





The current pandemic has led to an exponential increase in the need for invasive mechanical ventilation in patients with acute respiratory distress syndrome.
When lung protection and oxygenation targets are not achieved, patients are ventilated in the prone position1 to improve ventilation/perfusion of the alveoli. The lung and alveolar epithelium damage caused by the infection, together with the immune reaction and the cytokine storm, increase alveolar secretions, preventing adequate gas exchange in the undamaged alveoli. There is an increased risk of severe atelectasis secondary to the production of mucus plugs that completely obstruct the bronchial lumen. Various manual respiratory physiotherapy techniques for patients with respiratory distress have been described in the literature. In the case of the COVID-19 pandemic, it is important to ensure that the patient receives the best possible treatment while minimizing the risk of exposure and contact with patients in contaminated areas and reducing the number of people who care for the patient to the absolute minimum. With this objective in mind, we present a series of patients with pneumonia and invasive mechanical ventilation who were placed in the prone position to undergo mobilization of secretions using an autonomous vibratory belt system.
Our objective was to determine whether this would improve ventilator-delivered arterial oxygen partial pressure to fractional inspired oxygen ratio (PAO2/FIO2). PAO2/FIO2 was measured at 3 time points: PAO2/FIO2 supine, PAO2/FIO2 after 2 h prone, and PAO2/FIO2 in the prone position after performing respiratory physiotherapy with an autonomous vibrating belt.
Compassionate use was authorized by the hospitals Research Committee, and the family's authorization and informed consent was obtained verbally and by telephone. A standard vibrating belt (Innovagoods, Sauna effect model, 2019, Valencia, Spain) was used. The belt has various speeds, and for these patients the lowest speed (equivalent to 8 hz) was used, without heat. This minimal vibration is similar to that of full torso belts2,3 that have been used for several years. The physiotherapy belt was placed on the back and lower part of the thorax in order to facilitate mobilization of secretions from the areas of greater decubitus where they are more likely to accumulate.4,5
The belt also has two lateral fabric extensions that allow it to be secured to prevent it from moving during use. The fabric extensions are only used to secure the belt and do not exert any pressure on the patient in order to avoid pressure injuries. The device was placed over the lower posterior thorax two hours after placing the patient in the prone position. Three 15-minute lung physiotherapy sessions were performed, each with the vibrating belt at the lowest vibration speed without local heat.
Each 15-minute physiotherapy session was followed by an hour of rest before the next session. After completing the 3 sessions, and 4 h after the start of respiratory physiotherapy, PAO2/FIO2 was measured.
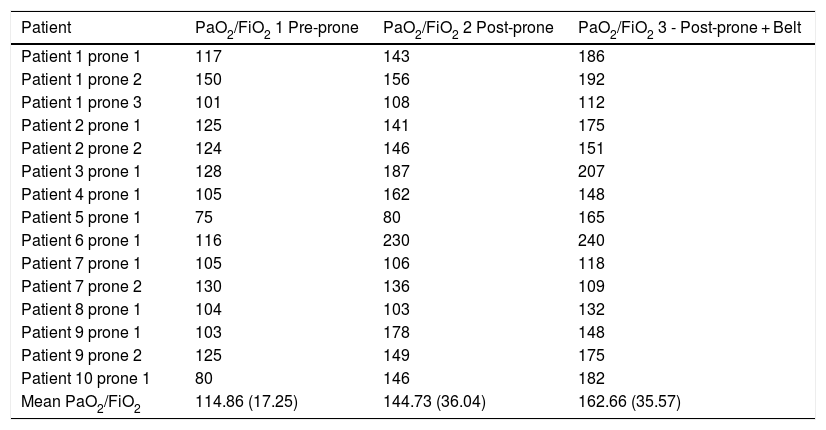
Ten patients were studied immediately after prone positioning, with a total of 15 pronations, observing improvement in 12 (Table 1). Mean PAO2/FIO2o in supine was 114.86 (17.25), in prone it was 144.73 (36.04) and in prone plus physiotherapy it was 162.66 (35.57). An improvement in PAO2/FIO2 was observed in most respiratory physiotherapy interventions, especially in those patients who responded to prone positioning.
PAO2/FIO2 measurements in the supine, prone, and prone position plus respiratory physiotherapy.
| Patient | PaO2/FiO2 1 Pre-prone | PaO2/FiO2 2 Post-prone | PaO2/FiO2 3 - Post-prone + Belt |
|---|---|---|---|
| Patient 1 prone 1 | 117 | 143 | 186 |
| Patient 1 prone 2 | 150 | 156 | 192 |
| Patient 1 prone 3 | 101 | 108 | 112 |
| Patient 2 prone 1 | 125 | 141 | 175 |
| Patient 2 prone 2 | 124 | 146 | 151 |
| Patient 3 prone 1 | 128 | 187 | 207 |
| Patient 4 prone 1 | 105 | 162 | 148 |
| Patient 5 prone 1 | 75 | 80 | 165 |
| Patient 6 prone 1 | 116 | 230 | 240 |
| Patient 7 prone 1 | 105 | 106 | 118 |
| Patient 7 prone 2 | 130 | 136 | 109 |
| Patient 8 prone 1 | 104 | 103 | 132 |
| Patient 9 prone 1 | 103 | 178 | 148 |
| Patient 9 prone 2 | 125 | 149 | 175 |
| Patient 10 prone 1 | 80 | 146 | 182 |
| Mean PaO2/FiO2 | 114.86 (17.25) | 144.73 (36.04) | 162.66 (35.57) |
Changing position from supine to prone may facilitate an improvement in PAO2/FIO2 due to the change in pulmonary perfusion ventilation and mobilization of secretions. Facilitating mobilization and expulsion of secretions with mechanical systems could reduce pulmonary atelectasis and facilitate alveoli ventilation by preventing the formation of mucus plugs that obstruct the bronchioles and improving PAO2/FIO2.
More studies are required to confirm the advantages of respiratory physiotherapy with autonomous vibration belts in critically ill, mechanically ventilated patients with COVID-19 infection placed in the prone position (Fig. 1).

Please cite this article as: Sancho PT, Gandarias PA, González RS, Gurumeta AA. Fisioterapia respiratoria con cinturones de vibración en el paciente crítico COVID-19 en posición de prono. Rev Esp Anestesiol Reanim. 2020;67:481–482.
