



Main objective: To compare the effectiveness for checking surgical margins between SPECT-portable and mammography of the piece (RxM).
Secondary objectiveTo standardize a pre-operative protocol using SPECT-portable and to evaluate the time required in the use of this technique.
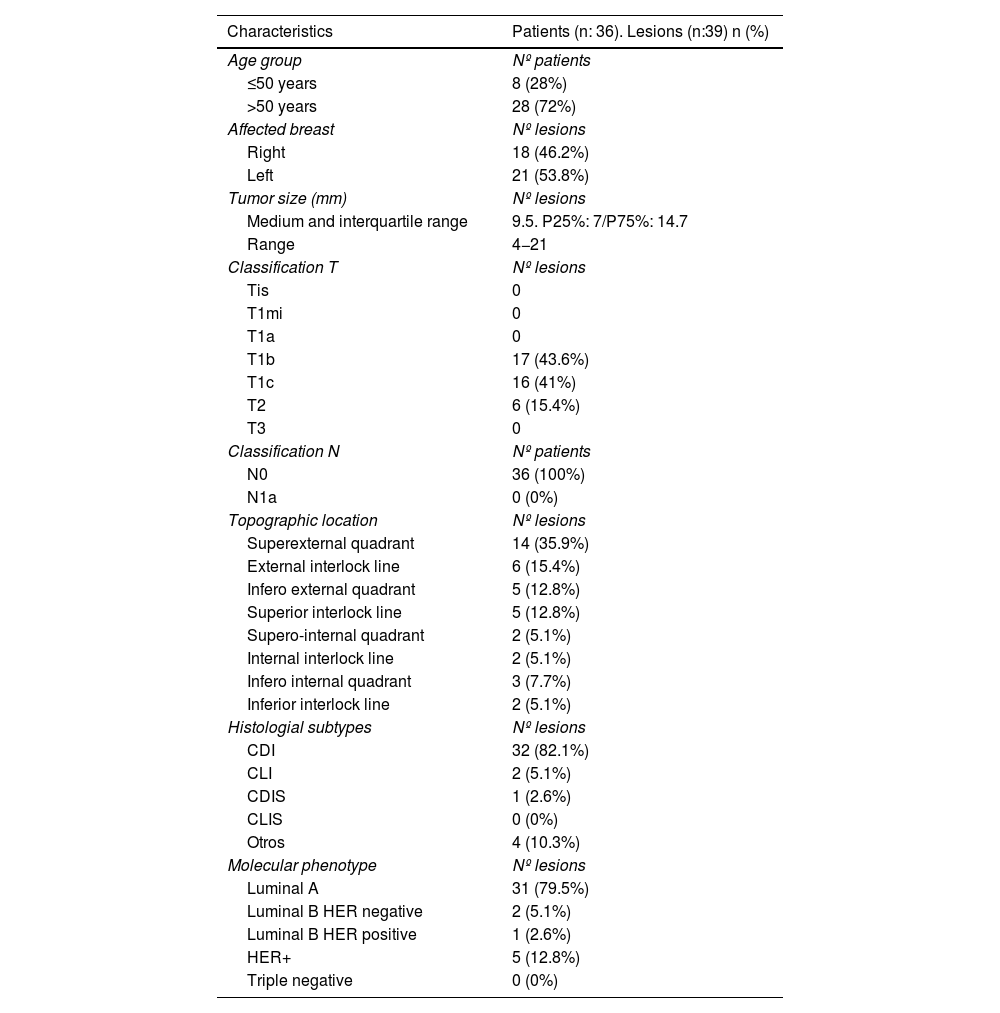
Material and methodsProspective longitudinal study with 36 patients (39 lesions) diagnosed with breast cancer (CM) with criteria for SNOLL/ROLL.
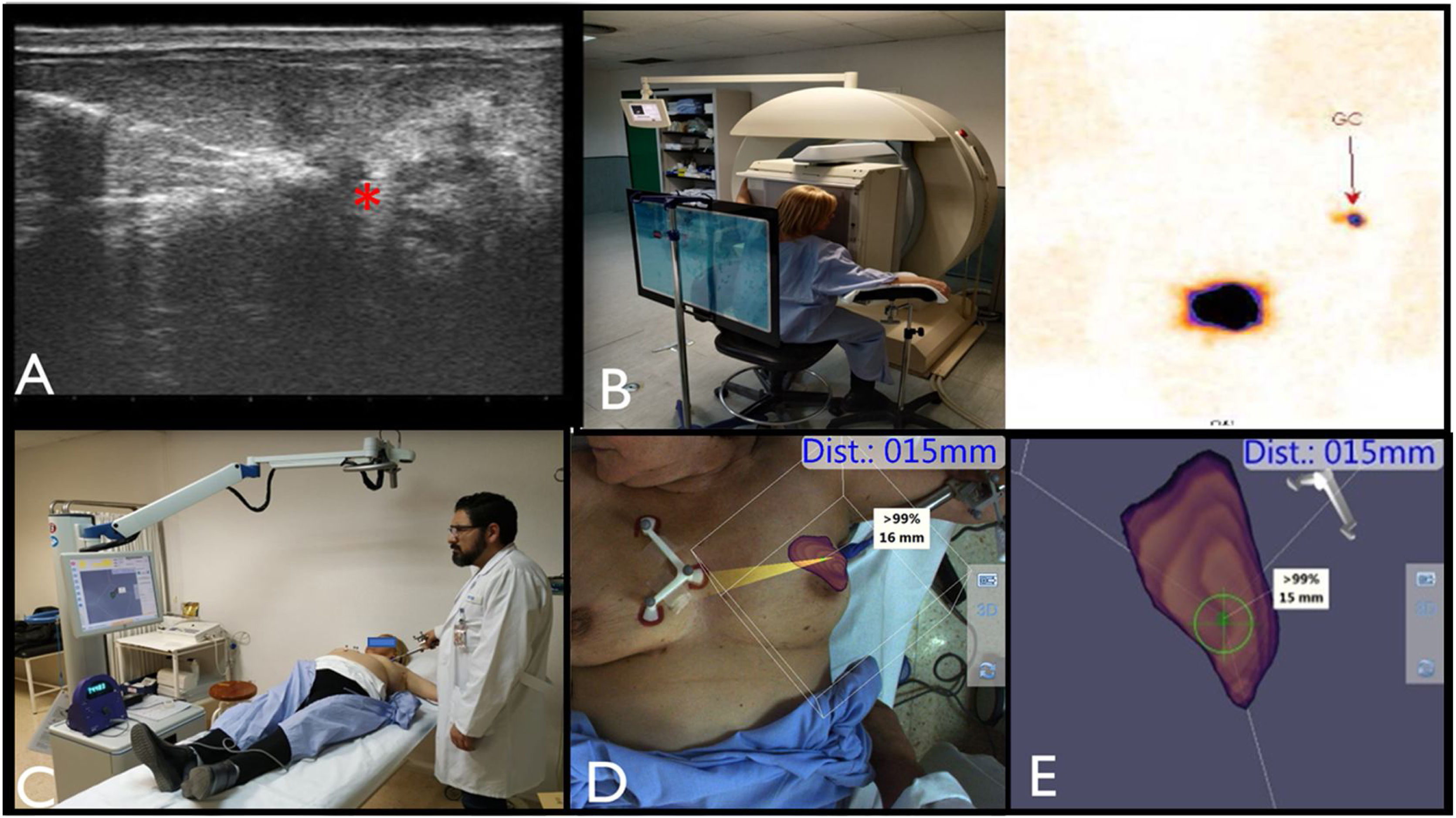
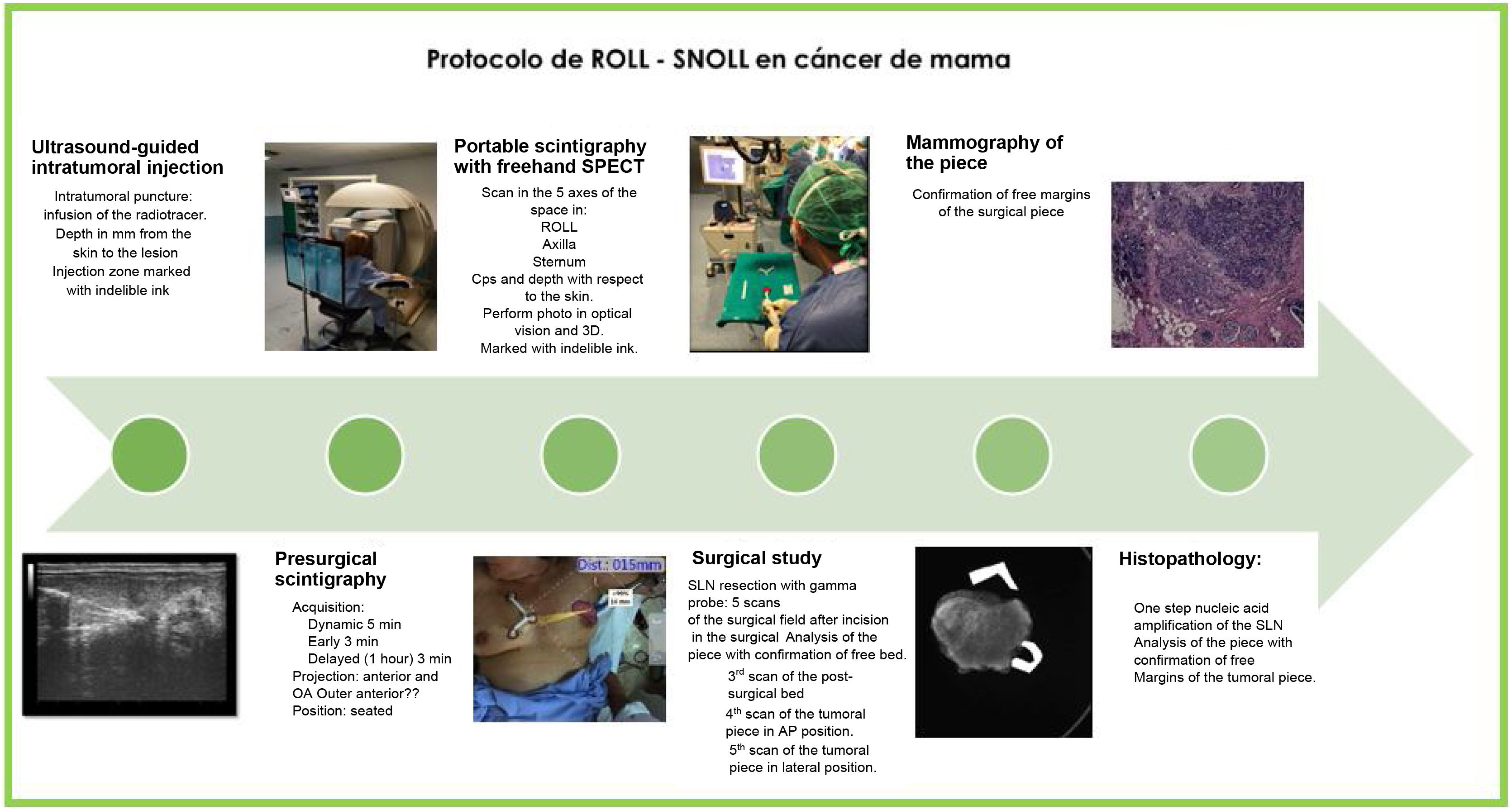
A pre-surgical study of the tumor lesion was performed, after the eco-guided administration of 99mTc-nanocolloids of albumin/99mTc-macroaggregates of albumin, in the tumor lesion. Hybrid images (optical + SPECT) and 3D navigation images with gamma probe are obtained using freehandSPECT.
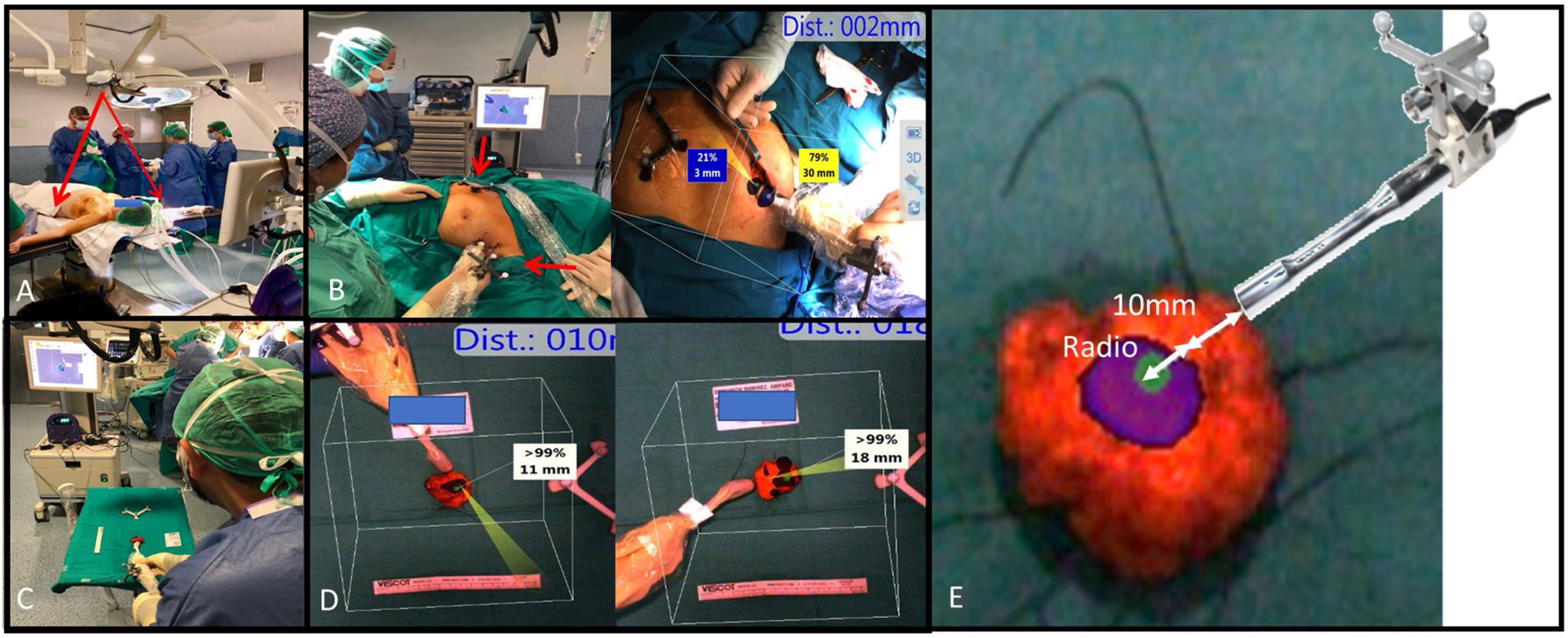
In the operating room, 4–5 images are obtained with freehandSPECT, (I) on skin for tumor location, (II) after exposure of surgical bed for resection guide, (III) of the surgical bed after exeresis, (IV and V) the anterior–posterior and lateral surface of the surgical specimen. The three criteria to decide to extend the margins are: (a) residual activity (cps) at the edges of the surgical bed resection; (b) visual analysis of the uptake in the specimen; (c) a minimum distance of 10 mm from the edges of the specimen to the center of greatest uptake, plus the radius of the lesion.
We study the concordance of: the depth measurement between ultrasound and freehandSPECT; the surgical margins between freehandSPECT vs. mammography of the specimen (RxM), considering anatomical pathology (AP) as the gold standard technique as reference; surgical time used with freehandSPECT and RxM.
ResultsIntraoperative localization was performed in all cases.
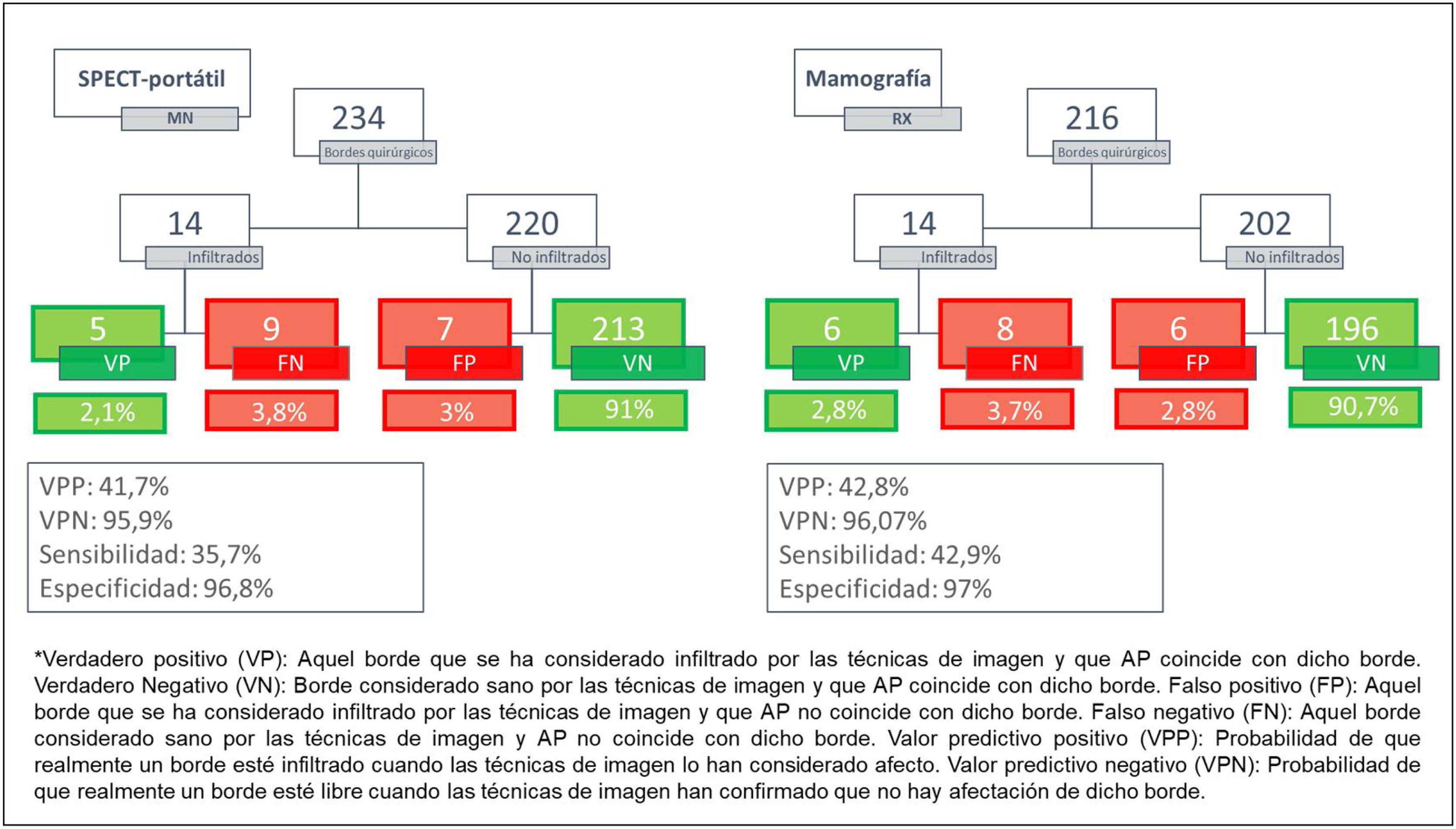
False negative (FN: no detection margin affected) with freehandSPECT: 9 margins; with RxM: 8. True positive (TP: detection margin affected) with freehandSPECT: 5 margins, with RxM: 6. True negative (TN: consider free margin when healthy) with freehandSPECT: 213 margins; with RxM: 196. Negative predictive value (NPV: probability of negative margin on unaffected part) with freehandSPECT: 95.9%, with RxM: 96.07%. Specificity with freehandSPECT: 96.8%, with RxM: 97%.
The concordance of surgical bed margins between freehandSPECT and RxM: 94.5%. Between freehandSPECT and AP: 93.1%. Between RxM and PA: 93.5%, being all statistically significant (p-value <0.000), so we can affirm that both techniques are related or dependent on the reference technique, the PA. Degree of correlation between SPECT-portable and low PA (Kappa index: 0.34, 95% CI [0.22–0.47], and between RxM and moderate PA (Kappa index: 0.42, 95% CI [0.29–0.56], p-value <0.001. Comparison of the successes and failures of both techniques (SPECT-portable and RxM) and PA: Distribution χ2: 0.023 with degree of freedom 1, with value <0.05, so we can affirm that both techniques are similar, since there are no significant statistical differences.
Median total OR time: 60.25 min (30–145). Mean freehandSPECT OR time: 5 scans = 10 min.
ConclusionsThere are no statistically significant differences in the probability to rule out affective margins that require a second surgery between both techniques (SPECT-portable and RxM) so, the technique performed with SPECT-Portable is a useful and effective procedure, which requires specific training with an optimized and multidisciplinary protocol. The time spent with SPECT-portable is feasible for daily practice.
Objetivo principal: comparar la efectividad para la comprobación de márgenes quirúrgicos entre SPECT portátil y la mamografía de la pieza (RxM).
Objetivo secundarioestandarizar un protocolo preintraquirúrgico mediante SPECT portátil y evaluar el tiempo requerido en el uso de esta técnica.
Material y métodosEstudio longitudinal prospectivo con 36 pacientes (39 lesiones) diagnosticadas de cáncer de mama con criterios para realización SNOLL/ROLL. Se realiza en estudio prequirúrgico de la lesión tumoral, tras la administración ecoguiada de [99mTc]Tc-nanocoloides de albúmina/[99mTc]Tc-macroagregados de albúmina, en la lesión tumoral. Mediante SPECT portátil se obtienen imágenes híbridas (óptico + SPECT) e imágenes de navegación en 3D con sonda gamma.
En quirófano se obtienen 4–5 imágenes con SPECT portátil, I) sobre piel para localización tumoral II) tras exposición de lecho para guía de resección, III) del lecho tras exéresis, IV y V) a la pieza quirúrgica. Se decide ampliación o no de márgenes considerando tres criterios: a) actividad residual (cps) en bordes de resección del lecho; b) análisis visual de la captación en la pieza; c) una distancia mínima de 10 mm de los bordes de la pieza hasta el centro de mayor captación, más el radio de la lesión.
En este estudio se valora la concordancia de: la medición de la profundidad entre ecografía y SPECT portátil en el estudio prequirúrgico; los márgenes quirúrgicos entre SPECT portátil vs. RxM, teniendo de técnica de referencia anatomía patológica (AP); del tiempo quirúrgico empleado con SPECT portátil.
ResultadosLocalización intraquirófano: se realizó en todos los casos.
El análisis de los resultados se realiza por cada uno de los bordes de cada lesión tumoral por separado. Falso negativo (FN: no detección borde afecto) con SPECT portátil: 9 bordes; con RxM: 8. Verdadero positivo (VP: detección borde afecto) con SPECT portátil: 5 bordes, con RxM: 6. Verdadero negativo (VN: considerar borde libre cuando es sano) con SPECT portátil: 213 bordes; con RxM: 196. Valor predictivo negativo (VPN: probabilidad de borde negativo en pieza sin borde afecto) con SPECT portátil: 95,9%, con RxM: 96,07%. Especificidad con SPECT portátil: 96,8%, con RxM: 97%.
Concordancia de bordes de pieza quirúrgica entre SPECT portátil y RxM: 94,5%. Entre SPECT portátil y AP: 93,1%. Entre RxM y AP: 93,5%, todo ello siendo estadísticamente significativo (p valor < 0,001). Grado de correlación entre SPECT portátil y AP bajo (índice Kappa: 0,34 IC95% [0,22-0,47] y entre RxM y AP moderado (índice kappa: 0,42 IC95% [0,29−0,56], con p valor < 0,001. Confrontación de los aciertos y los fallos de ambas técnicas (SPECT portátil y RxM) y AP: distribución χ2: 0,023 con grado de libertad 1, con p-valor < 0,05, por lo que podemos afirmar que ambas técnicas son similares, ya que no hay diferencias estadísticas significativas.
Mediana de tiempo total en quirófano: 60,25 minutos (30–145). Tiempo medio de uso SPECT-portátil intraquirófano: 5 rastreos = 10 minutos.
ConclusionesNo hay diferencias estadísticamente significativas en la probabilidad para descartar márgenes afectos que requieren una segunda cirugía entre ambas técnicas (SPECT portátil y RxM) por lo que, la técnica realizada con SPECT portátil es un procedimiento útil y efectivo, que requiere un entrenamiento específico con un protocolo optimizado y multidisciplinar. El tiempo empleado con SPECT portátil es viable para la práctica diaria.
Article
Revista Española de Medicina Nuclear e Imagen Molecular (English Edition)
