




The absence or hypoplasia of the carpal scaphoid bone is rare and unfrequent, especially if isolated, as it is usually associated with other congenital disorders. Such anomaly is usually the result of fetal development alterations before week 11 of pregnancy. We introduce the case of a 53-year-old woman with chronic wrist pain and persistent pain after surgical intervention of the carpal tunnel syndrome in the left hand. X-rays and CT confirmed the patient’s hypoplasia of the scaphoid bone with carpal instability diagnosis. The patient became asymptomatic after surgical intervention and post-surgical rehabilitation.
La ausencia e hipoplasia del escafoides carpiano es una entidad rara e infrecuente, y aún más si se da de forma aislada, pues suele aparecer asociada a otros síndromes congénitos. Suele ser debida a una alteración en el desarrollo fetal antes de la semana 11 del embarazo. Presentamos el caso de una mujer de 53 años, con dolor crónico de muñeca, intervenida de síndrome del túnel del carpo izquierdo, con persistencia de dolor tras la intervención. Las radiografías y la TC permitieron realizar el diagnóstico definitivo, evidenciando la existencia de una hipoplasia escafoidea con inestabilidad carpiana. Tras el tratamiento quirúrgico y la realización de tratamiento rehabilitador postquirúrgico la paciente quedó asintomática.
The complex anatomy of the hand, and mainly of the wrist, makes this functional unit a site for numerous, sometimes little known, injuries. The wrist is made up of bony structures reinforced by small musculo-ligamentous components that enable the biomechanical stability of its various joints (Figs. 1 and 2).

.")
Absence or hypoplasia of the carpal scaphoid bone is rare and infrequent, and even more so if it occurs in isolation, as it is usually associated with other structural anomalies or congenital syndromes.1–4 Aplasia or hypoplasia of the thumb, the thenar musculature or other bones of the carpus or forearm are some of the associated developmental abnormalities of the upper limb described in the literature.2,4 The condition may also appear in VACTERL syndrome (vertebral defects, anal atresia, cardiac anomalies, tracheoesophageal fistula, radial and renal anomalies, and other limb disorders) or in Holt–Oram syndrome (associated skeletal upper limb abnormalities and cardiovascular abnormalities), among others.2,5
Its aetiopathogenesis is very varied. It may be due to spontaneous mutations (85%–90%) or be the result of hereditary genetic factors. Environmental agents, infectious agents or dietary disturbances during gestation may be the cause.6,7
It is known that the outline of the upper limbs is visible at 4 weeks, during the embryogenesis period, and by 8 weeks the process is complete, and all limb structures are present.6,7 By the time pregnancy is diagnosed most abnormalities have already been generated.7 These congenital abnormalities occur in 1%–2% of all live newborns, with 10% affecting the upper limbs.7 Approximately half the cases are bilateral and are associated with various malformations.6
Various classifications have been made of congenital upper limb abnormalities; isolated scaphoid hypoplasia does not appear in any category.2,4,5,8 The classification of the International Federation of Societies for Surgery of the Hand, based on that of Swanson, is currently the most widely used and establishes 7 groups: I) failure of formation; II) failure of differentiation; III) polydactyly; IV) overgrowth; V) undergrowth; VI) amniotic band syndrome; and VII) generalised skeletal syndromes. Aplasia or hypoplasia of the scaphoid bone is always associated with thumb deficiencies and is included in the first group (developmental failure with longitudinal arrest and radial deficiency).2,9
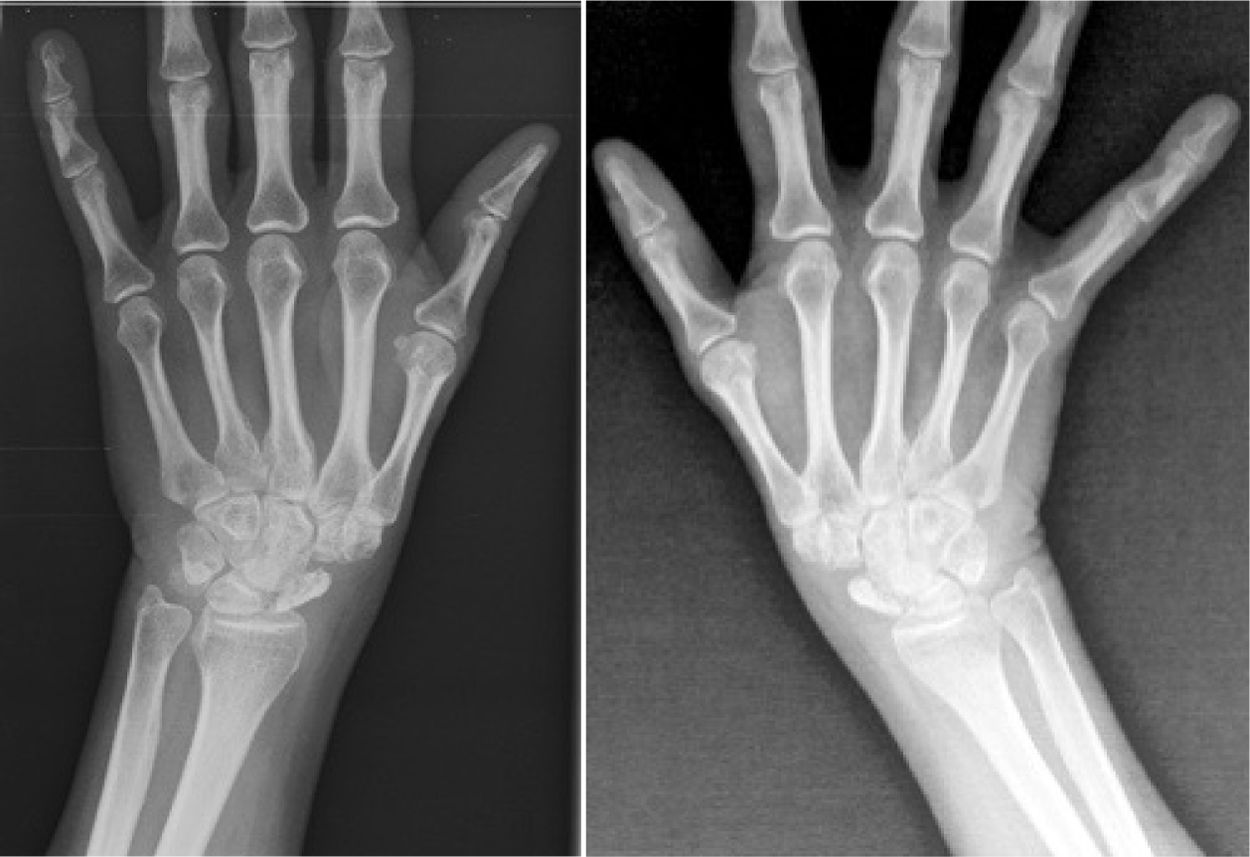
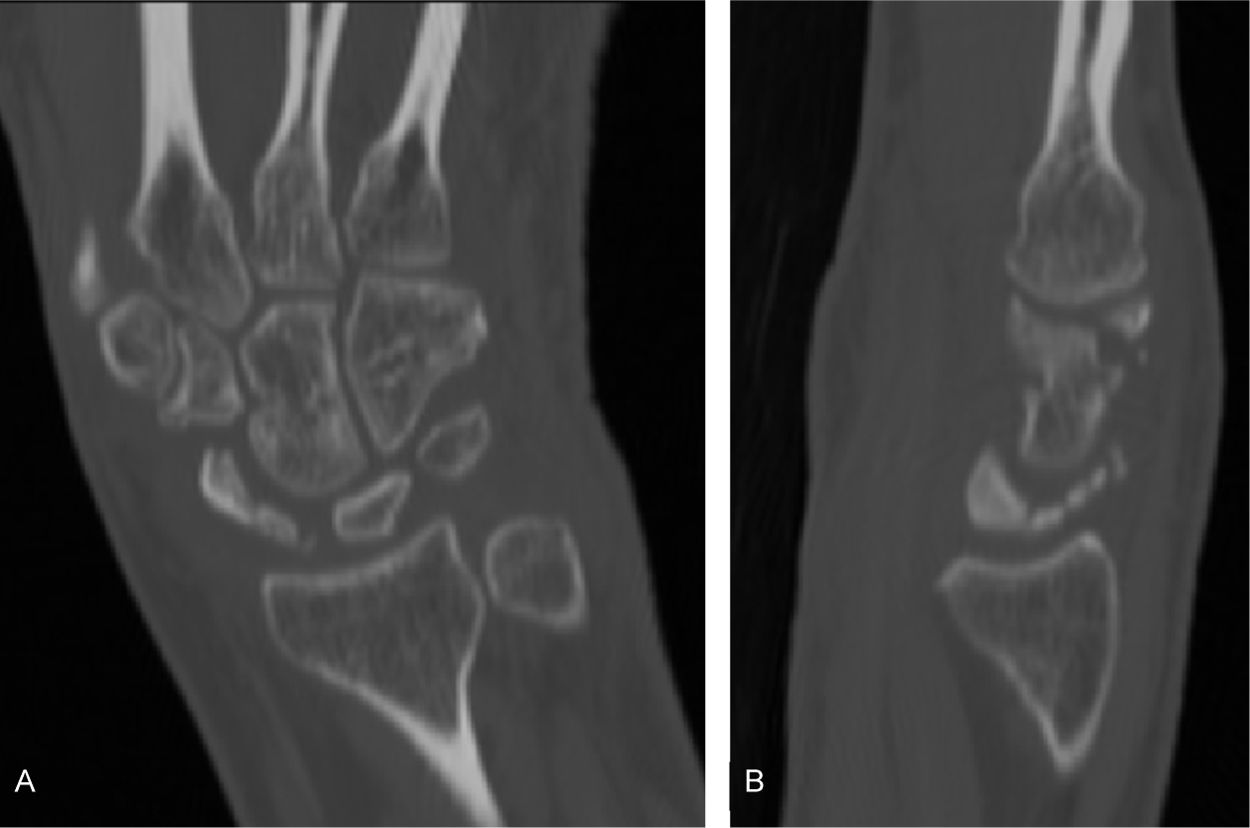
Clinically, the condition is tolerated well until onset of symptoms, as most cases are described in adulthood. X-ray and CT scan allow definitive diagnosis. Surgical treatment is indicated if symptoms are persistent and painful (Fig. 3).

We present the case of a 53-year-old woman, referred to our clinic for pain in the left wrist of 2 years’ duration, with no previous trauma. She had a history of exoneurolysis of the left median nerve 5 months previously due to carpal tunnel syndrome confirmed in a neurophysiological study, the neurological symptoms (paraesthesia in the first, second and third fingers of the left hand, predominantly at night) disappeared but she had persistent pain in the carpus after the operation. Examination revealed a scar on the volar aspect of the left wrist, which was neither adherent nor painful. Mild amyotrophy was observed in the bilateral thenar eminence, with preserved abduction and opposition of the thumb. There was no sensory disturbance. Tinel’s and Phalen’s signs were negative. She reported mechanical pain in the radial border of the left wrist with decreased joint range. No skin alterations or structural abnormalities in the upper limbs. A slaughterhouse worker by profession with left-hand dominance, and no other personal or family history of interest.
The radiological study revealed bilateral hypoplasia of the carpal scaphoid bone. CT scan of the left wrist showed a multi-fragmented, sclerosed and partially collapsed scaphoid. Dorsal subluxation of the lunate and an increase in the scapholunate distance were observed as indirect signs of probable carpal instability (DISI). The patient was assessed by the orthopaedic department and surgical treatment was decided, but only on the symptomatic side. After arthroscopic excision of the scaphoid remnant, the patient started rehabilitation treatment. During the postoperative phase of wrist immobilisation, active mobilisation exercises at home of the shoulder, elbow, and fingers (except the thumb) were prescribed to avoid joint contractures and stiffness. After removal of the forearm splint, active and self-assisted wrist flexion-extension and pronosupination exercises, proximal and distal hand closure manoeuvres and thumb opposition, and the start of isometric muscle work were introduced. From the third month onwards, proprioception exercises and strengthening of the muscles of the radial aspect of the wrist were added to promote carpal stability. The patient recovered joint range and strength and remains asymptomatic.
DiscussionCongenital malformations of the upper limb, and especially those of the wrist-hand functional unit, vary greatly, ranging from small skeletal abnormalities with little aesthetic-functional repercussion to large abnormalities or more disabling congenital malformation syndromes.3 Hypoplasia or agenesis of the scaphoid bone is very rare. It usually occurs together with other congenital anomalies such as hypoplasia of the thumb, radial hemimelia, absence of sesamoid or hypogenesis of the thenar or forearm muscles. Congenital syndromes include VACTERL, Holt–Oram syndrome and TAR syndrome (thrombocytopenia-absent radius).2,4,5 It is an entity possibly associated with a foetal development abnormality before the 11th week of pregnancy and its presentation in isolation, as in the patient in the case presented, is even rarer.3
Kuz and Smith1 published the case of an 18-year-old man with isolated absence of the right carpal scaphoid bone and hypoplasia of the left, and although radiological assessment also showed slight changes in the relationships of the rest of the carpal bones and discrete alteration in the morphology of the trapeziometacarpal joint, they argue that these changes are a biomechanical adaptation of the carpus. In our case, we believe that the lunate subluxation and increased scapholunate distance accompanying the morphological alterations of the carpal scaphoid bone were also due to functional readaptation and were not just another congenital abnormality. Gómez Fernández et al.2 present the first case of unilateral congenital absence of the scaphoid with dysplasia of the large bone, accompanied by hypoplasia of the trapezium and radial styloid and compensatory changes in the carpus. The 49-year-old patient reported chronic mild wrist pain and paraesthesia in the median nerve territory, flattening of the thenar eminence and limitation of joint balance. Electromyography detected severe neuropathy of the median nerve due to compression in the carpal tunnel, which was surgically released, resulting only in improvement of neuropathic symptoms. The authors of this paper do not consider that the compression of this nerve in the carpal tunnel originates in the absence of the scaphoid bone due to secondary narrowing of the tunnel, since if this were the case, the process would begin earlier clinically. In the case described, the patient also had carpal tunnel syndrome together with hypoplastic scaphoid, of late clinical onset, and although Radford and Matthewson10 suggested a possible causal relationship between hypoplastic scaphoid and carpal tunnel syndrome in a 15-year-old patient also associated with bilateral distal radial dysplasia, they found no description associating these diseases. Therefore, we consider that the skeletal abnormalities presented by the patient would not have caused her nerve compression either.
On the other hand, isolated absence or hypoplasia of the scaphoid is a condition tolerated well throughout life, which does not cause pain or functional limitations, despite the harmonious adaptation of the rest of the carpal bones, until adulthood.2 We believe that left dominance and the work carried out by the patient over the years may have affected the onset of painful symptoms unilaterally due to functional overload, causing a change in the transmission of forces in a structurally and biomechanically altered carpus. In our case, as also occurred in most of the clinical cases published, surgical treatment was only performed when symptoms were not controlled with conservative treatment, and the scaphoid was excised by arthroscopic surgery.
As potential complications, Panciera and Le Viet5 describe carpal collapse and degenerative arthritis in a 45-year-old man with wrist pain of 6 months' duration, who associated mild hypoplasia of the radial styloid with scaphoid hypoplasia. He required wrist arthrodesis with autogenous bone grafting due to the advanced state of the process. However, they only found one case in the literature with scaphoid anomaly and carpal collapse that eventually developed osteoarthritis. We have found no publications to support this possible causal relationship.
There are many factors that can cause wrist pain and it can be difficult to diagnose the exact cause, but an accurate diagnosis is essential to establish treatment. We consider this case to be of interest as it is exceptional in our practice, as is the necessary genetic follow-up in these patients.
Level of evidenceLevel of evidence iii.
Please cite this article as: V. Gallart Úbeda, R. Puerta de Diego and J.M. Elía Martínez, Dolor crónico de muñeca. Hipoplasia de escafoides carpiano, Rev Esp Cir Ortop Traumatol. 2021;65:382–385.
