









Knowledge translation (KT) not only encompasses a series of final actions in areas of dissemination, but also the identification of strategies for the implementation of this process.
ObjectiveTo evaluate the effectiveness of KT strategies in audiovisual language compared with other languages to improve health outcomes in the general population.
MethodsWe performed a search in MEDLINE, CENTRAL, PsycARTICLES, the WHO International Clinical Trials Registry Platform, EMBASE and LILACS.
ResultsWe included 63 studies encompassing a broad range of study populations, languages that were compared to audiovisual language and measurement scales for outcomes. These studies presented a high risk of bias and the quality of evidence was not sufficient to draw conclusions about the effectiveness of the evaluated languages for knowledge translation.
ConclusionsWe identified different languages that could be used in knowledge translation. The knowledge and the effects produced as a result of the strategy diminish as time progresses, regardless of the type of language used. This is an important point to consider when implementing this type of strategy.
La transferencia del conocimiento (KT) corresponde no solo a una serie de acciones finales en áreas de divulgación, sino a la identificación de estrategias para la realización de este proceso.
ObjetivoEvaluar la efectividad de estrategias de KT en lenguaje audiovisual comparadas con otros lenguajes para mejorar los desenlaces en salud de la población general.
MétodosSe realizó una búsqueda en MEDLINE, CENTRAL, PsycARTICLES, WHO International Clinical Trials Registry Platform, EMBASE y LILACS.
ResultadosSe incluyeron 63 estudios; se observó gran variabilidad en las poblaciones de estudio, así como en los lenguajes comparados con el lenguaje audiovisual y los instrumentos de medición. Los estudios tienen alto riesgo de sesgo y la calidad de la evidencia identificada no permite llegar a una conclusión respecto a la efectividad de los lenguajes evaluados en KT.
ConclusionesSe identifican diferentes lenguajes que pueden emplearse para transferir conocimientos. Se evidencia que el conocimiento y los efectos producidos por la intervención disminuyen a medida que avanza el tiempo, independientemente del tipo de lenguaje empleado. Por lo tanto, es el tiempo es un punto importante a tener en cuenta en este tipo de intervenciones.
There are various perspectives from which health communication (HC) is analysed depending on the nature and specific aim of the action. Three of the most relevant models are research, education and communication (REC), risk communication and, over the last decade, the communication for social change perspective. These models have experienced a boom, especially in the development of strategies seeking to shape actions associated with prevention and health-related decision-making.1–3
In this vein, health communication processes are closely tied to specific knowledge translation (KT) dynamics, a concept which is being continually developed in different sectors of society; for example, in the relationship between universities and businesses or the commercial sector, in different levels of institutional organisation and in relation to the field of health, among others.4
With regard to the latter, the correspondence between HC and KT has been established, with the latter taking elements and processes from HC, which can vary depending on the model adopted and which structure the series of specific translation actions, which in turn explains the variation between existing KT models such as that of the Canadian Institutes of Health Research (CIHR) based on the knowledge-to-action framework developed by Graham et al.,5,6 and the models of Eroglu et al. that place greater emphasis on knowledge diffusion and disclosure practices, whereas the former is more interested in influencing the day-to-day dynamics of populations.7,8
In this sense, KT is recognised as the nexus between research, academia and the practice of the health sciences, boosting and improving results in health, including the planning and design of actions.9,10 KT seeks to reduce the gap between knowledge producers and users11; however, it does have some limitations in the characterisation of procedures to develop specific actions in health, as well as in proposing strategies that allow the effectiveness of KT to be measured in specific contexts, particularly in non-personalised interventions.5
Eroglu et al. view KT as a complex process involving the interaction of different social groups, in which knowledge production is not a construct that exists outside of society, rather it happens within it, based on society's interests, codes and systems, such that the data and information take on meaning, as well as involving ongoing relationships between the agents participating in joint dynamics.12
Description of the interventionAudiovisual language is a set of symbolic elements and standards for use in a communication context. It is characterised in that, like most languages, it possesses morphology, syntax, semantics, aesthetics (a major characteristic in comparison with other types of language) and didactics, and is gaining ground with its images, which prevail and which represent us.13,14
In the context of the audiovisual communication system, priority is given to multisensory (visual and auditory) transmission, which facilitates the processing and global integration of information, which translates to a unified and time-limited experience. In this way it resembles synthetic languages; in other words, it only has meaning if perceived as a set.
Finally, it mobilises the emotions before the cognitive processes; it is however a trigger for the latter, the numerous emotional stimuli propelling the generation of cognitive messages and interaction with them. As Eisenstein wrote, “From image to emotion, from emotion to thesis”.15
Different research results reveal that audiovisual language facilitates communication processes independently of language, bridging the gap between known and/or unknown realities, although there is some relativity in that speakers of different languages interpret it and relate to it from different points of view depending on the specificity of the available categories.15
It has been confirmed, from different analysis perspectives, that the contributions of audiovisual language have a continuous relationship with cognitive and psychological aspects that personalise the message and are associated with behaviour in a wide range of different cognitive processes, including categorisation, classification, recognition and perception.5
Scientific findings in the field of health do not represent a positive or negative change unless they are effectively translated not only to health professionals, but also to the general population. Effective knowledge translation increases the actual effectiveness of the interventions or strategies promoted. The results of this review may be useful for implementing health interventions or strategies using mass communication strategies.
For the reasons discussed above, this review's objective is to assess the effectiveness in the general population of KT strategies, including audiovisual language compared with other languages, in improving outcomes in individual health and the general population.
MethodsThe inclusion criteria for studies were: cross-sectional and cluster randomised clinical trials in the general population (regardless of whether they have any type of disease or belong to any vulnerable group) comparing the application of KT strategies using audiovisual language with any other type of language.
The primary endpoints considered were adherence to treatment and health programmes, attendance at medical appointments, changes in lifestyle and level of memory retention, while the secondary endpoints were changes in physiological variables, reduction in mortality and reduction in length of hospital stay.
Nevertheless, given the broad and variable definition of KT, endpoints of any type were taken into account.
Search strategyA systematic search was conducted between February and March 2016 in the MEDLINE (OVID), CENTRAL, PsycARTICLES, WHO International Clinical Trials Registry Platform, EMBASE and LILACS databases (search strategies can be seen in Appendices 1–6). A search of the following resources was also carried out: grey literature through Open Grey and Google Scholar (1 March 2016), manual search of the references of articles and/or books associated with the subject, as well as the list of references of the articles included.
Analysis and data collectionFour authors (LM, MS, NM, SL) independently selected the studies based on titles and abstracts. In case of disagreement, the authors discussed and attempted to reach an agreement. If this was not possible, the opinion of another author (LB, NG, NS) was sought. The articles selected after this first screening were included for full text review. All authors reviewed the full text of the articles using the inclusion and exclusion criteria.
Data extraction and processingOn reviewing the full text of the included articles, the characteristics of interest of each study were entered into an Excel spreadsheet for data extraction. Information on the authors, year of publication, audiovisual language used, comparator, main results, study type, missing data and other observations that might be relevant to the review were recorded.
Assessment of the risk of bias of the studies includedThe Cochrane Handbook for Systematic Reviews of Interventions bias risk assessment tool16 was applied to the studies included to qualify each risk encountered as low, high or unclear.
Measurement of the effect of the interventionMeasurement of the effect varied depending on the endpoint variable presented in each study. If the endpoint was measured using a dichotomous variable, the effect was assessed using the relative risk or odds ratio (OR) with their respective 95% confidence interval (95% CI); for endpoints with continuous variables, the effect was assessed using the mean difference or standardised mean difference.
The analysis unit of interest was individuals put in contact with KT strategies; cluster-based studies were also taken into account.
Management of missing dataIf a study did not present sufficient information to measure the effect of any endpoint, the study's authors were contacted to obtain clarification on the results. If there was no response, the decision was made to not include results for an endpoint with a large quantity of missing data in general effect measurements, but a narrative description of the result was given.
Heterogeneity assessmentNo sensitivity analysis was performed due to the high degree of heterogeneity. This was assessed qualitatively by means of a visual assessment and study differences based on logic. The high degree of heterogeneity observed is due to the differences between the populations, measuring instruments and endpoints encountered in the studies, and means that this review is unable to assess the general effect of all the interventions.
Evidence quality assessmentThe GRADE tool17 was used to assess the quality of the evidence for the endpoints of the interventions in question, taking into account the risk of bias, inconsistencies, indirect evidence and the imprecision of each endpoint of interest.
Data synthesisThe results estimates were combined based on study design; results from studies with different types of design or intervention were not combined. Due to the heterogeneity of the studies, it was not possible to determine an overall effect (meta-analysis). A complementary narrative synthesis for the analysis was prepared, which helps to explore the intervention processes.
ResultsThe studies included are described in the tables of characteristics of the studies included (Annex A). Initially, 3827 references were identified after eliminating duplicates in the first screening; 193 articles were then selected based on the title and abstract for full text review, 63 of which were ultimately included in the review (Fig. 1).
Study designs.")
Sixty-three randomised clinical studies were included.18–80 The intervention follow-up time varied considerably between the studies included (from 2 weeks to 24 months) and very few studies communicated the mean follow-up or follow-up interval.
Participants and toolsAmong the studies included there is a high degree of variability in the study populations and the languages compared with the audiovisual intervention. There were few occasions where the measuring instruments were similar. Choices of follow-up times were not backed up by theoretical justification, suggesting that they are more closely linked to the instrument rather than the endpoint measured. This situation makes it difficult to measure KT in the endpoints found.
The population groups encountered include the following: Seven studies focussing on groups of adolescents,26,31,47,48,69,71,78 five on groups of pregnant women,29,50,64,68,74 five on patients with cancer,28,32,34,42,44 three on groups of diabetic patients,39,56,59 three on groups of paediatric patients,19,58,65 three on groups of patients with heart disease51,75,79 and three on groups of surgical patients,30,40,77 as well as groups such as asthmatic patients, hospitalised patients, burn victims, healthy volunteers, etc.
Description of the interventionIn all of the studies included, the intervention was audiovisual language (video, multimedia, audiobook); some were accompanied by written languages or oral advice. The comparator languages included written media, oral advice or standard information (Annex A).
EndpointsThere was a high degree of variability in the endpoints of the studies included. This is due to their having been assessed using different scales which were rarely comparable with those of the other studies included.
Primary endpointsThirty-one studies assessed the knowledge or memory retention endpoint using questionnaires created for the research; of these, only two used a knowledge scale52,53; four studies assessed adherence to treatment, each using a different scale based on the population assessed.
Secondary endpointsNo endpoints were found that focussed on reduction of mortality or length of hospital stay. The changes in biological variables endpoint was observed in four studies: reduction of dental plaque, hypoglycaemia and reduction in the weight of patients with heart failure. Each of these studies was conducted in a different type of population, and in three of them57,59,80 significant changes in biological variables were observed with audiovisual language. Endpoints such as anxiety, self-assessment, reduction in symptoms, behaviour, depression, satisfaction and perception, among others, were also revealed (Annex A)
Studies excludedArticles were excluded based on methodological criteria (Annex B). Articles were excluded at the full text stage if they were found to be before-and-after studies, if the comparator was also an audiovisual language, if it was not possible to obtain the full text of the article, or if the publication was a conference abstract with little information on methodology.
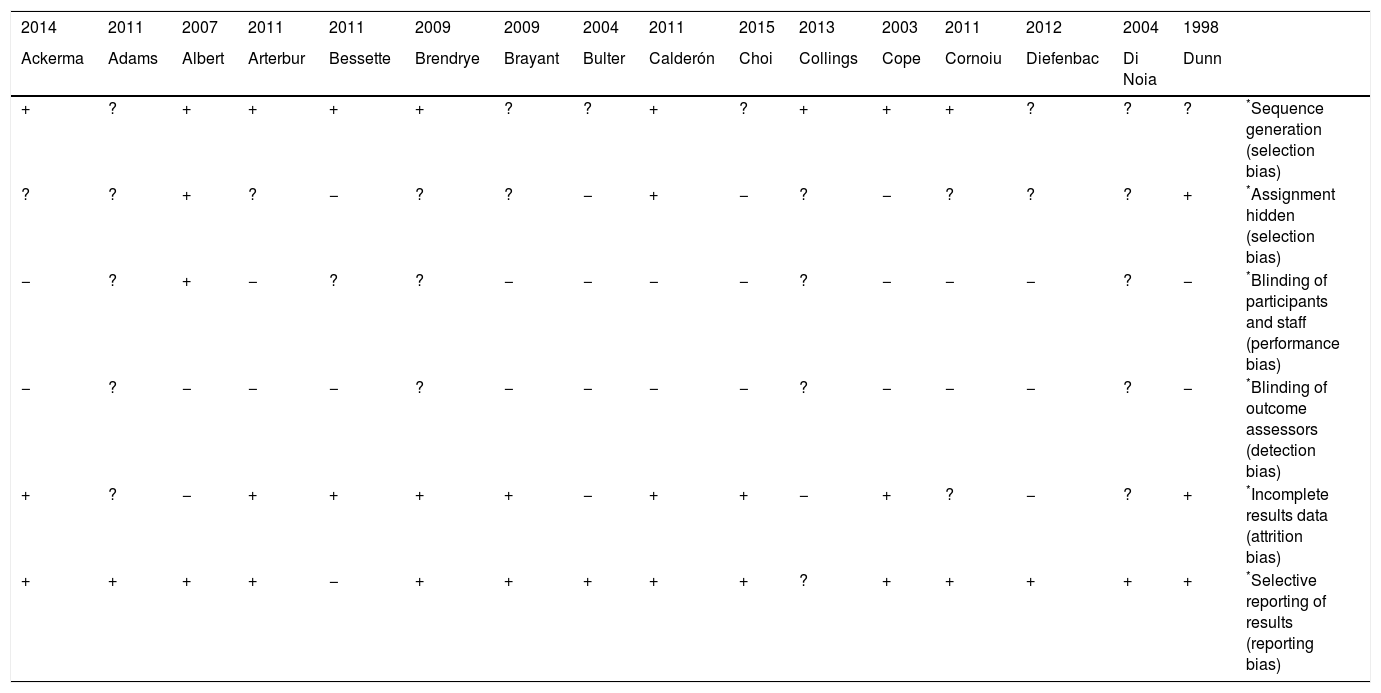
Risk of bias of the studies includedThe most common high risks of bias were blinding of the assessor and of the participants from the assessor, and incomplete data (Fig. 2, Appendix 7 and Annex A).
Effects of the intervention
It was not possible to obtain the effect of the intervention (audiovisual language) due to the heterogeneity of the population and the different types of measurement and endpoints assessed. For the knowledge or memory retention endpoint, it was possible to perform a group analysis of some studies as the measurements were expressed in the same units and the interventions were the same (Figs. 3–5) using standardised mean difference (SMD), but no general effect was obtained due to the heterogeneity of the study populations.

.")

In spite of this, Annex C details the group analysis effect, showing an effect in favour of audiovisual language. The analysis in Fig. 3 obtained a SMD of 0.75 (95% CI 0.56–0.93).26,33 For the comparison of correct responses to knowledge items between audiovisual language and written material (leaflet) (Fig. 4), the SMD was −0.34 (95% CI 0.57–0.11).21,62 Meanwhile, the analysis in Fig. 5 obtained a SMD of 3.16 (95% CI 1.54–4.78).30,52,53 It is worth highlighting that the quality of the evidence for these endpoints was very low to low.
Again, in Annex C, studies can be seen with a low quality of evidence and high risk of bias that show an effect in favour of audiovisual language; the 2003 study by Krishna, with 12 months’ follow-up, shows a mean difference in the change in knowledge between the audiovisual language (multimedia) and oral advice plus written information groups of caregivers for children from 0 to 6 years of age of 5.39 (95% CI 2.12–8.66); this change in knowledge was also seen for children from 7 to 17 years of age, with a mean difference of 5.56 (95% CI 2.15–4.61).49
These low-quality studies also included some that found effects in favour of audiovisual language, but that were not statistically significant. The study by Eaden, with one month's follow-up found a mean difference in the percentage change in knowledge of colonoscopy and cancer risk between audiovisual language (video) accompanied by written information and written information alone (leaflet) of 18.3 (95% CI −6.33 to 42.93).34 Another study conducted in 2008 with one week's follow-up also found audiovisual language (multimedia) to be better than written information alone, with a mean difference in the percentage of knowledge of 4.3 (95% CI −3.92 to 12.52).48
Since it was not possible to measure the general effect of KT interventions, what follows is a narrative description of the effect in the population groups encountered.
In the studies on the group of pregnant women, Cope et al. did not find significant differences between groups for the depression endpoint, but did find lower levels of anxiety in the intervention group than in the control group.29 Other authors similarly failed to find differences between the intervention and control groups,50,64 but did consider that audiovisual media could have benefits for women with low literacy levels,64 and contributes to improving attitudes to stopping smoking among pregnant women, as well as to definitively stopping said habit, compared with printed information alone.68
In the group of patients with cancer, both the visual and written interventions implemented were able to increase knowledge, which could lead to improvements in treatment and the information given to patients and/or their carers.28 Moreover, when the format used is a multimedia programme, the findings were improved comprehension regarding the treatment, reduced anxiety, greater confidence in treatment options and being better informed to make decisions about treatment.32 On the other hand, in situations such as radiotherapy treatment, giving prior information in a video versus a written format did not lead to advantages in health outcomes.34
In the group of patients with diabetes mellitus, the studies covered interventions that would enable them to prevent clinical risks, including education programmes, elements targeting specific preventive measures in these patients, and focussed and attractive information allowing greater acceptability.39,56,80 A lower incidence of hypoglycaemia was observed in patients receiving visual material and leaflets with a self-assessment and treatment plan.39 With regard to positive outcomes such as weight loss in individuals at risk of contracting diabetes mellitus, it can be seen that an intervention consisting of a cable television programme can help with weight loss as a health promotion and prevention measure in this population.56 Regarding patients’ glucose control and weight, a randomised clinical trial reported a negative result for audiovisual education programmes in diabetes, after observing no benefit in these two variables.80
With regard to the effect of the intervention on the paediatric population, no statistically significant differences were found in the impact of the various interventions.19,58,65 Redsell et al. identified that the use of multimedia material or the use of leaflets for healthcare and psychosocial outcomes in children with enuresis did not lead to a better prognosis in their treatment. This could be associated with the children's prior knowledge of their disease, which would diminish their interest in these tools. For this reason, it was concluded that such interventions should be personalised.65 In contrast, the use of audiovisual media and leaflets for parents on the primary care of their children had a greater impact on changing the habits of their children in terms of exposure to violence through communication media.58 Nevertheless, the use of leaflets and videos for parental knowledge of procedures and complications of surgical interventions did not improve memory or the retention of the information beyond that given by the surgeon during the consultation.19
On the effect of the use of a multimedia format in the group of patients with heart disease, it could be thought to be useful because most hospital readmissions are due to lack of adherence, insufficient knowledge of the diet the patient must follow, how to appropriately use the medication and how to identify the symptoms of heart failure.51 However, to our knowledge, no study has been able to demonstrate a statistically significant benefit. In the group of patients with AIDS and heart failure, a benefit was seen in the improvement of fluid control and uptake of low-sodium diets with the implementation of DVD education.75 Lastly, the study in patients due to undergo catheterisation demonstrated that digital education combined with group therapy reduced anxiety levels and improved patient satisfaction, although the authors also propose this method for routine use in the care of patients with heart disease.79
In contrast, in the group of surgical patients, due to the greater complexity of the orthopaedic surgical procedures and the higher expectations of patients’ with regard to the outcome of the surgery, obtaining true informed consent is extremely difficult.30 In the group of surgical patients with knee arthroscopy and in the group of patients undergoing radical prostatectomy, the effect of implementing multimedia resources was found to be a significant improvement in patient comprehension and retention of the information and a reduction in the risk of possible medico-legal disputes when the ideal result was not achieved.30,40 In the group of patients who received audiovisual education on prostate-specific antigen (PSA) screening, there was an increase in the number of patients who chose to actively participate in screening.40 However, the study with patients with planned laparoscopic cholecystectomies emphasises that no multimedia format is going to replace personal interaction and that it should only be used as an additional support.77
Exhaustiveness and applicability of the evidenceThe evidence found in this review of the effectiveness of audiovisual language strategies to achieve KT highlights the existence of a body of theoretical work on KT; however, it is not sufficient to determine the level of effectiveness associated with audiovisual strategies in comparison with other types of languages, meaning that its applicability is limited.
Although the information found is not sufficient to perform an analysis of its effectiveness, it has been possible to identify some of the most used methods of KT in healthcare for the general population.
These elements could be taken into account in future investigations in this area; they may also serve as a basis to consider possible interventions with the objective of transmitting relevant information to the general population.81–83
DiscussionThis brings to light the numerous strategies, programmes, actions and interventions developed with the aim of improving health outcomes, using different languages, graphic designs and strategy combinations; however, the methodology used in making these decisions is not clear, which may correspond with the emphasis in highlighting the improvement, neutrality and/or alteration of the health outcome of interest.
The numerous strategies in existence make use of different digital resources and technological repertoires, such as communication technology, but in presenting the evidence a lesser degree of relevance is given to the intervention, such that it is not possible to extract the real impact of these strategies, which was a factor in the results of this review.
Regarding formats classified by language, a high degree of variety was revealed. The most used are “clip” type audiovisual formats, with 2D graphics predominating over 3D; booklets and/or printed materials on the subject of interest; and, to a lesser extent, games or multimedia.
Due to the high degree of heterogeneity in the studies in terms of population, intervention and how outcomes were measured, a description of the most relevant population groups is provided (Table 1), which qualitatively shows the superior performance of the audiovisual format over other formats in specific population groups.
Qualitative description of the endpoints of comparisons of the audiovisual language format with other formats for the most relevant population groups identified in the studies included.
| Population | Article | Topic | Interventions compared | Conclusions | Observation |
|---|---|---|---|---|---|
| Adolescents | Calderón et al.84 | HIV prevention | [Video] versus [Oral advice] | Video intervention reduces lack of knowledge Increases participation versus oral intervention | Future research needed to come to a recommendation or choose the best intervention |
| Di Noia et al.85 | [Multimedia] versus [Traditional strategies] | Multimedia interventions can improve knowledge of HIV/AIDS They help to reduce the risk of self-efficacy in adolescents | |||
| Klein47 | [SiHLE multimedia] versus [traditional health education session] | Can disseminate health-related content at low cost, which can have an impact on risk reduction in behaviours associated with HIV transmission | Adolescent and African-American population | ||
| Koch et al.48 | Education on acne vulgaris | [Multimedia] versus [Printed information (leaflet)] | Both interventions have equivalent benefits in terms of knowledge gained in the short and long term among adolescent patients with acne | ||
| Shrier et al.69 | Patients diagnosed with gonorrhoea or chlamydia Sex education | [Personalised video] versus [standard information] | Video can improve condom use Reduces the number of adolescent couples who have had a sexually transmitted disease | Future studies with bigger samples needed to determine the definitive effects of this intervention | |
| Srai et al.71 | Patients with orthodontic devices | [Multimedia+oral information] versus [Oral information] | Providing additional audiovisual information does not significantly reduce anxiety levels in adolescents with orthodontic devices | ||
| It may be more profitable and beneficial to disseminate this information on social networks or in waiting rooms | |||||
| Windham et al.78 | Knowledge of obesity | [Multimedia+routine care] versus [routine care] | Both interventions improve measures of motivation to lose weight and diet-related aspects The multimedia intervention helped to improve parental knowledge | Results indicating that it is better than conventional treatment were not observed | |
| Pregnant women | Cope et al.29 | suspected foetal anomaly with the aim of reducing anxiety | [Written information+recording] versus [standard information or written information or recording] | Providing additional material, especially a recording, during prenatal checks appears to reduce the level of anxiety compared to routine practice | All on different subjects |
| Combining the recording+written information does not appear to increase or decrease patients’ ability to retain the key aspects | |||||
| Leung et al.50 | Decisions regarding prenatal screening for Down's Syndrome | [Multimedia+video+leaflet] versus [Video + leaflet] | Women in the intervention group had a better understanding There was no difference in the final decision on whether to take the test | ||
| Raynes et al.64 | First-time mothers planning a vaginal delivery | [Written information (leaflet)+audio-assistance] versus [leaflet] | No differences were found in the results in knowledge or anxiety levels between the two groups | ||
| Secker et al.68 | Interventions to reduce cigarette use in pregnant women | [Advice+video+a suggestions sheet] versus [Advice+suggestions sheet] | The use of video shapes the change in smoking behaviour | ||
| In may increase the efficacy of support to stop smoking | |||||
| Szmeja et al.74 | Advice on overweight and obesity in pregnancy | [Written material+consultation+video] versus [Written material+consultations] | Providing an informative video was associated with an improvement in diet quality at 36 weeks pregnant It was not associated with changes in physical activity or weight gain | ||
| Cancer | Collinge et al.28 | Patients with cancer | [Multimedia] | Multimedia formats can provide certain additional benefits aside from the knowledge they can transmit Instructions given to carers using a multimedia strategy lead to an increase in satisfaction with the care provided It is an easy strategy to apply for teaching massage techniques | Knowledge translation is essential in various healthcare processes, for example, an adequate strategy can provide useful information for patients allowing greater autonomy when making decisions on their care as they will be informed and appropriately supported. |
| Diefenbach et al.32 | Patients with cancer | [Multimedia] | The use of this strategy was associated with increased confidence with regard to treatment options The information provided in the various formats supports the information provided by the healthcare professional | ||
| Eaden J, et al.34 | [video] versus [leaflet] | The use of distinct formats in a single intervention improves patients’ level of knowledge | |||
| Harrison R, et al.42 | [video cassette] versus [written information] | During the knowledge translation, different instruments were identified and assessed The follow-up time varied considerably. Some studies performed follow-up beyond one year. In knowledge translation, it is essential to perform long-term assessments or follow-ups in order to really see the link between the process and the effects. | |||
| Hutchison et al.44 | Patients with cancer | [Audiovisual] | The intervention did not change the rate of cancer patients turning down participation in clinical trials | ||
| It was found that patients have a higher level of knowledge that may affect decisions | |||||
| Diabetic patients | Glasgow et al.39 | Diabetic patients | Participants were allowed to choose the type of intervention they preferred. Most opted for DVD | Unless all the different intervention formats contained the same information, the degree of knowledge could vary Patient preferences may be a factor in the development of certain preference-oriented strategies to improve their reach | |
| Mulrow et al.56 | [Conventional information] versus [informed consent-type information letters] versus [leaflet] | Carrying out knowledge translation interventions is associated with acceptance by the users or receivers of the information | |||
| The expected results were not obtained for any of the formats assessed. Loss of patient motivation was revealed, as they may have already experienced several education strategies in various formats. This suggests that this group had received the maximum benefit from educational processes | |||||
| Nordfeldt et al.80 | [Traditional clinical follow-up] versus [questionnaire] | This type of intervention may work better as a facilitator in a discussion and not alone as a didactic message | |||
| Paediatric patients | Adams et al.19 | Patients in consultations prior to adenotonsillectomy | Pre- and post-intervention [oral advice+leaflet] versus [oral advice+video] | Regardless of format, patients were not able to identify all the risks associated with the procedure Better retention of the information was found when the time between the training day and procedure was shorter | |
| Neely et al.58 | Reduction of habits associated with exposure to violence | [Audiovisual series] versus [leaflet] | Exposure to various media can have different effects on consumption habits and exposure to violence This type of intervention may contribute to preventing exposure to violence | ||
| Redsell et al.65 | Patients with nocturnal enuresis | [Multimedia] versus [written leaflets] | Multimedia programmes are no more effective than traditional materials in influencing health-related behaviours | ||
| Patients with heart disease | Linné et al.51 | Adult patients with heart failure | [Multimedia+conventional information] versus [traditional information] | Additional information in multimedia formats does not have a greater effect on readmission rates or death within the next 6 months This low effectiveness may be linked to sample size A small variation was found between the two interventions, but it is not conclusive | |
| Veroff et al.75 | [Multimedia DVD+leaflet] versus | The use of different low-cost formats contributes to changing behaviours | |||
| [basic informative programme] | The use of DVD, leaflets and programmes may facilitate self-care processes in patients with heart failure | ||||
| Wu et al.79 | Anxiety reduction | [Regular education] versus [multimedia education strategy] versus [anxiety questionnaire] | Patients who had access to multimedia information reported a slight reduction in anxiety This type of format can become a supplement to patients’ regular care in the future | ||
| Surgical patients | Cornoiu et al.30 | Mechanisms to improve informed consent processes for orthopaedic surgeries | [Multimedia]+[oral advice]+[informative pamphlets] | Patients exposed to multimedia demonstrated greater and more correct correspondence in completing the questionnaire versus the oral advice and informative pamphlet groups | |
| There was no evidence of reductions in anxiety Better information retention processes were identified up to 6 months after surgery | |||||
| Gyomber et al.40 | Patients with upcoming radical prostatectomy | [standard informed consent] versus [multimedia presentation] | The multimedia format suggests better understanding of the implications of the surgery Knowledge of the risks and aspects of the procedure is increased Patients had more consistent explanations and more active participation | It is the only research report that makes use of legal and ethical concepts and considerations | |
| If the tools take ethical information and legal informed consent into account, they could increase patients’ knowledge, as well as reducing their anxiety and potential medico-legal distraction and its consequences | |||||
| Wilhelm et al.77 | Patients undergoing laparoscopic cholecystectomy | [Multimedia] versus [traditional presentation] | Patients could be better informed using multimedia strategies regardless of surgical procedure A positive impact on the knowledge of patients exposed to multimedia resources was found. | The only study to look at the efficacy of the tool as well as considering the role of human labour as an irreplaceable resource | |
| However, a multimedia tool cannot replace personal interaction and daily support | |||||
The evidence identified does not allow a conclusion to be reached on the effectiveness of the languages assessed for KT, although it does enable us to identify possible languages and the frequency with which they are used.
The review included 63 experimental studies, all with a randomised design, incorporating a total of 6884 participants; the methodological quality of these studies was assessed using the GRADE methodology, with the evidence quality generally being classified as low or very low, although some studies attained moderate quality (Annex C). The limitations encountered were associated primarily with the risk of bias of the studies and the imprecision of the results. Consequently, the studies found are considered to be of low quality.
In using the GRADE methodology to assess evidence quality, no adequate grouping of the principal endpoints was possible as the way in which they were assessed varied not only due to the high diversity of the instruments used, but also due to the study populations, the follow-up time, the interventions and the comparators.
The results of the studies were in most cases in favour of interventions using audiovisual language; however, on analysing the data in the studies for which they were available using standardised means, this result was not upheld.
Potential biases in the review processThis review aims to identify endpoints spanning the KT process. For this reason, a wide variety of endpoints was included, which could limit the analysis due to the high degree of heterogeneity. Another possible bias of the review is limitation in terms of language, as only studies in English and Spanish were included.
ConclusionsImplications in practiceDifferent languages that can be used to transfer relevant knowledge on healthcare to the general population have been identified. Audiovisual language formats such as videos, multimedia tools, and talks and audio recordings accompanied by a visual format have been found to offer better knowledge translation in specific populations, although it should be noted that the quality of the evidence in these studies varies from very low to moderate. In general, the majority of the studies assessed reflect the fact that the knowledge and effects generated by the intervention erode over time, regardless of the type of language used, meaning that it is important to take follow-up into account in KT interventions of this type.
Implications in researchKT has been found to improve with the support of audiovisual formats, although the quality of the evidence in the studies included is low with a high risk of bias. For this reason, new experimental studies are needed with a more careful design that is suitable for drawing appropriate conclusions on the effectiveness of KT interventions. The importance of using validated instruments to measure knowledge and the need for these to be standardised so that the results obtained can be compared over time should also be borne in mind.
FundingResearch funded and conducted through the Programa Jóvenes Investigadores e Innovadores [Young Researchers and Innovators Programme] 645-2014 COLCIENCIAS, Traditional system.
Publication prepared by the Grupo de Investigación Equidad en Salud [Equity in Health Research Group], Faculty of Medicine, Universidad Nacional de Colombia.
Conflicts of interestThe authors have no conflicts of interest to declare.
MEDLINE strategy (February 2016)
Ovid MEDLINE(R) <1946 to June 18, 2016>
- 1.
exp audiovisual aids/ (96680)
- 2.
audiovisual aids.tw (137)
- 3.
(aid$ adj3 audiovisual$).tw(174)
- 4.
(audio-visual$ adj3 aid$).tw(115)
- 5.
(visual$ adj3 aid$).tw (1574)
- 6.
1 OR 2 OR 3 OR 4 OR 5 (97906)
- 7.
knowledge translation.tw,ti,ab(1065)
- 8.
Knowledge transference.tw (5)
- 9.
Knowledge transfer.tw (747)
- 10.
KT.tw,ti,ab(7079)
- 11.
knowledge utilization. tw(65)
- 12.
implementation research.tw(384)
- 13.
(exchang$ OR translat$ OR transfer$ OR diffus$ OR disseminat$ OR implement$ OR utili$).tw,ti,ab.(1738543)
- 14.
change.tw(711837)
- 15.
information.tw(756242)
- 16.
evaluation.tw(805730)
- 17.
implementation.tw (120492)
- 18.
utilization.tw(116330)
- 19.
utilisation.tw (9952)
- 20.
adoption.tw(26395)
- 21.
dissemination.tw (35089)
- 22.
OR 8 OR 9 OR 10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21. (3609030)
- 23.
randomized controlled trial. tw,ti,ab (36652)
- 24.
controlled clinical trial. tw,ti,ab(8916)
- 25.
clinical trial.tw (82191)
- 26.
random$.ti,ab. (715265)
- 27.
23 OR 24 OR 25 OR 26 (757742)
- 28.
6 AND 22 (21940)
- 29.
28 AND 27 (1684)
CENTRAL strategy (February 2016)
EBM Reviews – Cochrane Central Register of Controlled Trials – Ovid
- 1.
exp audiovisual aids/ (2812)
- 2.
audiovisual aids.tw (6)
- 3.
(aid$ adj3 audiovisual$).tw(12)
- 4.
(audio-visual$ adj3 aid$).tw(13)
- 5.
(visual$ adj3 aid$).tw (127)
- 6.
1 OR 2 OR 3 OR 4 OR 5 (2929)
- 7.
knowledge translation.tw,ti,ab(79)
- 8.
Knowledge transference.tw (0)
- 9.
Knowledge transfer.tw (46)
- 10.
KT.tw,ti,ab(727)
- 11.
knowledge utilization.tw(7)
- 12.
implementation research.tw (63)
- 13.
(exchang$ OR translat$ OR transfer$ OR diffus$ OR disseminat$ OR implement$ OR utili$).tw,ti,ab. (51031)
- 14.
change.tw (74456)
- 15.
information.tw (25310)
- 16.
evaluation.tw (62123)
- 17.
implementation.tw (6252)
- 18.
utilization.tw (4743)
- 19.
utilisation.tw (696)
- 20.
adoption.tw (1064)
- 21.
dissemination.tw (1270)
- 22.
OR 8 OR 9 OR 10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21. (188327)
- 23.
randomized controlled trial. tw,ti,ab (47657)
- 24.
controlled clinical trial. tw,ti,ab(11098)
- 25.
clinical trial.tw (56471)
- 26.
random$.ti,ab. (465225)
- 27.
23 OR 24 OR 25 OR 26 (476304)
- 28.
6 AND 22 (1188)
- 29.
AND 27 (895)
EMBASE strategy (February 2016)
Embase 1947 to 2016Feb26
- 1.
‘audiovisual aid’/exp OR ‘audiovisual aid’ (376)
- 2.
‘audiovisual aid’:ab,ti(11)
- 3.
(audio-visual NEAR/3 aid*):ab,ti(158)
- 4.
(audiovisual NEAR/3 aid*):ab,ti(230)
- 5.
‘audiovisual equipment’/exp (85103)
- 6.
‘audiovisual equipment’:ab,ti (22)
- 7.
1 OR 2 OR 3 OR 4 OR 5 OR 6 (85576)
- 8.
‘knowledge translation’:ti,ab(1822)
- 9.
‘Knowledge transference’:ti,ab (10)
- 10.
‘Knowledge transfer’:ti,ab (1252)
- 11.
‘KT’:ti,ab (9820)
- 12.
‘knowledge utilization’:ti,ab (83)
- 13.
‘implementation research’:ti,ab (577)
- 14.
(exchang* OR translat* OR transfer* OR diffuse* OR disseminat* OR implement* OR utili*) (2744763)
- 15.
‘change’:ab,ti(997523)
- 16.
‘information’:ab,ti (1088177)
- 17.
‘evaluation’:ab,ti (1206595)
- 18.
‘implementation’:ab,ti (186098)
- 19.
‘utilization’:ab,ti (168724)
- 20.
‘utilisation’:ab,ti (26131)
- 21.
‘adoption’:ab,ti (37893)
- 22.
OR 8 OR 9 OR 10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 (5380061)
- 23.
AND 22 (25470)
- 24.
23 AND (‘controlled clinical trial’/de OR ‘randomized controlled trial’/de OR ‘cluster randomised trial’) (740)
- 25.
24 AND [embase]/lim (531)
LILACS strategy (February 2016)
- 1.
(tw:(recursos audiovisuales)) OR (tw:(audiovisual aid)) AND (tw:(implementacion)) OR (tw:(Evaluacion)) (16)
PsycARTICLES strategy (March 2016)
- 1.
Interface – EBSCOhost Research Databases
- 2.
TX audiovisual aids OR TI audiovisual aids AND TX knowledge translation OR TI knowledge translation OR TI KT OR TX implementation OR knowledge utilization (13747)
- 3.
Methodology: treatment outcome/clinical trial (302)
WHO strategy (March 2016)
- 1.
International Clinical Trials Registry Platform ICTRP portal
- 2.
Audiovisual aids AND knowledge translation OR KT (486)
Bias risk summary: judgements of the authors of the review regarding each bias risk for each study included.
| 2014 | 2011 | 2007 | 2011 | 2011 | 2009 | 2009 | 2004 | 2011 | 2015 | 2013 | 2003 | 2011 | 2012 | 2004 | 1998 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ackerma | Adams | Albert | Arterbur | Bessette | Brendrye | Brayant | Bulter | Calderón | Choi | Collings | Cope | Cornoiu | Diefenbac | Di Noia | Dunn | |
| + | ? | + | + | + | + | ? | ? | + | ? | + | + | + | ? | ? | ? | *Sequence generation (selection bias) |
| ? | ? | + | ? | − | ? | ? | − | + | − | ? | − | ? | ? | ? | + | *Assignment hidden (selection bias) |
| − | ? | + | − | ? | ? | − | − | − | − | ? | − | − | − | ? | − | *Blinding of participants and staff (performance bias) |
| − | ? | − | − | − | ? | − | − | − | − | ? | − | − | − | ? | − | *Blinding of outcome assessors (detection bias) |
| + | ? | − | + | + | + | + | − | + | + | − | + | ? | − | ? | + | *Incomplete results data (attrition bias) |
| + | + | + | + | − | + | + | + | + | + | ? | + | + | + | + | + | *Selective reporting of results (reporting bias) |
| 2002 | 2007 | 2011 | 2005 | 2013 | 2009 | 2010 | 2013 | 2001 | 1998 | 2007 | 1988 | 2010 | 2011 | 2008 | 2003 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Eaden | Einsprun | Elander | Gattellart | Gerber | Glasgow | Gyomber | Haggbio | Harrison | Hoizheim | Hutchiso | Jenkinson | Kerunara | Klein | Koch | Krishna | |
| ? | ? | + | + | + | ? | + | + | ? | ? | + | ? | ? | ? | + | ? | *Sequence generation (selection bias) |
| ? | − | ? | + | ? | ? | ? | ? | ? | ? | − | ? | ? | − | ? | ? | *Assignment hidden (selection bias) |
| ? | + | ? | + | ? | − | ? | ? | − | − | − | − | − | − | − | + | *Blinding of participants and staff (performance bias) |
| ? | − | ? | + | ? | − | ? | + | − | − | − | − | − | − | − | ? | *Blinding of outcome assessors (detection bias) |
| + | − | − | + | + | + | + | − | ? | ? | + | − | + | − | ? | + | *Incomplete results data (attrition bias) |
| + | + | ? | + | ? | + | − | ? | + | − | ? | ? | + | + | + | + | *Selective reporting of results (reporting bias) |
| 2004 | 2006 | 2010 | 2011 | 2001 | 2009 | 1987 | 2013 | 2013 | 2003 | 2005 | 1995 | 2009 | 2011 | 2003 | 2009 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Leung | Linne | Lo | Lo | Meischke | Moore | Muirow | Mun | Neely | Nordfeldt | Nordfeldt | O’Donnell | Olver | Paradis | Proudfoot | Raynes − | |
| ? | + | ? | + | ? | + | ? | ? | ? | + | ? | ? | − | + | + | + | *Sequence generation (selection bias) |
| + | ? | ? | ? | ? | ? | ? | ? | + | − | − | ? | + | ? | ? | − | *Assignment hidden (selection bias) |
| − | − | ? | + | ? | − | ? | ? | + | + | + | − | ? | ? | ? | ? | *Blinding of participants and staff (performance bias) |
| − | − | ? | ? | ? | ? | ? | ? | − | − | − | − | − | + | ? | − | *Blinding of outcome assessors (detection bias) |
| + | + | − | − | − | − | − | − | − | + | + | + | + | + | − | + | *Incomplete results data (attrition bias) |
| + | ? | + | + | ? | + | − | ? | + | + | + | + | + | ? | − | ? | *Selective reporting of results (reporting bias) |
| 2004 | 2004 | 2009 | 1997 | 2001 | 2005 | 2013 | 2014 | 2015 | 2014 | 2012 | 1997 | 2009 | 2014 | 2014 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Redsell | Rossi | Rumnengo | Secher − | Shrier | Snyder − | Srai | Stice | Sullivan | Szmeja | Veroff | Weston | Wilheim | Windham | Wu | |
| ? | ? | ? | ? | ? | + | + | + | ? | + | ? | + | ? | ? | + | *Sequence generation (selection bias) |
| ? | − | − | ? | ? | ? | + | ? | ? | + | ? | − | ? | ? | ? | *Assignment hidden (selection bias) |
| ? | ? | − | − | ? | − | + | + | − | ? | ? | − | − | ? | ? | *Blinding of participants and staff (performance bias) |
| ? | − | − | − | ? | − | + | − | − | ? | ? | − | − | − | ? | *Blinding of outcome assessors (detection bias) |
| − | + | ? | + | − | + | + | + | ? | + | ? | ? | − | ? | ? | *Incomplete results data (attrition bias) |
| ? | + | + | − | − | + | + | + | ? | + | + | ? | + | − | + | *Selective reporting of results (reporting bias) |
+: low risk; −: high risk; ?: risk unclear.
The following are the supplementary data to this article:
Please cite this article as: Garzón-Orjuela N, Sánchez Bello NF, Bonilla Mahecha LP, Moreno Hernández LA, Suárez Ángel MC, Murcia Ardila NV, et al. Efectividad de las estrategias de transferencia de conocimiento en lenguaje audiovisual comparadas con otras para mejorar desenlaces en la salud individual y de la población general: revisión sistemática. Rev Colomb Psiquiat. 2019;48:105–126.
