





Two cases are presented of rheumatoid arthritis that started during the gestation period, a rare clinical situation and for which no other clinical cases are reported.
Reportamos 2 casos de artritis reumatoide que inician durante el periodo de gestación, situación clínica muy poco frecuente y de la cual no encontramos otros casos clínicos reportados.
Rheumatoid arthritis affects 0.7–1% of the general population, with predominance in females and a higher prevalence in the group of women of childbearing age.1 There is a series of immunological and hormonal changes during the gestation period that could eventually change the immune response and, therefore, the clinical behavior of the already established disease. The onset of rheumatoid arthritis in pregnancy is a phenomenon of very low frequency and without reports in the literature, so we considered that is interesting and pertinent to report these 2 clinical cases of rheumatoid arthritis during the gestation.
Case reportsCase 1A 30-year-old primiparous woman, 30 weeks pregnant at the time of assessment by Rheumatology, with no relevant personal or family history of autoimmune disease, consults for a clinical picture of 4 months of evolution consisting in joint pain of inflammatory characteristics that starts in the left shoulder and which improved with acetaminophen. Subsequently, the joint pain becomes generalized to hands, wrists, knees and hip, and improves with physical activity; she also refers associated morning joint stiffness lasting for 1h.
In the physical articular examination are found 6 painful joints (bilateral proximal interphalangeal 2–4) and 8 swollen joints (bilateral proximal interphalangeal 2–5), with limited range of movement of the carpus due to pain (Fig. 1). Studies for inflammatory arthropathy are started, finding: rheumatoid factor 493IU/ml (normal value<14IU/ml), anti-cyclic citrullinated peptide antibodies 1030.8U/ml (normal value<20U/ml), increased CRP in 2.22mg/dl (normal value 0–1mg/dl), ESR 32mm/h. The ANAs, ENAs and anti-DNA are negative, with complement and hemogram within normal limits.

Given the context of a patient with joint pain of inflammatory characteristics, presence of a high number of swollen and painful joints, with elevation of acute phase reactants and positivization of rheumatoid factor and anti-CCP in high titers, is diagnosed with active early rheumatoid arthritis, with DAS 28 at 5.72. She is considered as a patient with factors of poor prognosis and management is initiated with disease modifiers allowed in pregnancy (hydroxychloroquine, low doses of prednisolone and acetaminophen), with which an adequate control of the symptoms is achieved. The outcome of the pregnancy is a female healthy newborn, without obstetric complications during childbirth. The patient remains in remission during her postpartum, continuing the immunomodulatory treatment with antimalarial agent and glucocorticoid at low doses.
Case 2A 24-year-old primiparous woman, 25 weeks pregnant at the time of assessment by Rheumatology, with no relevant personal or family history of autoimmune disease, consults for a clinical picture of 3 months of evolution, consisting in polyarticular pain of inflammatory characteristics with involvement of hands, wrists, elbows, knees and ankles. She denies the presence of morning stiffness.
In the physical articular examination are found 10 painful joints (bilateral proximal interphalangeal 3–5, wrists, left elbow and right knee) and 10 swollen joints (bilateral proximal interphalangeal 2–5, left wrist and right knee), with bilateral compression test in hands (Fig. 2). Studies for inflammatory arthropathy are started, finding: rheumatoid factor 512IU/ml (normal value<14IU/ml), anti-cyclic citrullinated peptide antibodies>500U/ml (normal value<20U/ml), increased CRP in 16.3mg/dl (normal value 0–1mg/dl), ESR 55mm/h. The ANAs, ENAs and anti-DNA are negative, with complement and hemogram within normal limits.

Given the context of a patient with joint pain of inflammatory characteristics, presence of a high number of swollen and painful joints, with elevation of acute phase reactants and positivization of rheumatoid factor and anti-CCP in high titers, is diagnosed with active early rheumatoid arthritis, with DAS 28 at 6.71. She is considered as a patient with factors of poor prognosis and management is initiated with disease modifiers allowed in pregnancy (sulfasalazine, low doses of prednisolone and acetaminophen), with which a better control of the symptoms is achieved. She currently continues in her third trimester of pregnancy, with a better control of the rheumatoid arthritis and under follow-up, due to high obstetric risk, by the service of Rheumatology of our institution.
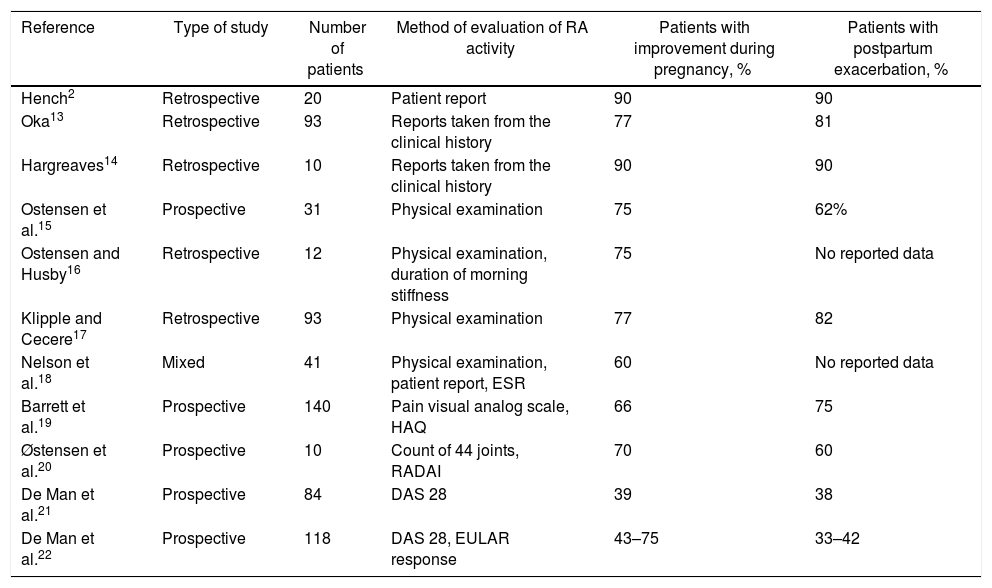
DiscussionIt was conducted a systematic review of the literature seeking information about the diagnosis, prognosis and treatment of rheumatoid arthritis in pregnancy. The following MeSH terms were used: pregnancy, rheumatoid arthritis, diagnosis, prognosis, treatment. The search was carried out in MedLine, Scopus, SciELO and Cochrane, selecting articles in English and Spanish, with no time limit in the publication. The first observation which indicated that the symptoms of rheumatoid arthritis improved during pregnancy comes from the past century, from a publication of Hench in 1938.2 Subsequently, other studies have shown variable values in terms of the percentage of patients who go into remission of the disease, with a trend toward a higher percentage of patients in whom clinical remission occurs (Table 1), although this variability in the results can be explained by the different definitions of remission, given the different instruments used in each of the diverse studies to assess the degree of disease activity (count of swollen and painful joints, clinical concept, DAS 28, RADAI, EULAR response, ESR, among others).
Summary of the studies in which the clinical behavior of patients with rheumatoid arthritis during the gestational and postpartum period has been evaluated.
| Reference | Type of study | Number of patients | Method of evaluation of RA activity | Patients with improvement during pregnancy, % | Patients with postpartum exacerbation, % |
|---|---|---|---|---|---|
| Hench2 | Retrospective | 20 | Patient report | 90 | 90 |
| Oka13 | Retrospective | 93 | Reports taken from the clinical history | 77 | 81 |
| Hargreaves14 | Retrospective | 10 | Reports taken from the clinical history | 90 | 90 |
| Ostensen et al.15 | Prospective | 31 | Physical examination | 75 | 62% |
| Ostensen and Husby16 | Retrospective | 12 | Physical examination, duration of morning stiffness | 75 | No reported data |
| Klipple and Cecere17 | Retrospective | 93 | Physical examination | 77 | 82 |
| Nelson et al.18 | Mixed | 41 | Physical examination, patient report, ESR | 60 | No reported data |
| Barrett et al.19 | Prospective | 140 | Pain visual analog scale, HAQ | 66 | 75 |
| Østensen et al.20 | Prospective | 10 | Count of 44 joints, RADAI | 70 | 60 |
| De Man et al.21 | Prospective | 84 | DAS 28 | 39 | 38 |
| De Man et al.22 | Prospective | 118 | DAS 28, EULAR response | 43–75 | 33–42 |
The mechanism by which rheumatoid arthritis would tend to improve during pregnancy is not fully elucidated; however, it is considered that pregnancy is a clinical situation of immunological tolerance induced by the semialogenic fetus. This is due to different factors that include several immunological processes, among which stand out: thymic involution, decreased activity of NK cells and decrease in the immune response in Th1 lymphocytes with shift toward Th2 activity.3 In addition, the syncytiotrophoblast expresses molecules that inhibit the complement, as it is the case of the decay-accelerating factor and the membrane cofactor protein, which protects the embryonic cells against complement-mediated lysis.4 From the point of view of cellular immunity, it should be noted that the activation of T cells in the maternal–fetal interface is inhibited by the local expression of indoleamine 2–3 dioxygenase, which degrades tryptophan, an amino acid that is essential for the activation of T-cells.5
In the 2 cases reported, we found patients with clearly inflammatory joint pain, with presence of a high count of swollen and painful joints and with paraclinical tests results compatible with rheumatoid arthritis. The diagnosis of individual cases is clear, given their florid presentation; however, the clinical peculiarity that motivated us to publish these cases lies in that the patients begin their symptoms while pregnant, a very infrequent situation in clinical practice, without being able to identify other reports of similar cases of onset of rheumatoid arthritis during pregnancy. When we carried out the search of literature we found 3 cases of adult-onset Still's disease that begin during the gestation period,6–8 but no case of rheumatoid arthritis.
Patients with rheumatoid arthritis may require pharmacological treatment during pregnancy. In this context, the options are limited not only by the disease activity, but also by concerns related to fetal toxicity.9,10 The drugs most frequently used for the treatment of rheumatoid arthritis can be divided into 4 categories according to their risk for fetal development:
- •
Drugs with a moderate to high risk of fetal damage: methotrexate and leflunomide are found in this group, with a high risk of causing birth defects, such as congenital malformations of the central nervous system, cerebral palsy, alterations in the ossification of the cranium, extremities and palate, so they should be avoided during the conception and pregnancy. These drugs must be discontinued at least 3 months and 2 years before conception, respectively, due to their prolonged retention in the tissues.11,12
- •
Drugs that can be used selectively during pregnancy: this group includes the glucocorticoids such as prednisone, prednisolone and methylprednisolone, which cross the placenta in low concentrations and are relatively safe for their use in pregnancy when they are used in low doses.24 Non-steroidal anti-inflammatory drugs can be used safely during pregnancy with certain considerations, such as being avoided during preconception and early pregnancy, since they can interfere with the implantation of the embryo; likewise, they should be avoided in the third trimester because of the risk of premature closure of the ductus arteriosus.25,26 Inhibitors of the tumor necrosis factor can also be used electively, since it has been determined that the risk of congenital defects in patients exposed to this type of drugs is low.27,28
- •
Fetal and maternal minimum risk: these are drugs that can be used during pregnancy; hydroxychloroquine and sulfazalazine are included here. Azathioprine, the antirheumatic drug most commonly used in lupus and other connective tissue diseases is also included in this group.21,29
- •
Unknown risk: in this group are the drugs in which the tests related to the risks are insufficient, and includes certain biological agents, in which their continuity during pregnancy should be agreed with the mother, who must receive information on the potential risks of this medication in case of deciding to continue it during pregnancy. Rituximab, abatacept, tocilizumab and tofacitinib are found within this group.30
We report two separate cases of appearance of rheumatoid arthritis in the second and third trimesters of pregnancy, an unusual phenomenon in clinical practice, without finding other reports of similar cases in the literature.
Conflict of interestThe authors declare they do not have any conflict of interest.
Please cite this article as: Fernández-Ávila DG, Rincón-Riaño DN, Gutiérrez JM. Inicio de artritis reumatoide durante el embarazo. Rev Colomb Reumatol. 2018;25:141–145.
