





Osteoarticular infections represent a major complication in orthopaedic surgery. The aim is to identify the percentage of suction cannulas colonised and to determine the relationship between the time they are used in surgery and the colonisation of these cannulas.
Materials and methodsDescriptive and prospective study that analysed 546 suction cannulas used in clean orthopaedic surgery in a trauma centre, between November 2017 and March 2018. The distal end of the cannula was cultured to determine the colonisation rate.
Results7.3% of the cultured cannulas were positive for pathogens, the most frequent being Staphylococcus epidermidis at 27.5%. In addition, an association was found between colonisation and the length of time the cannula was used. The possibility of colonisation of cannulas used for between 60min or more, is greater than those used for less than 60min; between 60 and 90min the possibility is twice as high OR=2.2 (95% CI 1.1–4.1) and in cannulas used for more than 90min it is 8 times higher OR=8.49 (95% CI 1.77–40.86).
ConclusionsThe colonisation rate of cannulas is lower than reported in the literature. The longer the cannula is used in surgery increases the risk of their colonisation. Follow-up studies are being considered to determine whether suction cannula colonisation is associated with increased postoperative infection.
Las infecciones osteoarticulares representan una complicación mayor en cirugía ortopédica. Se pretende identificar el porcentaje de cánulas de succión colonizadas y determinar la relación entre el tiempo de uso en cirugía y la colonización de estas.
Materiales y métodosEstudio descriptivo y prospectivo que analiza 546 cánulas de succión utilizadas en cirugía ortopédica limpia en un centro de trauma, entre noviembre del 2017 a marzo del 2018. El extremo distal de la cánula fue cultivado para determinar la proporción de colonización.
ResultadosEl 7,3% de las cánulas cultivadas tuvieron cultivos positivos para gérmenes patógenos, de los cuales el más frecuente fue Staphylococcus epidermidis con 27,5%. Además, se encontró asociación entre la colonización y el tiempo de uso de la cánula. La posibilidad de colonización de cánulas usadas entre 60 minutos o más, es mayor que en las que se usaron menos de 60 minutos; entre 60 y 90 minutos la posibilidad es dos veces mayor OR=2,2 (IC:95% 1,1-4,1) y en las cánulas usadas por más de 90 minutos es 8 veces mayor OR=8,49 (IC:95% 1,77-40,86).
ConclusionesLa proporción de colonización de las cánulas es menor a lo reportado en la literatura. El mayor tiempo de uso de la cánula en la cirugía aumenta el riesgo de la colonización de estas. Se considera realizar estudios de seguimiento para determinar si la colonización de las cánulas de succión se asocia a un incremento de infección postoperatoria.
Surgical site infection (SSI) in orthopaedic and trauma surgery is one of the most dreaded complications in this surgical area due to the high percentage of implants used, which hinder management and on many occasions removal of them is required to control the infection.
SSI generate high rates of mortality, long-term disability and prolonged hospital stays which impact quality of life and increase health system costs.1,2
Considerable advances have been made to mitigate the risk of infections associated with healthcare. These include less invasive surgical techniques, the use of prophylactic antibiotics and preoperative sterile measures.3 However, according to the Centre for Disease Control and Prevention infections associated with healthcare continue being one of the most common adverse events relating to health service provision.2 SSI are the second most notable type of adverse event in the world, presenting in approximately 14% of hospitalised patients and in 38% of patients who undergo surgery,1 with an associated mortality rate of 3%.3
Suction cannulas are used as an everyday tool in the great majority of orthopaedic surgery, since they enable visualisation of the operative field. However, some authors consider that the continuous airflow through the end of the suction cannula (which in most operations suctions continuously during the whole procedure) may generate a site of turbulence and encourage the attachment of microorganisms at this level, which would result in the production of a SSI.4 In their studies authors such as Strange-Vognsen et al., in 1988,5 and Givissis et al., in 2008,6 reported a contamination rate of 54% in the suction cannulas used in orthopaedic procedures with isolation in the cultivated cannula end with different types of Staphylococcus. In theory, this colonisation of the suction cannula end could be linked to the rate of surgical site infections in the patient but available publications are controversial and there has not yet been any scientific evidence to confirm this hypothesis.
This study was conducted with the aim of determining the percentage of suction cannulas colonised during orthopaedic operations of an institution specialising in trauma, to identify the contaminating microorganisms and establish the pre-and-intraoperative factors which may have been associated with colonisation. The intention was to generate new future studies which would finally assess the clinical outcome of patients with colonised cannulas and their association with the rate of SSI.
Materials and methodsA descriptive, prospective study which analysed 546 results from microbiological cultures of suction cannula ends used in clean orthopaedic operations of arthroplasties and osteosyntheses performed in a centre specialising in orthopaedics in the city of Barranquilla, northern Colombia, between November 2017 and March 2018.
Inclusion criteria were all cultures from suction cannulas which had been used in clean orthopaedic operations. Cannulas used in open fracture procedures were excluded, as were those from operations on limbs with extensive involvement, operations with more than one fracture in the same limb and cases which presented with a history of previous infections.
Suction cannula analysis was performed immediately after the operation by cutting off the distal end of the disposable plastic cannula, which was then sent to the clinical laboratory in a sterile vial and marked with a code for follow-up of the case. The clinical laboratory processed the specimen by adding a fluid enriched with thioglycolate for 2–4h and then putting it into different media: blood agar, chocolate agar and MacConkey agar. It was incubated at 37°C and the results were assessed after 24 and 48h. In positive cases the germ and antibiogram were identified using the automated VITEK®2 Compact (bioMerieux, Hazelwood, U.S.A.).
Several variables were taken into account, including age, sex and surgical factors such as antibiotic prophylaxis, mean time in surgery in minutes from the moment the incision was made until its closure, volume of blood measured in cubic cm (cc), volume of irrigation in (cc), time in minutes of suction cannula use from the beginning of the surgery until it was decided suction should be terminated in the intraoperative period, and any surgical complications arising.
Information was processed with the SPSS statistical package version 25. Descriptive analysis consisted in calculating frequency measures, central tendency and dispersion. The factors associated with cannula colonisation were calculated using simple binary logistic regression. Once identified, the strength of association of each of these factors was measured using a multivariate logistic regression model. The level of significance used was .05.
This research study was approved by the hospital ethics committee and conducted in accordance with the regulations established in Resolution 8430 of 1993 of the Ministry of Health of Colombia; it was classified as a “non risk” study.
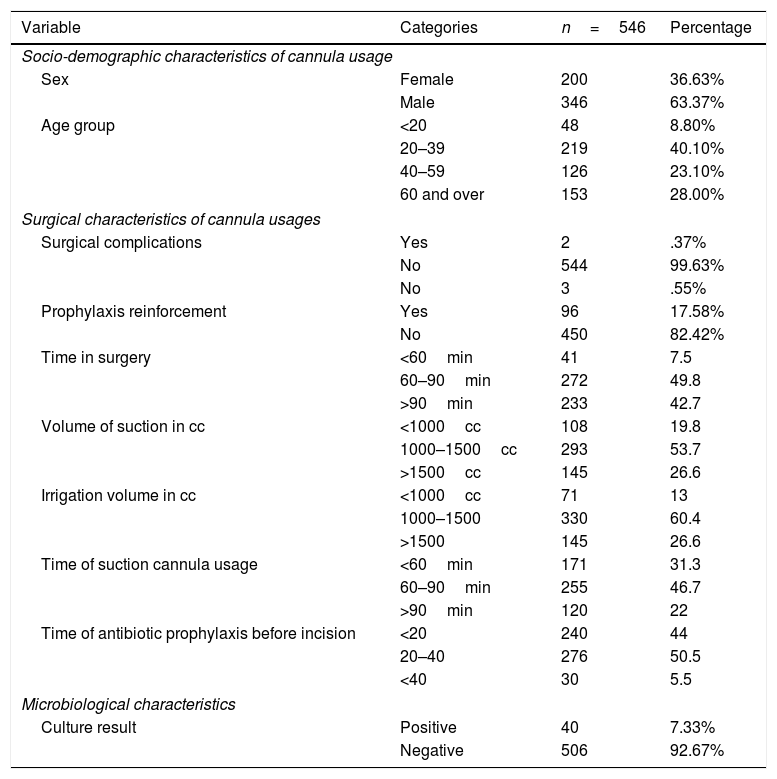
ResultsThe results of the culture tests of 546 suction cannulas were analysed, corresponding 546 patients who underwent clean orthopaedic operations, including those of osteosynthesis and articular replacements. In Table 1 it may be observed that 36.63% of the cannulas corresponded to female patients and 63.37% to male, with the most common age range being between 20 and 39 years (40.1%). Positive cultures were obtained in 40 cases (7.3%), from which the most frequently isolated microorganism was Staphylococcus epidermidis (S. epidermidis) (27.5%), followed by Staphylococcus aureus (S. aureus) (12.5%) and Enterobacter cloacae (E. cloacae) (10.0%) (Fig. 1).
Description of the socio-demographic, surgical and microbiological characteristics.
| Variable | Categories | n=546 | Percentage |
|---|---|---|---|
| Socio-demographic characteristics of cannula usage | |||
| Sex | Female | 200 | 36.63% |
| Male | 346 | 63.37% | |
| Age group | <20 | 48 | 8.80% |
| 20–39 | 219 | 40.10% | |
| 40–59 | 126 | 23.10% | |
| 60 and over | 153 | 28.00% | |
| Surgical characteristics of cannula usages | |||
| Surgical complications | Yes | 2 | .37% |
| No | 544 | 99.63% | |
| No | 3 | .55% | |
| Prophylaxis reinforcement | Yes | 96 | 17.58% |
| No | 450 | 82.42% | |
| Time in surgery | <60min | 41 | 7.5 |
| 60–90min | 272 | 49.8 | |
| >90min | 233 | 42.7 | |
| Volume of suction in cc | <1000cc | 108 | 19.8 |
| 1000–1500cc | 293 | 53.7 | |
| >1500cc | 145 | 26.6 | |
| Irrigation volume in cc | <1000cc | 71 | 13 |
| 1000–1500 | 330 | 60.4 | |
| >1500 | 145 | 26.6 | |
| Time of suction cannula usage | <60min | 171 | 31.3 |
| 60–90min | 255 | 46.7 | |
| >90min | 120 | 22 | |
| Time of antibiotic prophylaxis before incision | <20 | 240 | 44 |
| 20–40 | 276 | 50.5 | |
| <40 | 30 | 5.5 | |
| Microbiological characteristics | |||
| Culture result | Positive | 40 | 7.33% |
| Negative | 506 | 92.67% | |

Fig. 2 shows that the most common operations were osteosynthesis of the distal radial metaphysis (17.77%), followed by osteosynthesis of the tibial saucers (8.42%) and osteosynthesis in the hand (6.59%). 100% received antibiotic prophylaxis with 1g of intravenous cefalexin, which was administered between 20 and 40min prior to surgical incision. The majority of the operations (49.8%) lasted between 60 and 90min and in 46.7% of them the cannulas were used between 60 and 90min.

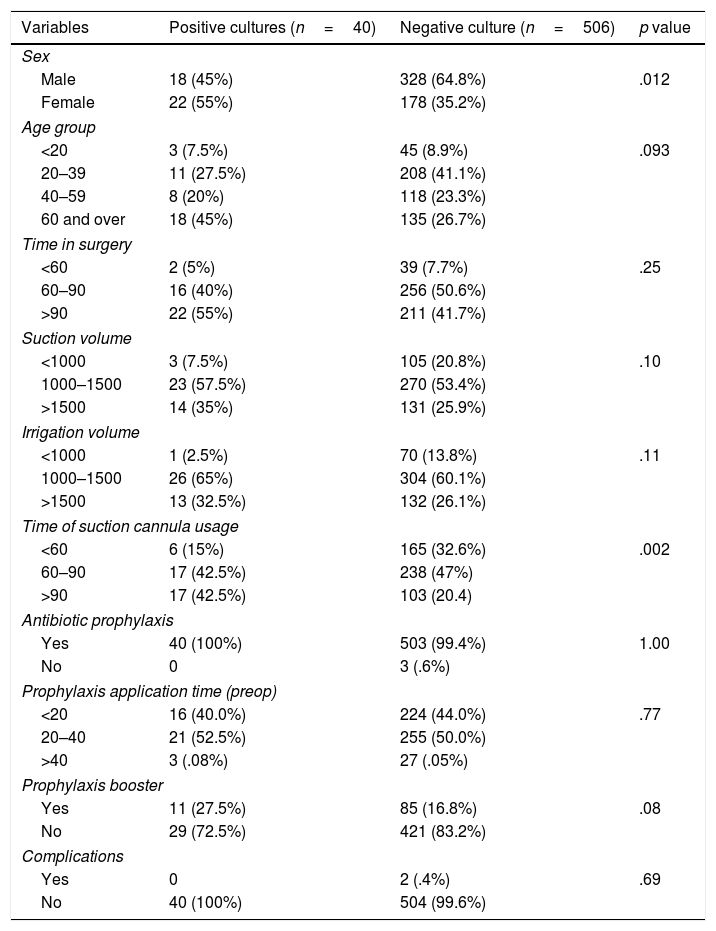
Table 2 shows the bivariate analysis where the groups with suction cannulas, with and without positive colonisation, were compared. We observed a higher proportion of colonised cannulas used in women (55%), p=0.12. There was also a larger proportion of colonisation when the cannulas were used for 60min or more, p=.002. No significant differences were observed during the time in surgery, suction volume, irrigation volume, prophylaxis use, time of prophylaxis application, prophylaxis booster and type of operation.
Comparison of the socio-demographic and surgical characteristics with and without suction cannula colonisation.
| Variables | Positive cultures (n=40) | Negative culture (n=506) | p value |
|---|---|---|---|
| Sex | |||
| Male | 18 (45%) | 328 (64.8%) | .012 |
| Female | 22 (55%) | 178 (35.2%) | |
| Age group | |||
| <20 | 3 (7.5%) | 45 (8.9%) | .093 |
| 20–39 | 11 (27.5%) | 208 (41.1%) | |
| 40–59 | 8 (20%) | 118 (23.3%) | |
| 60 and over | 18 (45%) | 135 (26.7%) | |
| Time in surgery | |||
| <60 | 2 (5%) | 39 (7.7%) | .25 |
| 60–90 | 16 (40%) | 256 (50.6%) | |
| >90 | 22 (55%) | 211 (41.7%) | |
| Suction volume | |||
| <1000 | 3 (7.5%) | 105 (20.8%) | .10 |
| 1000–1500 | 23 (57.5%) | 270 (53.4%) | |
| >1500 | 14 (35%) | 131 (25.9%) | |
| Irrigation volume | |||
| <1000 | 1 (2.5%) | 70 (13.8%) | .11 |
| 1000–1500 | 26 (65%) | 304 (60.1%) | |
| >1500 | 13 (32.5%) | 132 (26.1%) | |
| Time of suction cannula usage | |||
| <60 | 6 (15%) | 165 (32.6%) | .002 |
| 60–90 | 17 (42.5%) | 238 (47%) | |
| >90 | 17 (42.5%) | 103 (20.4) | |
| Antibiotic prophylaxis | |||
| Yes | 40 (100%) | 503 (99.4%) | 1.00 |
| No | 0 | 3 (.6%) | |
| Prophylaxis application time (preop) | |||
| <20 | 16 (40.0%) | 224 (44.0%) | .77 |
| 20–40 | 21 (52.5%) | 255 (50.0%) | |
| >40 | 3 (.08%) | 27 (.05%) | |
| Prophylaxis booster | |||
| Yes | 11 (27.5%) | 85 (16.8%) | .08 |
| No | 29 (72.5%) | 421 (83.2%) | |
| Complications | |||
| Yes | 0 | 2 (.4%) | .69 |
| No | 40 (100%) | 504 (99.6%) | |
| Type of fracture | Positive cultures n=40 | Negative cultures n=506 | p |
|---|---|---|---|
| Lower radial epiphyseal fracture | 5 (12.5%) | 92 (18.2%) | .3 |
| Upper tibial epiphyseal fracture | 2 (5%) | 44 (8.7%) | |
| Fracture of other finger of the hand | 0 | 36 (7.1%) | |
| Unspecified osteoarthritis of the knee | 2 (5%) | 30 (5.9%) | |
| Inter-tronchanteric fracture | 3 (7.5%) | 28 (5.5%) | |
| Tibial shaft fracture | 2 (5%) | 25 (4.9%) | |
| Fracture of the upper humeral epiphysis | 6 (15%) | 21 (4.2%) | |
| Clavicle fracture | 3 (7.5%) | 22 (4.3%) | |
| Fracture of the leg, part unspecified | 3 (7.5%) | 20 (4.0%) | |
| Fracture of the fibula alone | 2 (5%) | 17 (3.4%) | |
| Unspecified fracture of the foot | 0 | 17 (3.4%) | |
| Femoral shaft fracture | 3 (7.5%) | 13 (2.6%) | |
| Unspecific osteoarthritis of the hip | 0 | 15 (3.0%) | |
| Femoral neck fracture | 0 | 13 (2.6%) | |
| Acetabulum fracture | 2 (5%) | 10 (2.0%) | |
| Dislocation of the acromioclavicular joint | 1 (2.5%) | 11 (2.2%) | |
| Lower tibial epiphyseal fracture | 0 | 11 (2.2%) | |
| Upper radial epiphyseal fracture o | 1 (2.5%) | 10 (2.0%) | |
| Other fractures | 5 (12.5%) | 71 (14%) |
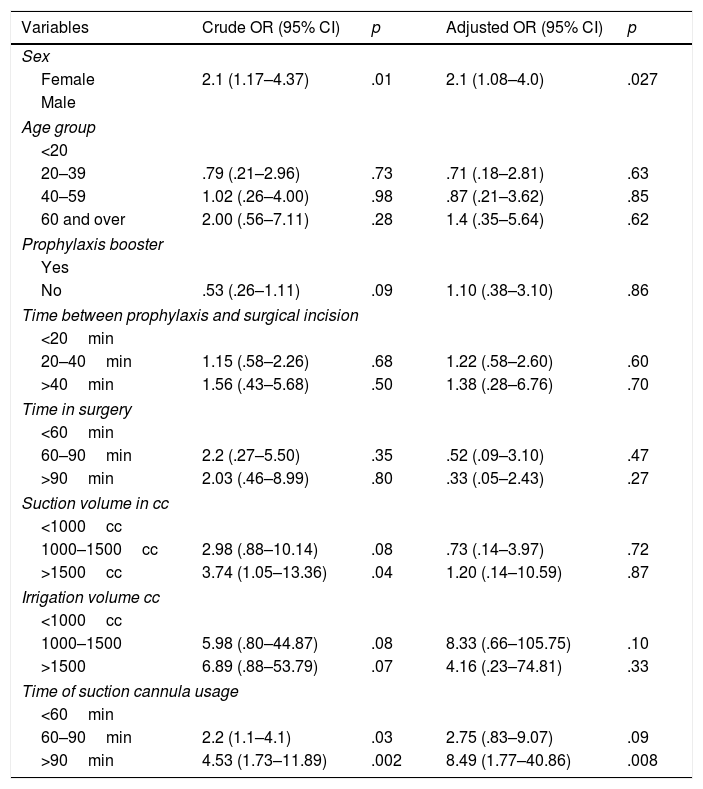
To determine the possible factors associated with suction cannula colonisation the crude and adjusted OR were calculated, which may be observed in Table 3.
Risk factors associated with suction cannula colonisation.
| Variables | Crude OR (95% CI) | p | Adjusted OR (95% CI) | p |
|---|---|---|---|---|
| Sex | ||||
| Female | 2.1 (1.17–4.37) | .01 | 2.1 (1.08–4.0) | .027 |
| Male | ||||
| Age group | ||||
| <20 | ||||
| 20–39 | .79 (.21–2.96) | .73 | .71 (.18–2.81) | .63 |
| 40–59 | 1.02 (.26–4.00) | .98 | .87 (.21–3.62) | .85 |
| 60 and over | 2.00 (.56–7.11) | .28 | 1.4 (.35–5.64) | .62 |
| Prophylaxis booster | ||||
| Yes | ||||
| No | .53 (.26–1.11) | .09 | 1.10 (.38–3.10) | .86 |
| Time between prophylaxis and surgical incision | ||||
| <20min | ||||
| 20–40min | 1.15 (.58–2.26) | .68 | 1.22 (.58–2.60) | .60 |
| >40min | 1.56 (.43–5.68) | .50 | 1.38 (.28–6.76) | .70 |
| Time in surgery | ||||
| <60min | ||||
| 60–90min | 2.2 (.27–5.50) | .35 | .52 (.09–3.10) | .47 |
| >90min | 2.03 (.46–8.99) | .80 | .33 (.05–2.43) | .27 |
| Suction volume in cc | ||||
| <1000cc | ||||
| 1000–1500cc | 2.98 (.88–10.14) | .08 | .73 (.14–3.97) | .72 |
| >1500cc | 3.74 (1.05–13.36) | .04 | 1.20 (.14–10.59) | .87 |
| Irrigation volume cc | ||||
| <1000cc | ||||
| 1000–1500 | 5.98 (.80–44.87) | .08 | 8.33 (.66–105.75) | .10 |
| >1500 | 6.89 (.88–53.79) | .07 | 4.16 (.23–74.81) | .33 |
| Time of suction cannula usage | ||||
| <60min | ||||
| 60–90min | 2.2 (1.1–4.1) | .03 | 2.75 (.83–9.07) | .09 |
| >90min | 4.53 (1.73–11.89) | .002 | 8.49 (1.77–40.86) | .008 |
The crude OR showed that the female sex is associated with colonisation (OR of 2.3 95% CI[1.17–4.34] p=.014) and time of cannula use between 60 and 90min (OR of 2.2 95% CI[1.1–4.1] p=.03); when cannula exposure time was greater than 90min the probability of colonisation increased (OR of 4.5 95% CI[1.73–11.89] p=.002). The other variables studied did not present with any statistically significant association.
Carrying out multivariate analysis using a logistic regression model for calculating the adjusted OR through all the independent variables studied, it was shown that the sex female continued to present a statistically significant association with colonisation (OR of 2.3 95% CI[1.08–4.0] p=.027) similarly to the time of usage of the cannula over 90min (OR 8.5 95% CI[1.77–40.86] p=.008). The other variables studied were not associated.
DiscussionSSI in orthopaedics and trauma is one of the most serious complications that may present after surgery where an implant has been introduced, whether this be a hip, knee or osteosynthesis material implant. It is associated with considerable morbimortality, an increase in hospital costs and the propagation of multi-resistant pathogens.7
Contamination may occur at any time during surgery, from the sterile surgical team or instruments directly introduced into the wound such as catheter suction cannulas which may be a reservoir of microorganisms.8 This study revealed a 7.3%, positivity of culture from suction cannulas which is similar to that reported by Insull and Hudson in 2012. They found that 7.8% of the suction cannulas ends were colonised.8 Other authors, however, have reported a higher percentage that ranges between 24.7% and 80% of positivity.5–10 It was considered that the non-prolonged nature of our surgical procedures, which in 50% of cases was 60min or less had an impact on this result, together with the use of a laminar flow chamber and the strict implementation of sterile techniques as part of the protocol used. Strange-Vognsen et al., in 1988,5 and Givissis et al., in 2008,6 reported a contamination rate of 54%. However, when filtering out the operations which lasted under 1h, this percentage dropped to 9.1% and in addition to this they reported on the non use of laminar flow chambers. Furthermore, their protocol included an initial subculturing in nutrient broth for 48h and subsequent transfer to culture media. This subculturing may have increased the risk of contamination. In the study conducted in Gaza, Palestine, in 2012, Al Laham showed a percentage of culture positivity of 24.7%.9 Review of their protocol found that they did not cultivate the cannulas directly but that the samples were taken with swabs, which is contraindicated by WAIOT principles, and this could have impacted their results. In 2015 Larsson et al. found a percentage of colonisation of 80%10; in this case it is important to note that the average time of surgery in this study was higher than 103min, a situation which has been shown to impact cannula colonisation.10 Furthermore, Vognosse,5 with a colonisation percentage of 54% reported in his study the anaesthesia time and did not specify time in surgery or the use of laminar flow chambers within his protocol.
The most commonly cultivated microorganisms were S. epidermidis (27.5%), followed by S. aureus (12.5%) and E. cloacae (10%); several authors also identified these microorganisms as causal to contamination.4–9 The presence of these pathogenic agents could be explained by the large volume of air which passes through the suction cannula end, through direct contamination of the end with the patient's skin or inappropriate sterile techniques by the surgical team.
One of the most relevant findings of this study is the association between suction cannula colonisation and usage time, which shows that the possibility of cannula colonisation is duplicated from 60min upwards in surgery (OR=2.2 [95% CI: 1.1–4.1]) and the possibility is 8 times higher after 90min of surgery (OR=8.5 [95% CI: 1.77–40.86]). These data are similar to those found in other studies where authors have shown cannula contamination rates rise when they are used for over 60min. One of them is by Givissis et al.,6 who found there was a higher risk of colonisation of the suction cannula end when time in surgery exceeds 60min, observing that the colonisation of the cannula was positive in 66.7% of cases, where surgery exceeded this time, and raising the contamination rate up to seven times, from 9.1% to 66.7%, p-value=.011.6 This author maintains that the end of the suction catheter may be a reservoir for microorganisms due to the continuous passing of large amounts of air through bloodshed and the catheter end may therefore lead to its contamination, with consideration that the longer the cannula is used during surgery the more it may later lead to subclinical or delayed infection, and particularly around artificial joints. In 2007 Byrne et al., reported that catheter colonisation may also be associated with a longer time in surgery. In surgical procedures of under 90min the contamination rate was 17%, and in operations of over 90min the contamination rate was 33%.7
In the most recent consensus on infection led by Parvizi (2019) they recommended changing the cannula after 1h of surgery in order to reduce the rate of contamination,11 considering that in this way the rate of colonisation would decrease, based on the suction cannula creating a constant airflow and it is this airflow which could generate the contamination. However, it is important to stress that no study has been published in the literature which correlates cannula colonisation with surgical site infection. Only one study identified a case where the germ obtained in the cannula coincided with the germ isolated in the cultures of a patient with surgical site infection.6
From this study and the others reviewed, the hypothesis exists that future studies could resolve this question, and determine whether cannula colonisation occurs when the cannula comes into contact with the wound tissues and may be associated with SSI in patients in the immediate or medium term postoperative period.
The authors recognise that one limitation of this study is its inability to generate a clinical correlation between cannula colonisation and surgical site infection for the patient. It would be of great use to follow up patients in their evolution to assess the possible clinical correlation with infection.
ConclusionsDespite the lack of available literature to compare this research, we consider that the proportion of suction cannula colonisation is lower than expected and, in turn, lower than that reported by the studies made, with duration time of cannula use in surgery the main factor to impact on colonisation percentage.
Reducing the time of the suction cannula by compressing this during surgery, except when it is required to visualise the operative field, could reduce airflow to this level and therefore reduce the percentage of colonisation. In any event, the administration of antibiotics of choice for Staphylococcus is also recommended.
Bearing in mind that a not insignificant percentage of suction cannulas are colonised during surgery, it is of interest for future studies to identify the relationship between the percentage of suction cannula colonisation with SSI, and also to identify whether the intermittent use of suction systems reduces colonisation percentage or whether it is necessary to change the suction cannula after 1h in surgery.
Level of evidenceLevel of evidence IV.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: González Edery E, Monclou Garzón F, Reatiga J, Ríos X, de la Rosa A, Arzuza Ortega L. Colonización bacteriana de las cánulas de succión en cirugía ortopédica. Rev Esp Cir Ortop Traumatol. 2020. https://doi.org/10.1016/j.recot.2020.04.007
