



A case is presented of septic knee arthritis caused by Pseudomonas stutzeri, which is an aerobic gram-negative bacillus widely distributed in nature and rarely causes serious infections in humans. The patient is an 84-year-old woman on haemodialysis, who developed a septic arthritis of the right knee after a hyaluronic acid injection. There was a favourable outcome after antibiotic therapy. This aetiology should be taken into account when there is a history of local invasion of the joint and in states of immunosuppression, as occurred in this patient.
Se presenta un caso de artritis séptica de rodilla por Pseudomonas stutzeri, bacilo gramnegativo aerobio ampliamente distribuido en la naturaleza y que rara vez ocasiona infecciones graves en el ser humano. Se trata de una mujer de 84 años, hemodializada, que desarrolla una artritis séptica de rodilla derecha tras una inflitración con ácido hialurónico y que evoluciona favorablemente tras terapia antibiótica. Se debe tener en cuenta esta etiología cuando hay antecedentes de invasión local de la articulación y en estados de inmunosupresión tal y como sucede en nuestra paciente.
Pseudomonas stutzeri is an aerobic gram-negative non-fluorescent bacillus, widely distributed in the environment, which has been isolated as an opportunistic human pathogen.1 This article discusses a case of septic arthritis, secondary to P. stutzeri, which is an unusual causal agent of this type infection, similar to other gram-negative bacteria.2
Clinical caseThis is an 84-year old female, allergic to sulfonamides and penicillin. The patient has a history of multifactorial origin chronic kidney disease, undergoing hemodialysis and calciphylaxis, with a chronic right lower limb ulcer. Additionally, the patient presents with high blood pressure, diabetes mellitus type 2, asymptomatic hyperuricemia receiving treatment with alopurinol, and gonarthrosis, who has been experiencing increasing mechanical pain over the past 2 months. The patient was treated one month before with an intra-articular infiltration of hyaluronic acid (with negligible improvement). She was admitted with right lower limb erythema and knee pain, with minor inflammatory signs and suspicious cellulitis. At home, the patient did not control her temperature. The examination revealed discrete localized fever of the right knee, and the laboratory tests showed a C-reactive protein of 28.34 mg/dL, with normal CBC. The knee X-ray showed severe joint space narrowing (grade III–IV arthrosis). The patient underwent arthrocentesis, from which 1 ml of macroscopically inflammatory synovial fluid was obtained; under the microscope, the fluid presented abundant leukocytes and intracellular pyrophosphate crystals. Due to the small fluid sample obtained, no urgent biochemistry analysis was performed. Empiric antibiotic therapy was initiated while waiting for the results of the microbiological cultures, due to the potential of septic arthritis (immunosuppressed patient). The synovial fluid culture isolated P. stutzeri sensitive to meropenem and quinolones, and resistant to piperacillin, with negative synovial fluid and blood cultures. The patient remained thermodynamically stable during her hospital admission, and evolved favorably with antibiotic therapy: 2 weeks of IV meropenem 1 g/day, followed by 4 weeks of oral ciprofloxacin 500 mg every 12 h. No intra-articular drainage was required. Another option for the differential diagnosis is a pyrophosphate monoarthritis (presence of crystals under the microscope and chronic kidney disease with probable associated hyperparathyroidism). Nevertheless, the good response to antibiotic therapy, without the use of corticoids or NSAIDs, is supportive of the septic origin of the condition in this particular patient.
DiscussionP. stutzeri is usually found as a saprophyte on the floor and in hospital environments, but seldom leads to severe community or hospital acquired infection. The cases of P. stutzeri infection normally present in immunocompromised patients, with underlying diseases, or previous surgery. They have been more frequently isolated in surgical wounds, blood, respiratory tract and urine.3 The treatment of choice is ciprofloxacin or carbapenem,2 but piperacillin-tazobactam and ceftazidime may be other options.3
Gram-positive bacteria (specifically Staphylococcus aureus and Streptococcus) are the most frequent aetiology in septic arthritis, and the empirical therapy of choice is ceftriaxone 2 g every 24 h and cloxacillin 2 g every 4 h. Other etiological possibilities should be considered in immunosuppressed patients (such as gram-negatives) and the usual empiric antibiotic regimen may not be enough.2
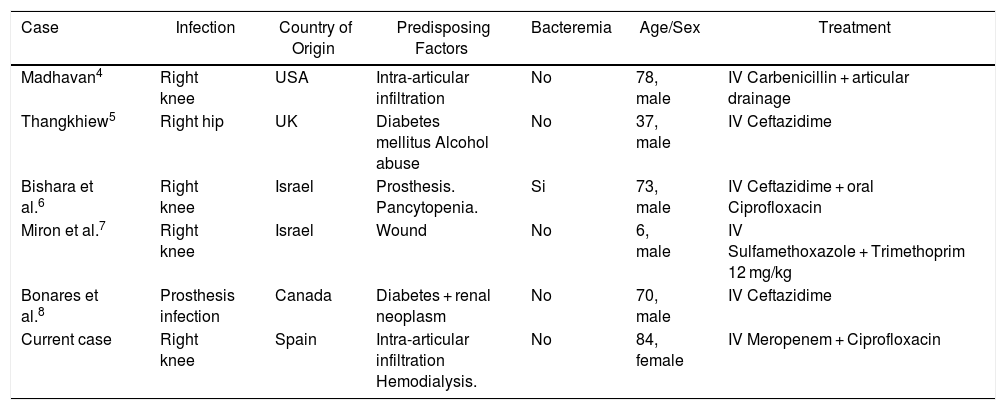
As far as we know, this is the sixth case of septic arthritis due to P. stutzeri, reported in the literature, as illustrated in Table 1. The first case reported,4 is a 78-year old male with a history of psoriasis and pulmonary emphysema, who developed septic arthritis following an intra-articular corticoid infiltration. The second case reported5 is a 37-year old patient with hip septic arthritis and a history of diabetes mellitus and alcohol abuse. The third case is a prosthetic knee infection in a 73-year old patient with pancytopenia. The fourth case7 is a 6-year old child with septic arthritis of the knee, secondary to a knife wound. The last case reported8 is a 70-year old male, with prosthetic infection and a history of diabetes mellitus and renal neoplasm. Three cases of osteomyelitis have also been reported.8–11 Therefore, in all of the cases mentioned, there is a history of local joint invasion or a condition of immunosuppression. In this particular case, the patient was undergoing renal replacement therapy with hemodialysis and she had a history of intra-articular infiltration one month prior to the development of arthritis. All patients evolved satisfactorily with antibiotic therapy. This search was conducted in Medline, Embase, Google Scholar, BVSalud and Scielo, using the kew word “arthritis” and “Pseudomonas stutzeri”; we could not find any cases reported in Latin America.
Reported cases of septic arthritis from Pseudomonas stutzeri.
| Case | Infection | Country of Origin | Predisposing Factors | Bacteremia | Age/Sex | Treatment |
|---|---|---|---|---|---|---|
| Madhavan4 | Right knee | USA | Intra-articular infiltration | No | 78, male | IV Carbenicillin + articular drainage |
| Thangkhiew5 | Right hip | UK | Diabetes mellitus Alcohol abuse | No | 37, male | IV Ceftazidime |
| Bishara et al.6 | Right knee | Israel | Prosthesis. Pancytopenia. | Si | 73, male | IV Ceftazidime + oral Ciprofloxacin |
| Miron et al.7 | Right knee | Israel | Wound | No | 6, male | IV Sulfamethoxazole + Trimethoprim 12 mg/kg |
| Bonares et al.8 | Prosthesis infection | Canada | Diabetes + renal neoplasm | No | 70, male | IV Ceftazidime |
| Current case | Right knee | Spain | Intra-articular infiltration Hemodialysis. | No | 84, female | IV Meropenem + Ciprofloxacin |
P. stutzeri is a rare cause of septic arthritis, but it must be kept in mind in patients with septic arthritis and a history of local joint invasions or immunosuppression. Because of its sensitivity profile, the usual empiric antibiotic therapy for septic arthritis may not be helpful in this cases.
Conflict of interestsThe authors have no conflict of interests to disclose.
Please cite this article as: Ranieri L, López-Salguero S, González Galván Y, Andrés M. A propósito de un caso: pseudomonas stutzeri, una causa inusual de artritis séptica. Rev Colomb Reumatol. 2020;27:215–217.
