





Psoriatic arthritis is an inflammatory arthritis with a wide range of manifestations. The complexity of the disease is a barrier to understanding it, however knowledge about the disease has increased considerably over time, due to advances in genetics, immunology, imaging, and a better understanding of epidemiology. The exact prevalence is unknown, and its calculation is difficult due to the use of different diagnostic or classificatory criteria throughout the last decades. The present work aims to establish the prevalence of psoriatic arthritis in Colombia and to describe the basic demographic characteristics of patients with this disease from the official administrative clinical records of the Colombian Ministry of Health.
ObjectiveTo estimate the prevalence and describe the main demographic characteristics of psoriatic arthritis in Colombia.
Methodology and methodsCross-sectional study, based on official Ministry of Health registry data.
Results6433 cases of psoriatic arthritis (ICD-10 code: M070, M071, M072, M073, L405) were reported between 2012 and 2018, for a prevalence in people over 18 years of 13.5 per 100,000 inhabitants, with a slight predominance of the female population (53%), with a female: male ratio of 1.12: 1, and a higher prevalence in the 55–59 year age group. Additionally, 149,130 cases of psoriasis were identified (ICD-10 code: L400, L401, L402, L403, L404, L408, L409), for a prevalence of psoriatic arthritis of 5.8% in psoriasis patients.
ConclusionsThis is the first study to present demographic information on psoriatic arthritis in Colombia. Data from our study show a lower prevalence compared to other similar studies in the region.
La artritis psoriásica es una enfermedad inflamatoria con una amplia gama de manifestaciones, y su complejidad es una barrera para entenderla. Sin embargo, el conocimiento sobre ella ha aumentado considerablemente con el tiempo, debido, sobre todo, a los avances en la genética, la inmunología y las imágenes, así como a un mejor conocimiento de la epidemiología. La prevalencia exacta de esta enfermedad es desconocida y su cálculo resulta difícil por el uso de diferentes criterios diagnósticos o clasificatorios a lo largo de las últimas décadas. El presente trabajo busca establecer la prevalencia de la artritis psoriásica en Colombia y describir las características demográficas básicas de los pacientes con esta enfermedad, a partir de los registros clínicos administrativos oficiales del Ministerio de Salud de Colombia.
ObjetivoEstimar la prevalencia y describir las principales características demográficas de la artritis psoriásica en Colombia.
MétodosEstudio transversal, basado en datos del registro oficial del Ministerio de Salud.
ResultadosSe notificaron 6.433 casos de artritis psoriásica (código CIE-10: M070, M071, M072, M073, L405) entre el 2012 y el 2018, para una prevalencia en mayores de 20 años de 13,5 por 100.000 habitantes, con un ligero predominio de la población femenina (53%), una relación mujer-hombre de 1,12: 1, y una mayor prevalencia en el grupo de edad de 55 a 59 años. Además, se identificaron 149.130 casos de psoriasis (código CIE-10: L400, L401, L402, L403, L404, L408 y L409), para una prevalencia de artritis psoriásica del 5,8% en pacientes con psoriasis.
ConclusionesEste es el primer estudio que presenta información demográfica sobre la artritis psoriásica en Colombia. Los datos encontrados ponen en evidencia una menor prevalencia en comparación con otros estudios similares en la región.
Psoriatic arthritis belongs to the spondyloarthritis group, defined as an inflammatory arthropathy associated with psoriasis, which can cause permanent joint damage and disability. Its etiology is unknown, but etiopathogenic components have been related, such as genetic factors: HLA-C*60 and other HLA-B alleles, interleukin 12B and a predisposition area in chromosome 6p TRAF3IP2, which encodes a protein involved in IL-17 signaling, as well as environmental factors, such as infections and trauma (Koebner phenomenon). The key pathological phenomena in psoriatic arthritis occur in the skin, synovial membrane, enthesis and bone, where there is a predominance of T lymphocytes, mainly CD8+.1 Joint involvement is highly variable, and 5 major phenotypes have been established: symmetric polyarthritis, asymmetric oligoarthritis, distal interphalangeal joint involvement, axial disease and mutilating arthritis, as described in the first criteria described by Moll in 1973.2 However, other very important manifestations such as dactylitis and enthesitis have been described over the years, which are part of the classification criteria developed in recent years.3 There are no analytical tests that allow its diagnosis. However, it is considered that the absence of the rheumatoid factor and the elevation of acute phase reactants may be useful, as well as plain radiography and musculoskeletal ultrasound findings. Treatment can be complex, due to the diverse nature of the clinical phenotype (peripheral arthritis, skin and nail disease, enthesitis, dactylitis, axial involvement), since not all treatments are equally effective for all the manifestations.4 The exact prevalence of psoriatic arthritis is unknown, studies on the epidemiology of PsA have conflicting results, mainly due to the differences in their methodology, target patient populations, criteria used to define PsA, and also the geographic difference.5 As the results vary according to the setting of the study, the epidemiology data are important for example the prevalence for planning public health programs in this regard and costs of the disease to the Health System. The present work seeks to establish the prevalence of psoriatic arthritis in Colombia and describe the basic demographic characteristics of patients with this disease, from the official administrative clinical records of the Ministry of Health.
Material and methodsThe Colombian health system is one with the highest coverage in Latin America; according to the most recent measurement, carried out in 2019, it reaches 95.1% of the 48 million inhabitants. The Ministry of Health and Social Protection of Colombia developed an information collection and storage tool, called the Comprehensive Social Protection Information System (SISPRO). This tool stores and processes the basic data that the General Social Security System in Health requires for management, regulation and control processes, which are filled out from the Individual Health Services Delivery Registry (RIPS), which the medical staff is required to fill out during each outpatient or inpatient care. All health providers (hospitals and healthcare centers), are required by law to send such information to the SISPRO, using the related code of the international classification of diseases ICD-10 for the primary diagnosis. Therefore, this registry offers consolidated data of the entire population requiring services within the social security system in Colombia. The SISPRO receives data from different sources, which are validated by the Ministry of Health and Social Protection. The data sent is subject to continuous quality control tests.6 The data received is checked against other sources of information (such as the population census, national health surveys, or other administrative records), before being entered into the SISPRO. If inconsistencies are detected, the data is sent back to the reporting institutions for review and correction in order to improve the quality of the data. The information contained in the SISPRO can be freely consulted by the public in the online dynamic tables of the Ministry of Health of Colombia. For the present study, information was obtained from the care provided between January 1, 2012 and December 31, 2018. Following the STROBE guidelines for observational studies, we analyzed the RIPS databases using the International Classification of Diseases code for psoriatic arthritis (ICD-10 code: M070, M071, M072, M073, L405). Diagnostic criteria, or reliability of the diagnosis, however, cannot be validated. Other clinically important information, like patient's ancestry, disease severity or disease duration, are unknown. Information regarding population size, geographical distribution by department, gender and age (distributed into five-year groups), was obtained in accordance with official projections of the National Administrative Department of Statistics (DANE), from the last national census of 2005 which was the one available at the time of conducting the study.7 DANE is the organization that processes official population statistics in Colombia. We estimated the prevalence rates of psoriatic arthritis standardized by age from 2012 to 2018. The numerator was the number of cases of psoriatic arthritis in patients of any age (divided into five-year groups), which were reported to the SISPRO. Prevalence per 100,000 inhabitants was calculated using as numerator any person diagnosed as psoriatic arthritis (counted once). The denominator was the number of inhabitants reported by DANE in each age group or geographical area. Study was approved by the Clinical Research and Ethics Committee of the Pontificia Universidad Javeriana in Bogotá, Colombia.
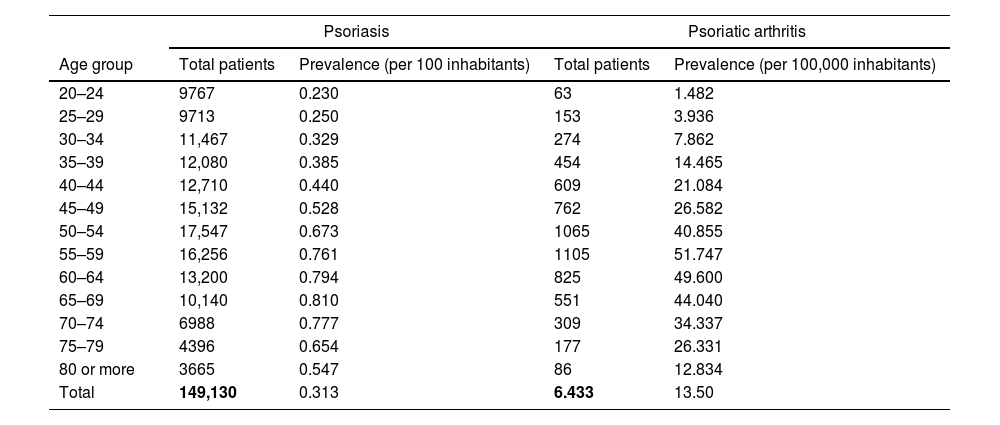
ResultsTotal 6433 cases of psoriatic arthritis were identified, for an estimated prevalence of 13.5/100,000 inhabitants in population 20 or older. 53% of the cases correspond to women, for a female:male ratio of 1.12:1. Colombia is divided into States called departments. In the analysis by departments, the largest number of cases were registered in Antioquia (1122), Bogotá D.C. (963) and Valle del Cauca (415). The departments with the highest prevalence per 100,000 adults were Antioquia (17.6), Caldas (19.3) and Santander (20.1) (Fig. 1). In addition, 149,130 cases of psoriasis were identified (ICD-10 code: L400, L401, L402, L403, L404, L408, L409), for an estimated psoriasis prevalence of 0.31%, and it is estimated in Colombia 5.8% of psoriasis patients have psoriatic arthritis (see Table 1).

Prevalence of psoriasis and psoriatic arthritis by age group in Colombia between 2012 and 2018.
| Psoriasis | Psoriatic arthritis | |||
|---|---|---|---|---|
| Age group | Total patients | Prevalence (per 100 inhabitants) | Total patients | Prevalence (per 100,000 inhabitants) |
| 20–24 | 9767 | 0.230 | 63 | 1.482 |
| 25–29 | 9713 | 0.250 | 153 | 3.936 |
| 30–34 | 11,467 | 0.329 | 274 | 7.862 |
| 35–39 | 12,080 | 0.385 | 454 | 14.465 |
| 40–44 | 12,710 | 0.440 | 609 | 21.084 |
| 45–49 | 15,132 | 0.528 | 762 | 26.582 |
| 50–54 | 17,547 | 0.673 | 1065 | 40.855 |
| 55–59 | 16,256 | 0.761 | 1105 | 51.747 |
| 60–64 | 13,200 | 0.794 | 825 | 49.600 |
| 65–69 | 10,140 | 0.810 | 551 | 44.040 |
| 70–74 | 6988 | 0.777 | 309 | 34.337 |
| 75–79 | 4396 | 0.654 | 177 | 26.331 |
| 80 or more | 3665 | 0.547 | 86 | 12.834 |
| Total | 149,130 | 0.313 | 6.433 | 13.50 |
The prevalence is calculated by dividing the total number of patients by the average population of the period by age group, as denominator, per 100 inhabitants and 100,000 inhabitants, respectively.
Studies on the epidemiology of psoriasis and psoriatic arthritis have produced diverse results, mainly due to differences in methodology, populations, diagnostic criteria, in addition to geographical variables.8 With respect to psoriasis, prevalence in the general population range from 0.1% in Tanzania9 to 5.1% in the United States.10 When evaluating adults only, the prevalence of psoriasis ranges from 0.51% in the United States geriatric population,11 to 11.43% in a study in Northern Norway, which reported the psoriasis prevalence during the 1979–2008 period, and a progressive increase was observed after each decade since the beginning of the analysis.12 We found a study in Brazil that reported a psoriasis prevalence of 1.2%,13 a higher value than in our study (prevalence of psoriasis in Colombia: 0.31%). However, our prevalence data is similar to reported in China (0.49%) and in Taiwan (0.23%).14,15
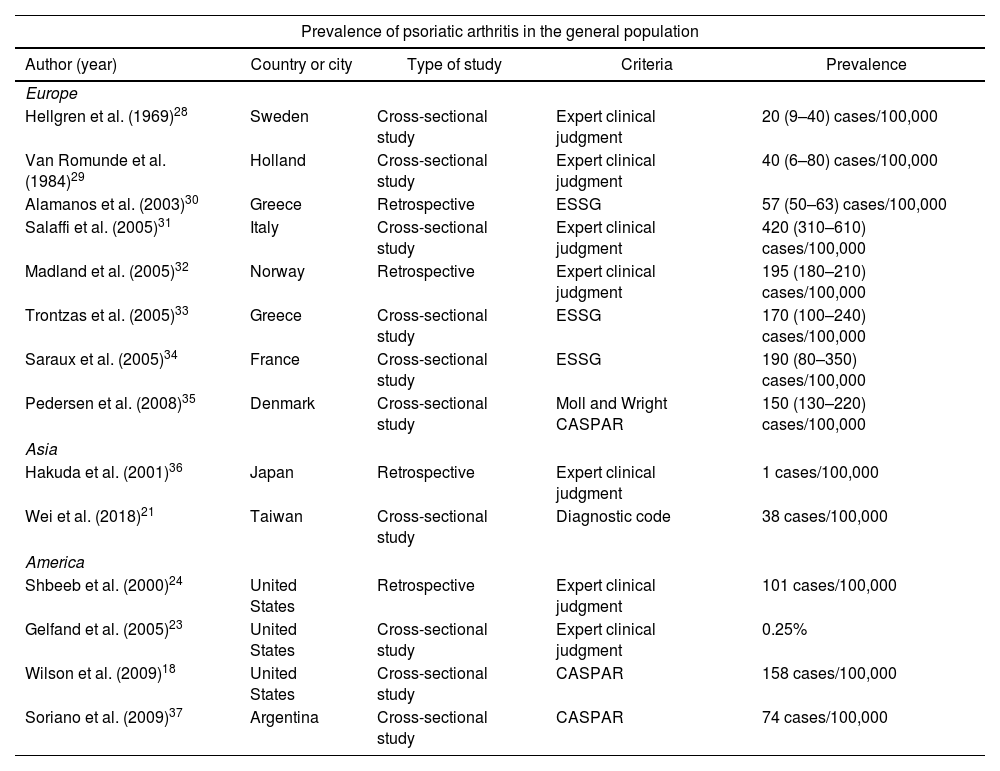
Literature data on the prevalence of psoriatic arthritis is also variable.5,16 Prevalence studies based on the general population report high prevalence, like 670 per 100,000 inhabitants in Norway17 and 158 per 100,000 inhabitants in the United States,18 and lower in Denmark,19 Israel20 and Taiwan, ranging from 11.12 to 38 per 100,000 inhabitants in a 2001–2013 follow-up period.21 A systematic review that included 13 studies of the prevalence of psoriatic arthritis in the general population reported values between 3 and 23.1 per 100,000 inhabitants, similar values in our data in the general population: 13.50 per 100,000.22 Data from different studies, mostly conducted in the United States, prevalence of psoriatic arthritis in patients diagnosed with psoriasis ranges from 6% to 40%.23,24 Data from European studies on the prevalence of psoriatic arthritis among psoriasis patients are also very variable, ranging from 5% in Turkey25 to 21% in Sweden.26 A study conducted in the United States to validate the codes used in the ICD-9 diagnosis, used a methodology very similar to our work. That study reports 87,827 cases of psoriasis, and of these, 5187 also had the psoriatic arthritis code, for a prevalence of psoriatic arthritis of 5.9% among psoriasis patients, data very close to that found in our study (5.8%)27 (see Table 2).
Prevalence of psoriatic arthritis in different regions.
| Prevalence of psoriatic arthritis in the general population | ||||
|---|---|---|---|---|
| Author (year) | Country or city | Type of study | Criteria | Prevalence |
| Europe | ||||
| Hellgren et al. (1969)28 | Sweden | Cross-sectional study | Expert clinical judgment | 20 (9–40) cases/100,000 |
| Van Romunde et al. (1984)29 | Holland | Cross-sectional study | Expert clinical judgment | 40 (6–80) cases/100,000 |
| Alamanos et al. (2003)30 | Greece | Retrospective | ESSG | 57 (50–63) cases/100,000 |
| Salaffi et al. (2005)31 | Italy | Cross-sectional study | Expert clinical judgment | 420 (310–610) cases/100,000 |
| Madland et al. (2005)32 | Norway | Retrospective | Expert clinical judgment | 195 (180–210) cases/100,000 |
| Trontzas et al. (2005)33 | Greece | Cross-sectional study | ESSG | 170 (100–240) cases/100,000 |
| Saraux et al. (2005)34 | France | Cross-sectional study | ESSG | 190 (80–350) cases/100,000 |
| Pedersen et al. (2008)35 | Denmark | Cross-sectional study | Moll and Wright CASPAR | 150 (130–220) cases/100,000 |
| Asia | ||||
| Hakuda et al. (2001)36 | Japan | Retrospective | Expert clinical judgment | 1 cases/100,000 |
| Wei et al. (2018)21 | Taiwan | Cross-sectional study | Diagnostic code | 38 cases/100,000 |
| America | ||||
| Shbeeb et al. (2000)24 | United States | Retrospective | Expert clinical judgment | 101 cases/100,000 |
| Gelfand et al. (2005)23 | United States | Cross-sectional study | Expert clinical judgment | 0.25% |
| Wilson et al. (2009)18 | United States | Cross-sectional study | CASPAR | 158 cases/100,000 |
| Soriano et al. (2009)37 | Argentina | Cross-sectional study | CASPAR | 74 cases/100,000 |
| Prevalence of psoriatic arthritis among psoriasis patients | ||||
|---|---|---|---|---|
| Reich et al. (2009)38 | Germany | Cross-sectional study | Moll and Wright | 20.6% |
| Ibrahim et al. (2009)39 | United Kingdom | Cross-sectional study | CASPAR | 13.8% |
| Yang et al. (2011)40 | China | Cross-sectional study | CASPAR | 5.8% |
| Khraishi et al. (2012)41 | Canada | Cross-sectional study | CASPAR | 40.9% |
| Carneiro et al. (2012)42 | Brazil | Cross-sectional study | CASPAR | 35% |
| Papadavidal et al. (2016)43 | Greece | Cross-sectional study | Moll and Wright | 30.5% |
There are few studies in Latin America that report prevalence data. A six-year follow-up study of patients from the Hospital Italiano in Buenos Aires showed a prevalence of psoriatic arthritis of 74 per 100,000 patients in the general population.37 Another study in Brazil showed a prevalence of psoriatic arthritis in psoriasis patients of 40%.43 In Colombia there are no published studies on the prevalence of psoriatic arthritis in our population or in psoriasis patients. However, a recent work in which ICD-10 codes were used and records of the ministry of health of 3 Latin American countries were reviewed: DEIS of Chile, DATASUS of Brazil, and SISPRO of Colombia between 2010 and 2014, estimated a prevalence of psoriatic arthritis in psoriasis patients of 65%, 49% and 3–4%, respectively.44
The differences between these prevalence studies may be due to the way patients were selected; for example, the definition of cases through patient self-report vs. confirmation through medical record, as well as the type of population studied (general population vs. psoriasis reference centers). However, despite the differences, there seems to be a clear tendency to an increase in prevalence in recent years, similar to what our study reports; this is probably due to a greater interest on the part of the dermatologists to make the diagnosis of psoriatic arthritis and a greater use of questionnaires developed in the last two decades, which help screen and identify possible psoriatic arthritis patients in the psorasis consultation of dematologists. These tools include TOPAS,45 with translation and validation in Spanish,46 PEST39 and PASE,47 the latter also with translation and validation at Spanish.48 The increase in prevalence in recent years could also be due to genetic and environmental factors associated with pathogenesis, such as alcohol consumption, stress, smoking, infections and obesity.49 The previously mentioned studies also reported that psoriatic arthritis affects men and women equally, with a greater frequency between the fourth and fifth decade of life. Our study shows a slightly higher prevalence in women and dominance in the fifth decade, as recorded in the literature.
The present study shows information on the prevalence of psoriatic arthritis in Colombia, through the analysis of data collected in SISPRO from patients registered with this diagnosis, using five ICD-10 codes. This may lead to under-reporting or wrong reporting by doctors when entering the ICD 10 code in the medical records, in addition to the arbitrary use only of psoriasis codes for the diagnosis of psoriatic arthritis, as reported in other studies that use the ICD-9 or ICD-10 code methodology.27 However, this data is the one that is legally recorded when patients are treated in Colombia and with which the Colombian Ministry of Health and Social Protection works, so it merits an approach and analysis like the one performed in the present work. Another weakness of our study is that it is not possible to establish the time of evolution of the disease, its incidence and severity, the demand for specialized services related to the disease, or mortality.
ConclusionThe present study shows demographic and epidemiological information on psoriatic arthritis in Colombia, taken from the database of the Ministry of Health. The study data show a low prevalence of psoriatic arthritis, both in the general population and in psoriasis patients, when compared to that reported in the United States, Europe and Latin America, but similar to that of the Asian population. There was a similar prevalence in men and women, with a higher prevalence of female in the 55–59 age group. The results of our study provide epidemiological information that contributes to a better understanding of psoriatic arthritis in Colombia and Latin America.
Authors’ contributionsAll authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Daniel Fernández-Ávila, Diana Rincón-Riaño, Santiago Bernal-Macías, Juan M Gutierrez and Diego Rosselli. The first draft of the manuscript was written by Diana Rincón-Riaño and all authors commented on previous versions of the manuscript. All co-authors take full responsibility for all aspects of the study and the final manuscript.
Ethics statementPatients’ informed consent was not required, as the research group had no direct contact with patients given that it was a retrospective study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of Medical School of Pontificia Universidad Javerina with the approval number 2018/20 and followed the 1964 Helsinki Declaration and its later amendments as well as national ethical standards (Resolution 8430 of 1993).
Conflicts of interestDaniel Fernández-Ávila, Diana Rincón-Riaño, Santiago Bernal-Macías, Juan M. Gutierrez and Diego Rosselli declare that they have no conflict of interest.
Supplementary material:
