as trauma.
In the case report hereby presented, taking into consideration the patient's clinical records we might venture that the dental retention that the patient presented was caused possibly by the premature loss of the deciduous tooth which consequently caused mesialization of the adjacent teeth. This presumption was based on studies conducted by authors such as Kokich that tell us that when a deciduous tooth is lost prematurely, the permanent tooth's eruption guide may result affected.
Upon searching for orthodontic treatment alternatives for teeth with microdonthia in the literature, it was difficult to find case reports, but it was found that microdonthia is the most frequent shape anomaly in the permanent dentition. Authors such as Sapp, Eversole and Schulze support this statement.
Regarding alternatives for dental retention, surgical treatment is the treatment of choice either for the retained tooth's exposure and subsequent extraction or when possible, for orthodontic traction through different materials and attachments to bring it to the dental arch. Traction attachments may range from the simplest to the most complex ones with materials such as elastomeric thread, ligature wire, elastomeric chains among others. On this patient it as decided to perform a surgical exposure and orthodontic traction by placing a bondable lingual button aided by elastomeric thread since the tooth did not require a heavy amount of force for traction. The adjacent tooth was interfering with the orthodontic traction so first space had to be obtained.
Regarding the treatment of the teeth with microdonthia it was performed with esthetic and occlusal stability goals. Rehabilitation of the teeth with microdonthia was required either with veneers or crowns since once the canines were moved distally, spaces would open in the anterior area. Due to the patient's age (10 years old), different authors have determined that final dental restorations should be performed once occlusion has been established. This occurs in the adult age, approximately, around 18 years of age once every tooth has erupted in the oral cavity. In this case, temporary but highly esthetic restorations were placed, with good dimensional stability as well as resistance to masticatory forces.
Orthodontically, there are no reports of combined treatments of dental retention and microdonthia so the treatment stages were determined as three: Phase 1: surgical treatment, Phase 2: orthodontic traction of the retained tooth and stablishment of the canine guidance, occlusal settling as well as a normal overbite and overjet; and stage 3, prosthetic rehabilitation upon appliance removal.
CONCLUSIONSA good diagnosis will provide a high-quality interdisciplinary team work in order to perform a more precise treatment according to the characteristics and needs of the patient so as to achieve better esthetic, functional, periodontal and articular health results.
Interconsultation must be performed before beginning any kind of treatment. By doing so, we may assess the best therapeutic decisions and offer diverse alternatives for the patient's treatment.
Interdisciplinary work in the dental health areas such as Orthodontics, Periodontics and Dental Prosthetics becomes an optimal combination for the overall rehabilitation of patients who present skeletal, dental and joint problems was well as esthetic and functional ones.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia