





Information and communication technologies (ICT) have made it possible to provide the population with accessible, profitable, and high-quality healthcare services in different pathologies. It is important to conduct an evaluation of the satisfaction of users of telemedicine who require frequent monitoring as in the case of chronic diseases such as rheumatoid arthritis; this is also important for insurers.
ObjetiveThe objective of the study was to evaluate the degree of satisfaction with telemedicine care among patients with rheumatoid arthritis from a health provider entity in Colombia.
Materials and methodsAn observational, descriptive cross-sectional study was carried out, patients older than 18 years with a diagnosis of rheumatoid arthritis who received telemedicine care on more than one occasion were included, telephone surveys were carried out in which the SERVQHOS questionnaire was applied to evaluate the quality of the health service; A dissatisfied patient was defined as one with an average response of 3 or less in the questions of the questionnaire, and a very satisfied patient when the average was 4 or more. The primary objective was to determine the degree of satisfaction of a cohort and the number of highly satisfied patients. We also evaluated whether there was an association between sex, age, origin, number of consultations, socio-economic status, and educational level with a high rating by very satisfied patients.
ResultsA total of 243 patients were evaluated. Evaluation of satisfaction with the telemedicine service in rheumatology showed that 92.2% of the patients were satisfied and 49% very satisfied. In the subsequent analysis, an association was found between very high satisfaction and a greater number of consultations (p = 0.001), people living in rural areas (p = 0.03), and a higher level of schooling with a greater difference in secondary education (p = 0.017).
ConclusionsWe found that the vast majority of patients surveyed were satisfied with the quality of telemedicine care and half were very satisfied which increases with the number of consultations, in people from rural areas and in some educational levels.
Las tecnologías de la información y la comunicación (TIC) han permitido brindar a la población servicios de atención en salud accesible, rentable y de alta calidad en diferentes patologías. Es importante hacer una evaluación de la satisfacción de los usuarios que utilizan la telemedicina y requieren seguimiento frecuente, como en el caso de las enfermedades crónicas como la artritis reumatoide, dato que es importante también para los aseguradores.
ObjetivoEl objetivo del estudio fue evaluar el grado de satisfacción de la atención por telemedicina de los pacientes con artritis reumatoide de una entidad prestadora de salud en Colombia.
Materiales y métodosSe realizó un estudio observacional, descriptivo transversal, en el que se incluyeron pacientes mayores de 18 años con diagnóstico de artritis reumatoide a quienes se atendió por telemedicina en más de una ocasión; se realizaron encuestas telefónicas en las cuales se aplicó el cuestionario SERVQHOS para evaluar la calidad del servicio en salud; se definió como paciente insatisfecho aquel con un promedio de respuestas de 3 o menos en las preguntas del cuestionario, satisfecho mayor a 3 y muy satisfecho cuando el promedio era de 4 o más. El objetivo primario es determinar el grado de satisfacción de la cohorte de pacientes y el número de pacientes muy satisfechos. Así mismo, se evaluó si existe una asociación entre sexo, edad, procedencia, número de consultas, estrato socioeconómico y nivel educativo con una alta calificación de muy satisfecho en los pacientes.
ResultadosSe evaluó un total de 243 pacientes, la evaluación de satisfacción en el servicio de telemedicina en reumatología evidenció que el 92,2% de ellos se encuentra satisfecho y el 49% muy satisfecho. En el análisis posterior se encontró asociación entre la muy alta satisfacción y un mayor número de consultas (p = 0,001), personas que viven en el área rural (p = 0,03) y un mayor nivel de escolaridad con mayor diferencia en formación secundaria (p = 0,017).
ConclusionesSe encontró que la gran mayoría de los pacientes encuestados está satisfecha con la calidad de la atención por telemedicina y la mitad tiene una muy alta satisfacción, la cual aumenta con el número de consultas, en personas de área rural y en algunos grupos de nivel educativo como básica secundaria y profesional.
Information and communication technologies have been beneficial in addressing the challenges that developing countries face in providing the population with accessible, cost-effective, and high-quality health care services. In some occasions, due to geographic barriers, this population lacks medical care. Telemedicine has been an instrument that has guaranteed the follow-up of patients with chronic and high-cost diseases, allowing the reduction of inequality gaps and the improvement in the quality of life.1
Rheumatoid arthritis (RA) is a chronic, inflammatory, multisystem autoimmune disease that affects the musculoskeletal system and is associated with a significant decrease in life expectancy. This disease of unknown etiology affects between 0.2% and 5% of the world population, with a 3:1 preponderance of females.2 According to the report of the High Cost Account, in Colombia, in 2019, 81,386 people were registered with RA, with a prevalence of 0.24%.3
In patients with this disease, it is essential to control the inflammation in order to prevent joint damage through strict follow-up by rheumatology specialists. For this reason, the use of information and communication technologies has gained great importance in monitoring this condition because it can generate continuity of care, control the disease, expand health coverage, reduce transfers, optimize waiting times for a consultation with the specialist and increase patient education for the adequate management of their disease.4
We were interested in the results obtained in a study that focused on a rural municipality in northern Australia, where the satisfaction with telemedicine in rheumatology was evaluated and a level of satisfaction between 85% and 90% was estimated, since it also allowed patients to save time and money, being the method for their care.5
For these reasons, it is important to carry out an evaluation of the satisfaction of the users of telemedicine and, on the other hand, the usefulness for the insurers, since is it a fundamental indicator concerning the quality care in health service. This opinion becomes one of the major sources of information to verify the quality of care offered, the errors and failures that may be being committed, and likewise allows the implementation of strategies to improve the service.6
There are models to evaluate service quality, such as SERVQUAL, proposed by Parasuraman, Zethaml and Berry, validated for the first time in Latin America in 1992 by Michelsen Consulting and the Latin American Institute of Service Quality, to be applied by the companies. However, it has also been useful in health services.7
Another different questionnaire to be developed by patients is the SERVQHOS, which contains basic elements for the evaluation and quality of hospital care, has been validated in Spanish and has been used in Colombia in several studies. This questionnaire combines expectations and perceptions with a smaller number of items, compared with the SERVQUAL model, to be applied to patients who access medical care.7 These expectations and perceptions are designed for the general evaluation of the entire health care (medical staff, non-medical staff, facilities, equipment…) and not in a specific process, in this case for telemedicine.
This research seeks to evaluate the satisfaction of a group of patients with RA treated in a tele-rheumatology service, which can allow to correct possible shortcomings and promote strengths that lead to improving the provision of health services.
MethodologyDefinition of the population and the interventionAn observational, analytical, cross-sectional study, which included patients older than 18 years diagnosed with RA according to the American College of Rheumatology (ACR)/European League against Rheumatism (EULAR) classification criteria was carried out.
The patients were treated by telemedicine through the syncronous modality, which consists in 2 offices in a health center, both in the issuing site and in the reception site, equipped with a videoconference system and high-definition cameras that allow real-time communication with the patient. In the issuing office there is a doctor with basic experience and training in musculoskeletal disorders, mainly for performing the physical examination.
These patients must have some means of telecommunication (landline or cell phone) to answer the survey, but not for the consultation.
The period evaluated was from March 2017 until March 2020, and the verbal consent for the evaluation was obtained. Those patients with only one assessment by telemedicine were excluded; it was considered that with a single attention it was not adequate to fully assess the quality of the service received and that the degree of acceptance could improve after a first visit. In addition, patients with hearing or visual difficulties or other limitations that impaired adequate communication to obtain the information were excluded.
Collection of the informationDuring the telemedicine consultation, the patient was informed that a telephone survey on satisfaction with the service received would be carried out. After the consultation, the call was made by the research team, in which the patient's verbal authorization was obtained and the satisfaction survey was applied to respond to the proposed objectives.
The appreciation of the quality of the healthcare service and the degree of satisfaction with telemedicine were evaluated through the use of the SERVQHOS questionnaire, which was applied by telephone.
The SERVQHOS survey consists of 19 ordinal categorical variables that evaluate the quality of the health service. Each of these variables is scored in a previously established Likert scale, in which 1 is “it has been much worse than expected”, 2 is “worse than expected”, 3 is “as expected”, 4 is “better than expected” and 5 is “much better than expected.” The maximum score is 95 points and the minimum is 19 points, of which a mean of the responses will be used for the definitions.
In addition, the patients were asked about age, occupation, gender, marital status, educational level, the city in which they lived, the area where the house was located, the socioeconomic stratum and smoking.
Information bias was controlled by training the interviewers. A pilot test was carried out in which the procedures were standardized, which allowed making changes if required. Source biases were controlled by sensitizing all respondents on the need to answer the survey in its entirety, as well as providing help if required.
For the analysis, it was arbitrarily defined to categorize each dissatisfied participant as the one with an average of responses of 3 or less, satisfied with responses of 3, and very satisfied when the average was 4 or more.
A sample size was not calculated, since an attempt was made to obtain data from the entire population seen in the telemedicine program.
The degree of satisfaction of the cohort and the number of patients highly satisfied was determined. It was evaluated if there was an association between gender, age, origin, number of consultations, socioeconomic status and educational level with a rating of very satisfied.
Statistical analysisInitially, a univariate analysis was performed, describing the numerical variables as means and their standard deviations (SD) or medians with their interquartile range (IQR), as specified by their normal or non-normal nature, respectively, according to the graphic assessment of the distribution of the responses; likewise, the categorical variables were described with their relative and absolute frequencies. As for the bivariate analysis, the relationship between patient satisfaction and gender, age, origin, number of consultations, socioeconomic status and educational level was studied, using the Student’s t or the Mann–Whitney U test, according to the nature of the distributions, and the Kruskal–Wallis test for ordinal categorical variables. The Chi-square test was used for the analysis of variables of dichotomous nature; In addition, the analysis of the association of the variables gender, age, origin, number of consultations, socioeconomic status and educational level with the group of highly satisfied patients was performed. A p < 0.05 was considered as statistically significant.
Ethical considerationsThe authors have the informed consent of the patients.
ResultsThe database of the tele-rheumatology service initially yielded 650 patients with RA. The size of the population with more than one telemedicine assessment was 447 patients, to whom telephone calls were made, with the following results: 243 effective calls in which the survey was filled out in its entirety and adequately, 195 calls in which telephone communication with the patient was not achieved, the patient had died in 4 (2%) cases, the patient was not enabled in the system in 4 (2%) cases, and others corresponded to one (0.5%) case (patient with cognitive deficit, who could not answer the survey, and attended his last telemedicine consultation without a companion).
Of the 243 effective calls, the majority of the population was made up of women (88%), from the Andean region (58%), residents of urban areas (88.8%) and with a secondary educational level (48%).
The complete description of the demographic variables, including the antibody profile and the functionality scale, considering their importance in this disease is presented in Table 1.
Sociodemographic characteristics.
| Characteristics | Total number of RA patients (n = 243) |
|---|---|
| Gender | |
| Men | 28 (11.5%) |
| Women | 215 (88.5%) |
| Age in years (SD) | 53.9 (14.4%) |
| Educational level | |
| Elementary | 45 (18.5%) |
| Secondary | 118 (48.5%) |
| Professional | 50 (20.6%) |
| Postgraduate | 27 (11.1%) |
| None | 3 (1.23%) |
| Region of residence | |
| Andean | 141 (58.0%) |
| Caribbean | 27 (11.1%) |
| Pacific | 59 (24.2%) |
| Orinoquia | 16 (6.7%) |
| Area in which is located | |
| Urban | 215 (88.8%) |
| Rural | 28 (11.5%) |
| Socioeconomic status | |
| 1 | 16 (6.6%) |
| 2 | 63 (25.9%) |
| 3 | 116 (47.7%) |
| 4 | 35 (14.4%) |
| 5 | 7 (2.9%) |
| 6 | 6 (2.5%) |
| Cigarette smoking | |
| Yes | 49 (20.16%) |
| No | 194 (79.8%) |
| Immunological profile | |
| RA Test – | 34 (13.9%) |
| RA Test + | 207 (85.2%) |
| Unknown | 2 (0.82%) |
| Anti-citrullines | |
| Citrulline – | 40 (16.46%) |
| Citrulline + | 148 (60.9%) |
| Unknown | 55 (22.6%) |
| Number of consultations | |
| 2–4 | 151 (62.1%) |
| 5–7 | 55 (22.6%) |
| 8–10 | 30 (12.3%) |
| >10 | 7 (2.9%) |
| Time with the disease | |
| 0–5 years | 74 (30.4%) |
| 5–10 years | 59 (24.2%) |
| 10–15 years | 46 (18.9%) |
| 15–20 years | 13 (5.3%) |
| More than 20years | 43 (17.7%) |
| Unknown | 8 (3.3%) |
| Functionality measured with the HAQ | |
| 0–0.49 | 117 (48.1%) |
| 0.5–0.99 | 38 (15.6%) |
| 1–1.49 | 29 (11.9%) |
| 1.5–1.99 | 18 (7.4%) |
| Two or more | 13 (5.3%) |
| Not registered | 28 (11.5%) |
SD: standard deviation.
The evaluation of the degree of satisfaction revealed that only 19 of 243 patients obtained an average less than or equal to 3, or were not satisfied with the quality of the service; this is equivalent to 7.8%, therefore, the remaining 92.2% correspond to satisfied patients or with an average in the survey higher than 3. Regarding the number of very satisfied patients, 120 were found, almost half (49.3%), since they considered in most of the responses that the service provided was better or much better than expected.
The distribution of the satisfaction of the group of patients can be seen in Fig. 1, according to the average satisfaction of the responses of the SERVQHOS instrument.

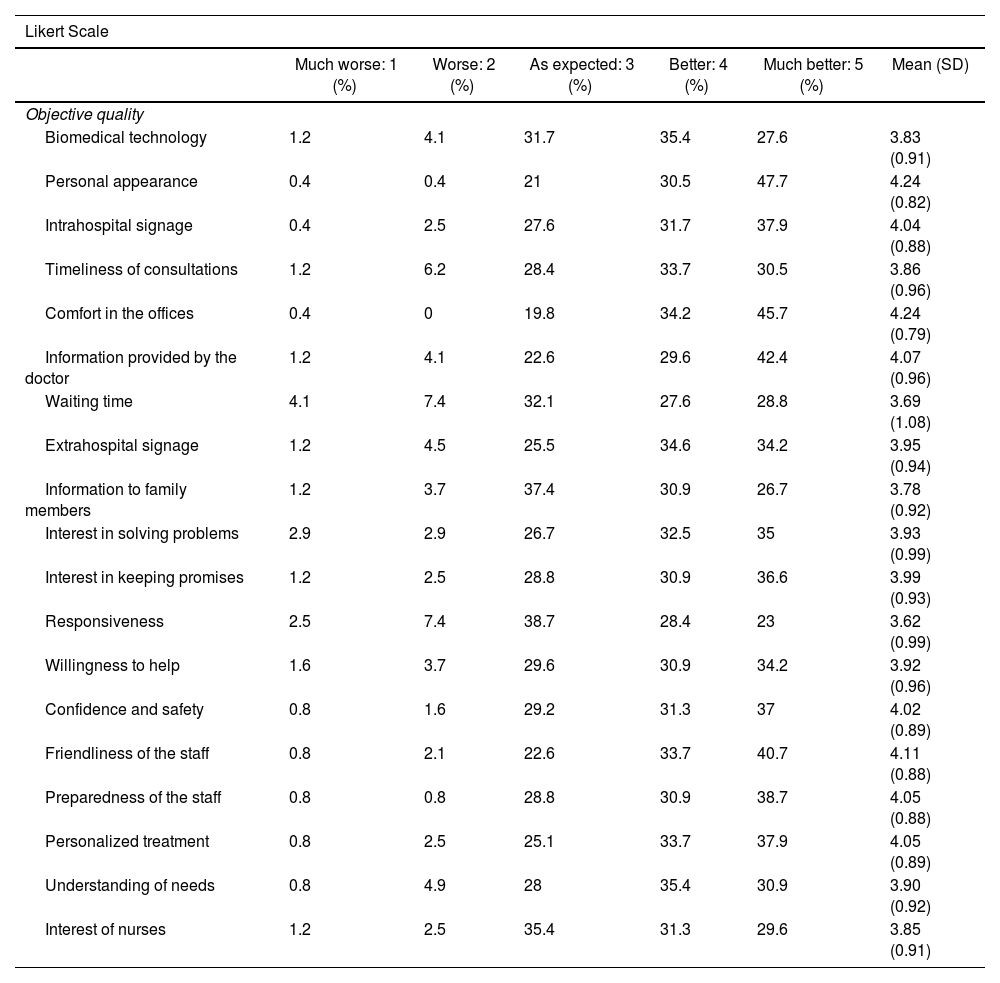
To describe the responses in more detail, Table 2 shows the distribution of the responses for each question in the questionnaire, in which it can be found that high scores of 5 or much better than expected were assigned to questions about the comfort of the offices (47%), information provided by the doctor (42.4%), personal appearance (47%) and friendliness of the staff (40.7%).
Distribution of the response in each question of the questionnaire.
| Likert Scale | ||||||
|---|---|---|---|---|---|---|
| Much worse: 1 (%) | Worse: 2 (%) | As expected: 3 (%) | Better: 4 (%) | Much better: 5 (%) | Mean (SD) | |
| Objective quality | ||||||
| Biomedical technology | 1.2 | 4.1 | 31.7 | 35.4 | 27.6 | 3.83 (0.91) |
| Personal appearance | 0.4 | 0.4 | 21 | 30.5 | 47.7 | 4.24 (0.82) |
| Intrahospital signage | 0.4 | 2.5 | 27.6 | 31.7 | 37.9 | 4.04 (0.88) |
| Timeliness of consultations | 1.2 | 6.2 | 28.4 | 33.7 | 30.5 | 3.86 (0.96) |
| Comfort in the offices | 0.4 | 0 | 19.8 | 34.2 | 45.7 | 4.24 (0.79) |
| Information provided by the doctor | 1.2 | 4.1 | 22.6 | 29.6 | 42.4 | 4.07 (0.96) |
| Waiting time | 4.1 | 7.4 | 32.1 | 27.6 | 28.8 | 3.69 (1.08) |
| Extrahospital signage | 1.2 | 4.5 | 25.5 | 34.6 | 34.2 | 3.95 (0.94) |
| Information to family members | 1.2 | 3.7 | 37.4 | 30.9 | 26.7 | 3.78 (0.92) |
| Interest in solving problems | 2.9 | 2.9 | 26.7 | 32.5 | 35 | 3.93 (0.99) |
| Interest in keeping promises | 1.2 | 2.5 | 28.8 | 30.9 | 36.6 | 3.99 (0.93) |
| Responsiveness | 2.5 | 7.4 | 38.7 | 28.4 | 23 | 3.62 (0.99) |
| Willingness to help | 1.6 | 3.7 | 29.6 | 30.9 | 34.2 | 3.92 (0.96) |
| Confidence and safety | 0.8 | 1.6 | 29.2 | 31.3 | 37 | 4.02 (0.89) |
| Friendliness of the staff | 0.8 | 2.1 | 22.6 | 33.7 | 40.7 | 4.11 (0.88) |
| Preparedness of the staff | 0.8 | 0.8 | 28.8 | 30.9 | 38.7 | 4.05 (0.88) |
| Personalized treatment | 0.8 | 2.5 | 25.1 | 33.7 | 37.9 | 4.05 (0.89) |
| Understanding of needs | 0.8 | 4.9 | 28 | 35.4 | 30.9 | 3.90 (0.92) |
| Interest of nurses | 1.2 | 2.5 | 35.4 | 31.3 | 29.6 | 3.85 (0.91) |
In the bivariate analysis, no relationship was found between the state of satisfaction and age (p = 0.45), socioeconomic status (p = 0.84) or educational level (p = 0.74), but it was found with the number of consultations (p = 0.04) and the place of origin, rural or not (p = 0.03).
The analysis with the group of very satisfied patients evidenced an association with the number of consultations (p = 0.001), the rural area (p = 0.03) and the schooling (p = 0.017), without being statistically significant for gender, age or socioeconomic status.
Regarding the comparison between the rural and the urban population, it can be seen a difference in the percentage of patient satisfaction: in the population of rural origin, 9 of 28 patients had an average satisfaction of less than 4 (32%) and the remaining 68% were very satisfied, while in the urban population 114 of 215 (53%) patients obtained an average of less than 4 or were not very satisfied.
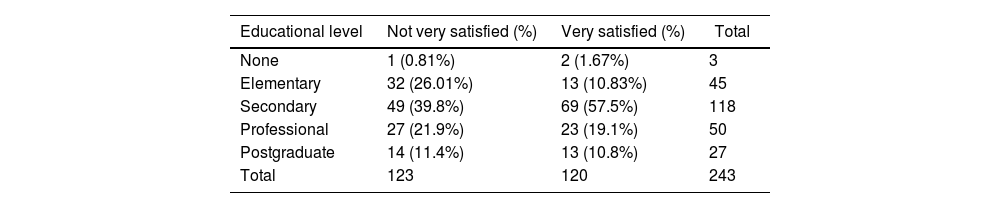
The distribution of the patients who are not very satisfied or very satisfied according to the educational level is exposed in Table 3, since an association was found between these variables.
Percentage of satisfied and very satisfied patients according to the educational level.
| Educational level | Not very satisfied (%) | Very satisfied (%) | Total |
|---|---|---|---|
| None | 1 (0.81%) | 2 (1.67%) | 3 |
| Elementary | 32 (26.01%) | 13 (10.83%) | 45 |
| Secondary | 49 (39.8%) | 69 (57.5%) | 118 |
| Professional | 27 (21.9%) | 23 (19.1%) | 50 |
| Postgraduate | 14 (11.4%) | 13 (10.8%) | 27 |
| Total | 123 | 120 | 243 |
Currently, telemedicine has been implemented for the management and control of chronic diseases that require continuous and strict follow-up. In Colombia, its implementation in the area of rheumatology is beginning, recognizing that technology in the area of information and communication could generate a change in favor of health services, since it has facilitated the entry and opportunity in the provision of services to the population, with an improvement in the offer, increased access to such services in geographical areas where face-to-face service is not possible, and generation of socioeconomic benefits for patients, families, and healthcare professionals.4
In previous studies, it has been found that the overall satisfaction with the provision of services by telemedicine for patients with early or established RA is around the high or very high rating, with data similar to those obtained in our study, such as 90% of satisfied patients among those surveyed, in addition to 49% of patients being very satisfied. The measurements of these studies were made using other non-validated instruments or surveys, unlike this study, in which the SERVQHOS questionnaire designed for this purpose was applied.8–10
When evaluating the relationship between the patients who are very satisfied with the number of consultations received by telemedicine, the rural area or the educational level, no literature has been found that has studied these same associations, which opens the possibility of doing studies that agree with the data obtained here, and not only in consultations carried out in rheumatology services. In this sense, as was to be expected, the level of acceptance is higher the more consultations have been received. Surprisingly, a very good acceptance was found among the rural population, which is not accustomed to the use of technology in their daily lives, and no great difference was found in high educational levels, despite having used much more frequently technological media.
While the research study was conducted, it was evidenced as a strength the fact of having a solid, collaborative work team committed to the study, trained in the areas of general medicine, family medicine and specifically in the areas of rheumatology and epidemiology, which allowed to carry out the clinical and statistical analysis of the data obtained. In addition, there was a tele-rheumatology service enabled for this purpose, with broad experience, and the support of the healthcare provider institution was received, in order to improve health and even economic and social indices in favor of an adequate quality of service.
On the other hand, the difficulties that arose were based, mainly, on the number of patients who could not be contacted for the application of the survey, since both the information and the contact telephone numbers included in the clinical history were out of date, which could lead to additional selection biases. Likewise, the conditions to attend the consultations and the times of opportunity were affected when conducting the surveys during the year of the COVID-19 pandemic. It is of utmost importance to note that the exclusion of patients with only one consultation can increase the risk of selection bias, as well as the external validity of the study, but it also reflects the perception of the patients with better knowledge of the telemedicine service and its operation.
Conducting this type of study in Colombia is of vital importance, taking into account the great difficulties that the country faces in terms of accessibility to health services and the concentration of human talent in large cities, which added to the current pandemic caused by COVID-19 creates an imperious need to improve this type of care, which has become a healthcare model that allows patients with chronic diseases to have adequate control of the disease, thanks to more timely access to medical consultation.
The overall satisfaction assessed in this study reflects a well-accepted way of receiving specialized medical care through telemedicine for patients suffering from diseases such as RA.
The results of the study allow to establish improvement plans for the health care institutions, since the evaluation of each of the applied variables establishes which are the areas that present the greatest difficulties according to the perception of the patients, proposing strategies in favor of improving the quality of attention.
ConclusionsTelemedicine has become a health care model that has gained great value today due to its great benefits in clinical management and in the provision of quality, efficient and profitable health services, especially in those populations that have geographical difficulties or with physical conditions inherent to the disease, as in the case of patients with chronic diseases such as RA. The satisfaction assessed in this cohort, using an instrument validated for this purpose, showed that the majority of patients are satisfied and nearly half feel very satisfied. Additionally, it was found a relationship between the degree of satisfaction and the number of consultations, the origin of the rural area and the educational level.
Conflict of interestThe authors declare that they have no conflict of interest for the preparation of this article.
