



A cross-sectional study carried out in Cali households selected via probabilistic sampling, by two-stage clustering. Sociodemographic variables and their relationship with the knowledge, attitudes and practices of the caregivers were analysed.
ResultsA total of 519 caregivers were surveyed, most of whom were the mothers of the children. It was found that the predictors related to the knowledge and practices were: schooling, kinship, affiliation with the system, origin, number of children and people in the home, and no related variables were found in terms of attitudes.
ConclusionsIt was confirmed that sociodemographic variables predict the presence of knowledge and practices related to child maltreatment in caregivers. The predictors found are fundamental for identifying populations with higher risk of child abuse towards which priority promotion and prevention actions should be directed. The results of this study are essential for being able to incorporate strategies that promote appropriate child care, prevent child abuse into the community component of integral care of prevalent diseases of children (AIEPI), and modulate its effects through by promoting resilience in Colombia.
Estudio de corte transversal realizado en hogares de Cali seleccionados mediante muestreo probabilístico por conglomerados bietápico. Se analizaron variables sociodemográficas y su relación con los conocimientos, actitudes y prácticas de los cuidadores.
ResultadosSe encuestó a 519 cuidadores, en su mayoría madres de los niños. Se encontró que los predictores relacionados con los conocimientos y las prácticas son: escolaridad, parentesco, afiliación al sistema, procedencia, número de niños y personas que conforman el hogar, y en cuanto a las actitudes, no se encontraron variables relacionadas.
ConclusionesSe confirma que las variables sociodemográficas predicen la presencia de conocimientos y prácticas de los cuidadores relacionados con maltrato infantil. Los predictores encontrados son fundamentales para identificar las poblaciones con mayor riesgo de maltrato infantil, que son a las cuales deben dirigirse prioritariamente acciones de promoción y prevención. Los resultados de esta investigación son fundamentales para poder incorporar al componente comunitario de AIEPI estrategias que promuevan el cuidado infantil apropiado, prevengan el maltrato infantil y modulen sus efectos mediante la promoción de la resiliencia en Colombia.
Child abuse is a global public health issue.1,2 It is estimated that annually 70% of the paediatric population suffers some type of abuse.3 In Colombia, the estimated prevalence of child abuse is 42%,4 while in Cali, the reported figure is 30%.5
Child abuse is a social problem that generates multiple negative consequences in children. It causes cognitive deficit, speech problems, learning disorders, behaviour disorders, emotional problems, self-destructive behaviour, severe disability, neurological sequelae and even death.1,2
Sociodemographic, financial and family factors related to knowledge, attitudes and practices associated with child abuse have been identified. In particular, it has been determined that knowledge about this event is associated with a low education level, lack of financial resources that limit access to information tools, lack of support networks in the community, culture and forms of parenting.6 In turn, motivation that contributes to child abuse is the result of a history of violent behaviour, single-parent families and a history of domestic abuse.7 Furthermore, it has been found that inappropriate practices in the care of children are established when children suffer from a health condition that is difficult for parents or carers to cope with.8
In particular, in Colombia, there are regulations and initiatives aimed at promoting childcare and the prevention of child abuse.9,10 However, the prevalence of child abuse remains at a high level despite government efforts.4,5 Given that childcare is the responsibility of adults, the actions to promote appropriate care and prevent abuse requires tools to identify, and intervene as a matter of priority, in adults with a greater predisposition to providing inappropriate care.
In view of the above, the objective of this study was to identify sociodemographic variables that make it possible to predict levels of knowledge, attitudes and practices related to child abuse among those who provide care to children in communities with low socioeconomic strata, with the purpose of finding tools to identify populations at the greatest risk of child abuse in whom actions need to be focused to promote childcare and prevent child abuse contemplated in the community component of the strategy Atención Integral de Enfermedades Prevalentes de la Infancia [Comprehensive Care of Prevalent Childhood Illnesses] (AIEPI).11,12
Material and methodsA cross-sectional study was carried out to estimate the prevalence of knowledge, motivation and skills (KMS) related to child abuse in carers of children under the age of five in poor urban populations of Cali, Colombia.
Study populationMothers and carers of children under the age of five who lived in blocks with socioeconomic strata levels 1–3 from five municipalities of the urban area of the city of Cali were studied. The selection of municipalities was done from the map, demographic and socioeconomic information that the local administration made available to the public in accordance with the director of the AIEPI programme, of the Municipal Public Health Secretary of Cali.
Sample designThe sample design was aimed at estimating the prevalence of KMS following national and international recommendations.13–15 The area of interest of the study was mothers and carers of children under the age of five, living in municipalities 13, 14, 15, 16 and 21 of the Cali urban area. Due to the characteristics of the area of interest of the study, the design used, its cost-precision balance, it was probability two-stage cluster sampling. Probability sampling was used because the probability of selection of each block and each home was known and greater than zero, given that in each block selected the homes with children under the age of five were censored and listed, meaning that it was ensured that no home from the blocks selected was excluded from the selection. In this case, the blocks were considered as the clusters and the selection units were considered as the primary clusters and the homes as the secondary clusters. It was two-stage sampling given that first the blocks were selected and then, from a list of all the homes with children under the age of five identified in each block, the homes that would form part of the sample were selected systematically. The selection of homes relied on pre-designed tables that made it possible to reduce variability in the selection probability introduced by the variations in the number of homes per block.13,14
Sample sizeFrom the exploratory calculations for one-off estimates, using as parameters the study requirements, the resources available and the accuracy expected and a formula typical of simple random sampling of elements adapted to the design of clusters,13,14 to which a design effect (Deff) of 1.3 was incorporated in accordance with the national recommendations derived from urban studies in other Colombian cities,15,16 a minimum prevalence of KMS related to child abuse of 30%, similar to the prevalence of abuse estimated for Cali5, a relative standard error of 11%, which would make estimates possible, with an accuracy of 95%, between 23 and 37% and also expecting 20% of no response, it was estimated that it was necessary to select at least 360 carers of children under the age of five from the study population. Carers who were part of the community homes of the Instituto Colombiano de Bienestar Familiar [Colombian Institute of Family Well-being] were not included in this sample.
Study variablesTaking into account the Information, Motivation, Behavioural Skills (IMB) model17 and the parameters contemplated by the Ministry of Social Protection in the Baseline Survey included in the Guide for Local Facilitators of the Community AIEPI,11 the knowledge, motivation and skills related to child abuse were determined. In addition, sociodemographic variables such as education level, occupation, health system membership scheme, household composition, time living in the city and characteristics of the home.
Data collectionTo ensure the quality of the data, an instrument was designed for the collection of information based on the constructs of the IMB model11 and the guidelines for local facilitators of community AIEPI.18 Before applying it, this instrument was subjected to a cognitive interview which made it possible to adjust it to a more understandable speech for the population that was going to be interviewed, as well as to improve the sequence of questions. The form was applied face to face only to carers that agreed to participate freely and voluntarily in the study after explaining the procedures, benefits and risks that participation involved to them. The willingness to participate was expressed in a consent document that the carer signed. This study was endorsed and classified as a minimal risk study by the institutional ethics committee, taking into account the international guidelines for studies on human subjects and resolution 8430 of 1993 of the Ministry of Health of Colombia.19,20
The format was applied by interviewers with experience who were trained in the general aspects of the study and its operative procedures and who performed supervised application exercises. These interviewers were coordinated and accompanied by field supervisors with experience in the operation of population studies, group management, mapping and the application of procedures for the quality control of data. As the data collection advanced, a professional reviewed and evaluated the completed forms. This professional also verified the application of the interview by means of a telephone call to participants selected at random. Once reviewed and evaluated, they proceeded to store the formats in a database. The database records were contrasted with the completed formats in a random sample of 50% of the stored records.
AnalysisTaking the IMB model as a reference, variables which made it possible to examine and identify carers who presented inadequate knowledge, unfavourable motivation and inappropriate parenting skills which could contribute to the onset of child abuse were constructed. For each one of these variables, the prevalence was estimated with their respective 95% confidence intervals.
With the purpose of identifying predictors related to KMS with regard to child abuse, a count-type result variable was constructed. This variable quantified the number of KMS reported by the carers which are considered appropriate for the care of children according to international recommendations.2,4 Given the characteristics of this response variable, a negative binomial regression model was constructed. This type of model was considered the most appropriate because it sought to control the dispersion of the data, given that they presented differences between the variance and the mean of the result variable.21–23 Consequently, three models were constructed based on the negative binomial distribution: one for knowledge, another for motivation and a third for skills. In these models, the set of potentially predictive factors corresponded to sociodemographic variables.
To construct each model, after estimating the prevalences and evaluating the distribution, measures of central tendency and dispersion of each KMS, it was proceeded to carry out a bivariate negative binomial analysis. In this, the relationship was examined between sociodemographic characteristics and the variables of the sum of knowledge, motivation and skills. The relationship between continuous independent variables and each result variable was examined. If this relationship was of a non-linear type, it was proceeded to categorise the continuous variable. The categories were defined according to the ranges of values of the independent variable in which changes were observed in the direction and scale of the relationship with the count variable; these inflection points were the limits of the categories. With the nominal and categorical variables, contingency tables were constructed to estimate the coefficients of relationship (β) with the count variable. The results of this bivariate analysis made it possible to identify the sociodemographic variables which were related significantly to the KMS count. All the variables for which the coefficient of relationship had a significance p<0.25 in the bivariate analysis were included in the construction of the multiple model.
Then, by means of the elimination method of backward variables, variables were selected which were included in the final model, with a probability of withdrawal of 0.2. Among the variables selected, the presence of co-linearity was evaluated through the estimation of Spearman's correlation coefficient. If co-linearity was significantly high (around 30%), it was opted to exclude one of the variables from the final model to reduce its effect on variance, taking into account the theoretical model and the feasibility of intervention of these co-linear variables from the point of view of public health.
As a result of this analysis, sociodemographic variables were identified which were correlated with the appropriate number of KMS among the carers.
The analyses carried out were weighted by expansion factor in order to reduce possible biases in the estimations resulting from the variability in the final probability of selection of each participant.13,14,24
To carry out the diagnosis of the final model obtained, the presence of extreme values was examined through the calculation of residuals and graphic representation, variations of the coefficients >10% were verified and the plausibility of the data was evaluated in order to define its permanence or withdrawal from the model.
ResultsFrom the map databases, 80 blocks were selected, in which 3494 homes were registered in the census. It was identified that children under the age of five lived in 814 of these. Of these homes with children, 564 were selected, and in them 22 carers refused to participate, 10 were not at home after three visits on different days, and it was not possible to interview 12 for security reasons. Consequently, 519 surveys were completed; two of them were incomplete with no possibility of retrieving data, one survey was cancelled because it was applied to an underage carer and it was not possible to apply 44 surveys for security reasons. The rate of no response was 7.8%, but the planned sample size was exceeded.
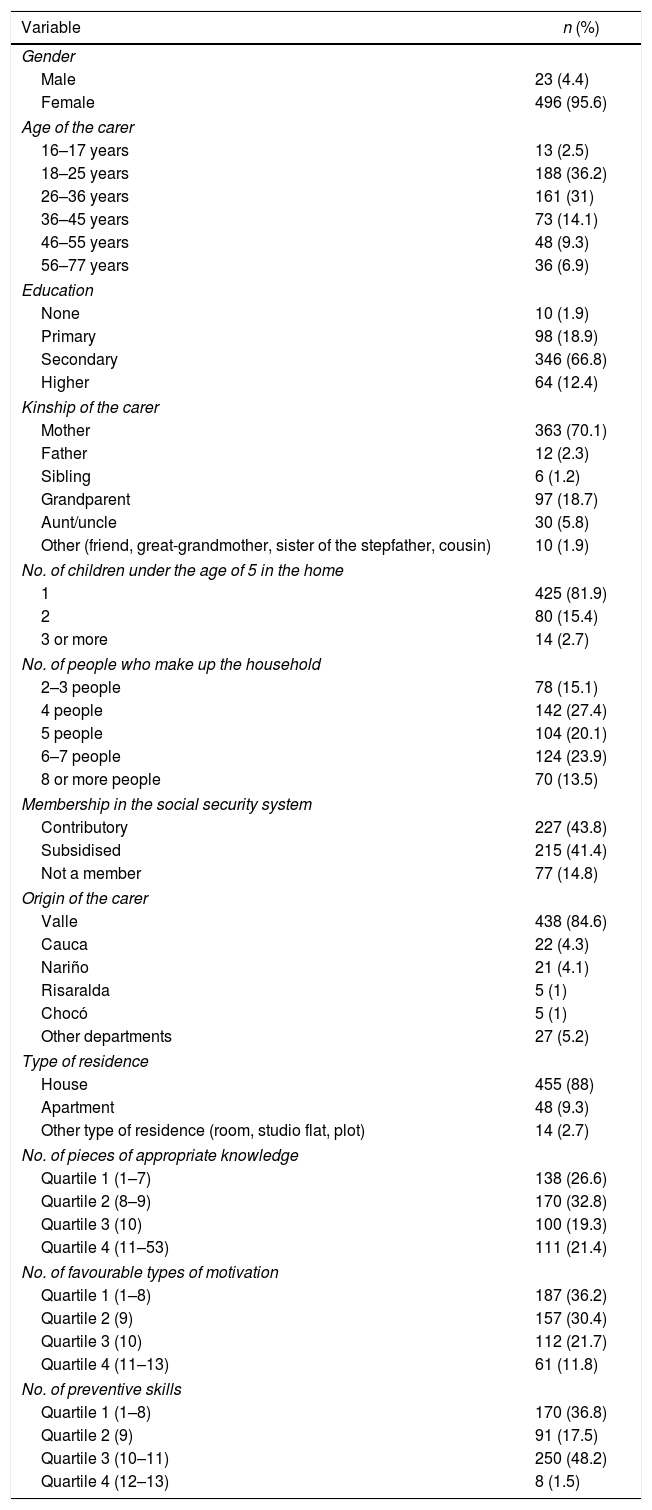
Most of the carers who participated in the study were the mothers of the children, aged between 18 and 45, most of them with secondary education; homes with only one child under the age of five predominated and most of the homes comprised of four to seven people. More than four out of five carers were members of the Colombian General Social Security System, but the State subsidises the membership of the health system for more than half, given their socioeconomic vulnerability. Almost all of them were from Valle and most of them live at home. Regarding the 53 pieces of knowledge investigated, almost 60% of the carers reported 9 or less appropriate pieces of knowledge; of the 13 favourable types of motivation and 13 preventive skills, 66.6 and 54.3% of the carers reported 9 or less (Table 1).
Sociodemographic characteristics of the participating carers.
| Variable | n (%) |
|---|---|
| Gender | |
| Male | 23 (4.4) |
| Female | 496 (95.6) |
| Age of the carer | |
| 16–17 years | 13 (2.5) |
| 18–25 years | 188 (36.2) |
| 26–36 years | 161 (31) |
| 36–45 years | 73 (14.1) |
| 46–55 years | 48 (9.3) |
| 56–77 years | 36 (6.9) |
| Education | |
| None | 10 (1.9) |
| Primary | 98 (18.9) |
| Secondary | 346 (66.8) |
| Higher | 64 (12.4) |
| Kinship of the carer | |
| Mother | 363 (70.1) |
| Father | 12 (2.3) |
| Sibling | 6 (1.2) |
| Grandparent | 97 (18.7) |
| Aunt/uncle | 30 (5.8) |
| Other (friend, great-grandmother, sister of the stepfather, cousin) | 10 (1.9) |
| No. of children under the age of 5 in the home | |
| 1 | 425 (81.9) |
| 2 | 80 (15.4) |
| 3 or more | 14 (2.7) |
| No. of people who make up the household | |
| 2–3 people | 78 (15.1) |
| 4 people | 142 (27.4) |
| 5 people | 104 (20.1) |
| 6–7 people | 124 (23.9) |
| 8 or more people | 70 (13.5) |
| Membership in the social security system | |
| Contributory | 227 (43.8) |
| Subsidised | 215 (41.4) |
| Not a member | 77 (14.8) |
| Origin of the carer | |
| Valle | 438 (84.6) |
| Cauca | 22 (4.3) |
| Nariño | 21 (4.1) |
| Risaralda | 5 (1) |
| Chocó | 5 (1) |
| Other departments | 27 (5.2) |
| Type of residence | |
| House | 455 (88) |
| Apartment | 48 (9.3) |
| Other type of residence (room, studio flat, plot) | 14 (2.7) |
| No. of pieces of appropriate knowledge | |
| Quartile 1 (1–7) | 138 (26.6) |
| Quartile 2 (8–9) | 170 (32.8) |
| Quartile 3 (10) | 100 (19.3) |
| Quartile 4 (11–53) | 111 (21.4) |
| No. of favourable types of motivation | |
| Quartile 1 (1–8) | 187 (36.2) |
| Quartile 2 (9) | 157 (30.4) |
| Quartile 3 (10) | 112 (21.7) |
| Quartile 4 (11–13) | 61 (11.8) |
| No. of preventive skills | |
| Quartile 1 (1–8) | 170 (36.8) |
| Quartile 2 (9) | 91 (17.5) |
| Quartile 3 (10–11) | 250 (48.2) |
| Quartile 4 (12–13) | 8 (1.5) |
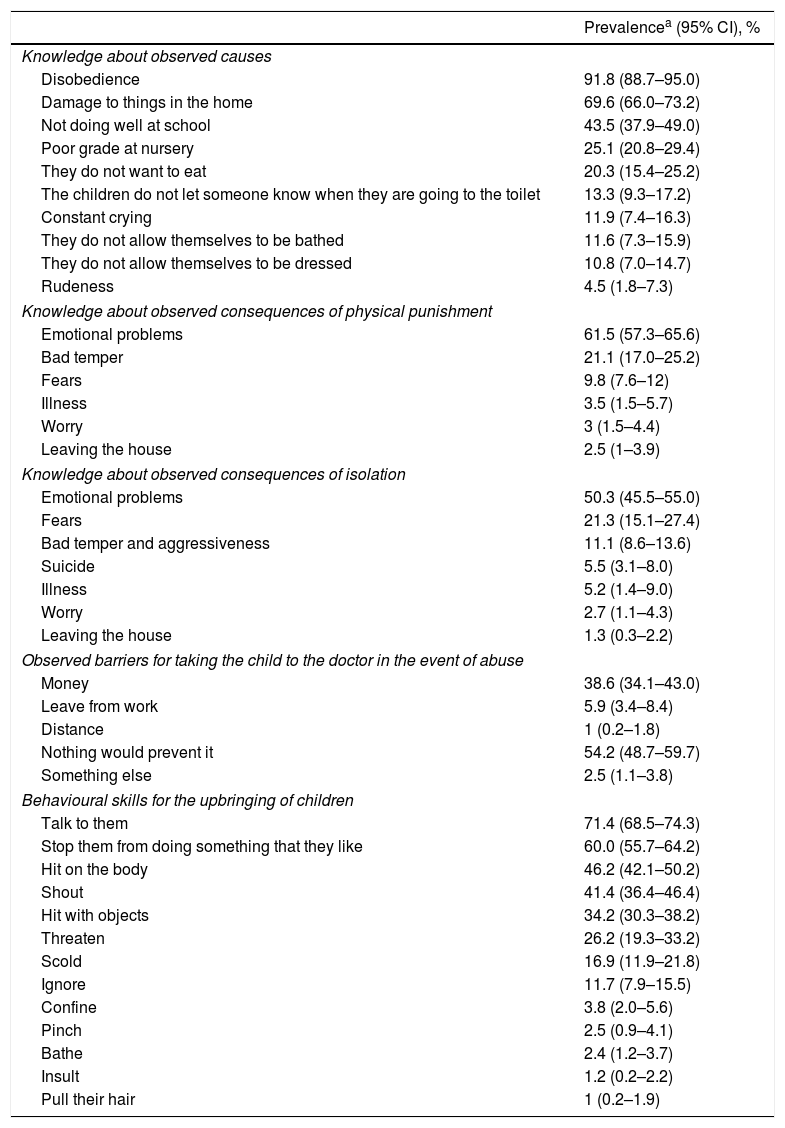
In particular, high prevalences were observed of inappropriate knowledge that leads to the punishment of children, low levels of knowledge on the consequences of physical punishment and of isolation, and a little more than half ensures that nothing would stop them from taking the child to the doctor in the case of abuse. In skills, it was observed that more than two thirds use dialogue to modulate the child's behaviour, but a high percentage also resort to physical and emotional punishment simultaneously. Regarding motivation, it was reported that almost all of the carers consider it necessary to explain to the child what they did wrong. Despite this, types of motivation were demonstrated which contribute to child abuse such as considering that as they are the parents or carers of the children they have the right to physically punish their children, that in the face of bad behaviour of their children it is necessary to tell them off or punish them physically and that punishment is good for their education (Table 2).
Prevalence of knowledge, motivation and skills related to child abuse in carers of children under the age of 5 in Cali, Colombia.
| Prevalencea (95% CI), % | |
|---|---|
| Knowledge about observed causes | |
| Disobedience | 91.8 (88.7–95.0) |
| Damage to things in the home | 69.6 (66.0–73.2) |
| Not doing well at school | 43.5 (37.9–49.0) |
| Poor grade at nursery | 25.1 (20.8–29.4) |
| They do not want to eat | 20.3 (15.4–25.2) |
| The children do not let someone know when they are going to the toilet | 13.3 (9.3–17.2) |
| Constant crying | 11.9 (7.4–16.3) |
| They do not allow themselves to be bathed | 11.6 (7.3–15.9) |
| They do not allow themselves to be dressed | 10.8 (7.0–14.7) |
| Rudeness | 4.5 (1.8–7.3) |
| Knowledge about observed consequences of physical punishment | |
| Emotional problems | 61.5 (57.3–65.6) |
| Bad temper | 21.1 (17.0–25.2) |
| Fears | 9.8 (7.6–12) |
| Illness | 3.5 (1.5–5.7) |
| Worry | 3 (1.5–4.4) |
| Leaving the house | 2.5 (1–3.9) |
| Knowledge about observed consequences of isolation | |
| Emotional problems | 50.3 (45.5–55.0) |
| Fears | 21.3 (15.1–27.4) |
| Bad temper and aggressiveness | 11.1 (8.6–13.6) |
| Suicide | 5.5 (3.1–8.0) |
| Illness | 5.2 (1.4–9.0) |
| Worry | 2.7 (1.1–4.3) |
| Leaving the house | 1.3 (0.3–2.2) |
| Observed barriers for taking the child to the doctor in the event of abuse | |
| Money | 38.6 (34.1–43.0) |
| Leave from work | 5.9 (3.4–8.4) |
| Distance | 1 (0.2–1.8) |
| Nothing would prevent it | 54.2 (48.7–59.7) |
| Something else | 2.5 (1.1–3.8) |
| Behavioural skills for the upbringing of children | |
| Talk to them | 71.4 (68.5–74.3) |
| Stop them from doing something that they like | 60.0 (55.7–64.2) |
| Hit on the body | 46.2 (42.1–50.2) |
| Shout | 41.4 (36.4–46.4) |
| Hit with objects | 34.2 (30.3–38.2) |
| Threaten | 26.2 (19.3–33.2) |
| Scold | 16.9 (11.9–21.8) |
| Ignore | 11.7 (7.9–15.5) |
| Confine | 3.8 (2.0–5.6) |
| Pinch | 2.5 (0.9–4.1) |
| Bathe | 2.4 (1.2–3.7) |
| Insult | 1.2 (0.2–2.2) |
| Pull their hair | 1 (0.2–1.9) |
95% CI: 95% confidence interval.
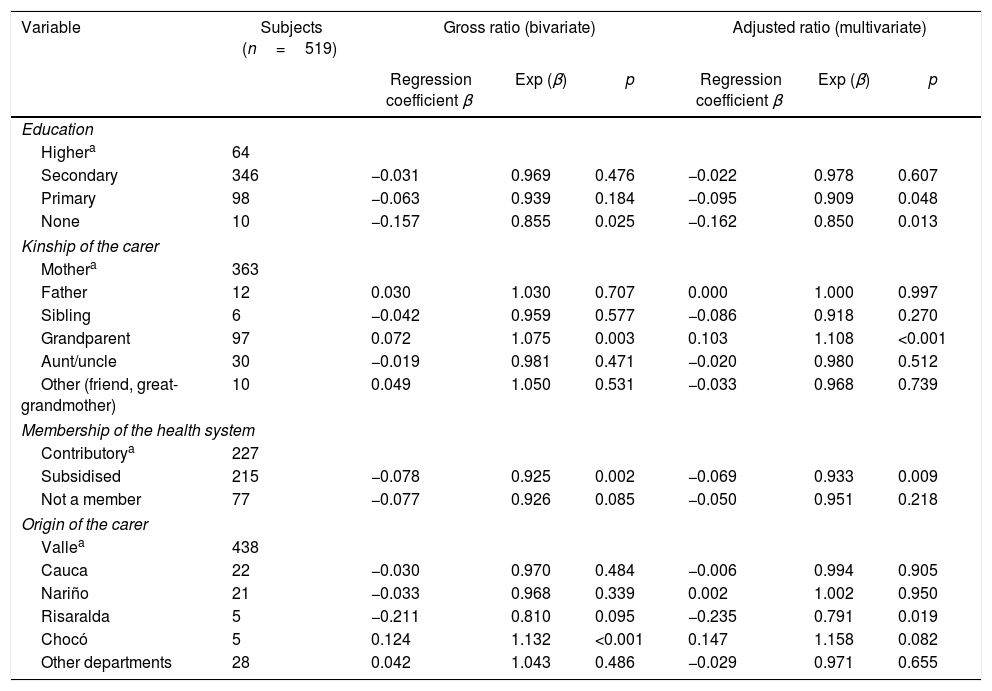
The number of appropriate pieces of knowledge of the carers reduced the lower the education level. This trend towards the reduction in the number of appropriate pieces of knowledge for the care of the child was accentuated significantly when the carers with higher education were compared with the carers without education, who had 14% less knowledge than those with higher education.
Carers who were members of the health system by means of the subsidised scheme had 7% less appropriate knowledge than carers who were members of the contributory scheme. It was also found that by comparing mothers as carers with grandparents as carers, the latter had 8% more appropriate knowledge than mothers who look after their children and when the carer came from the department of Chocó, they had 13% more appropriate knowledge than the carer from Valle (Table 3, gross ratio).
Relationship between sociodemographic variables and number of appropriate pieces of knowledge for the care of children under the age of 5 in Cali, Colombia.
| Variable | Subjects (n=519) | Gross ratio (bivariate) | Adjusted ratio (multivariate) | ||||
|---|---|---|---|---|---|---|---|
| Regression coefficient β | Exp (β) | p | Regression coefficient β | Exp (β) | p | ||
| Education | |||||||
| Highera | 64 | ||||||
| Secondary | 346 | −0.031 | 0.969 | 0.476 | −0.022 | 0.978 | 0.607 |
| Primary | 98 | −0.063 | 0.939 | 0.184 | −0.095 | 0.909 | 0.048 |
| None | 10 | −0.157 | 0.855 | 0.025 | −0.162 | 0.850 | 0.013 |
| Kinship of the carer | |||||||
| Mothera | 363 | ||||||
| Father | 12 | 0.030 | 1.030 | 0.707 | 0.000 | 1.000 | 0.997 |
| Sibling | 6 | −0.042 | 0.959 | 0.577 | −0.086 | 0.918 | 0.270 |
| Grandparent | 97 | 0.072 | 1.075 | 0.003 | 0.103 | 1.108 | <0.001 |
| Aunt/uncle | 30 | −0.019 | 0.981 | 0.471 | −0.020 | 0.980 | 0.512 |
| Other (friend, great-grandmother) | 10 | 0.049 | 1.050 | 0.531 | −0.033 | 0.968 | 0.739 |
| Membership of the health system | |||||||
| Contributorya | 227 | ||||||
| Subsidised | 215 | −0.078 | 0.925 | 0.002 | −0.069 | 0.933 | 0.009 |
| Not a member | 77 | −0.077 | 0.926 | 0.085 | −0.050 | 0.951 | 0.218 |
| Origin of the carer | |||||||
| Vallea | 438 | ||||||
| Cauca | 22 | −0.030 | 0.970 | 0.484 | −0.006 | 0.994 | 0.905 |
| Nariño | 21 | −0.033 | 0.968 | 0.339 | 0.002 | 1.002 | 0.950 |
| Risaralda | 5 | −0.211 | 0.810 | 0.095 | −0.235 | 0.791 | 0.019 |
| Chocó | 5 | 0.124 | 1.132 | <0.001 | 0.147 | 1.158 | 0.082 |
| Other departments | 28 | 0.042 | 1.043 | 0.486 | −0.029 | 0.971 | 0.655 |
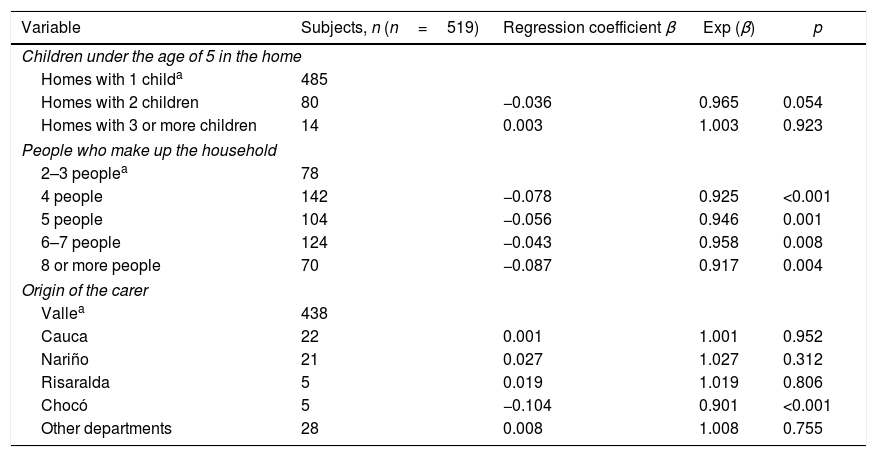
With regard to the types of motivation related to the appropriate care of children, it was observed that homes made up of more than four people tend to have less motivation for appropriate care than homes made up of two or three people. By comparing carers from Valle with those from Chocó, it was observed that they had 10% less motivation for the appropriate care of children than those from Valle. It was also found that by comparing homes with one child and homes with two children, they had 3% less motivation for the appropriate care of children than homes with only one child under five, but this difference is not statistically significant (Table 4, gross ratio).
Gross ratio (bivariate) between sociodemographic variables and the number of types of motivation for the adequate care of children under the age of 5 in Cali, Colombia.
| Variable | Subjects, n (n=519) | Regression coefficient β | Exp (β) | p |
|---|---|---|---|---|
| Children under the age of 5 in the home | ||||
| Homes with 1 childa | 485 | |||
| Homes with 2 children | 80 | −0.036 | 0.965 | 0.054 |
| Homes with 3 or more children | 14 | 0.003 | 1.003 | 0.923 |
| People who make up the household | ||||
| 2–3 peoplea | 78 | |||
| 4 people | 142 | −0.078 | 0.925 | <0.001 |
| 5 people | 104 | −0.056 | 0.946 | 0.001 |
| 6–7 people | 124 | −0.043 | 0.958 | 0.008 |
| 8 or more people | 70 | −0.087 | 0.917 | 0.004 |
| Origin of the carer | ||||
| Vallea | 438 | |||
| Cauca | 22 | 0.001 | 1.001 | 0.952 |
| Nariño | 21 | 0.027 | 1.027 | 0.312 |
| Risaralda | 5 | 0.019 | 1.019 | 0.806 |
| Chocó | 5 | −0.104 | 0.901 | <0.001 |
| Other departments | 28 | 0.008 | 1.008 | 0.755 |
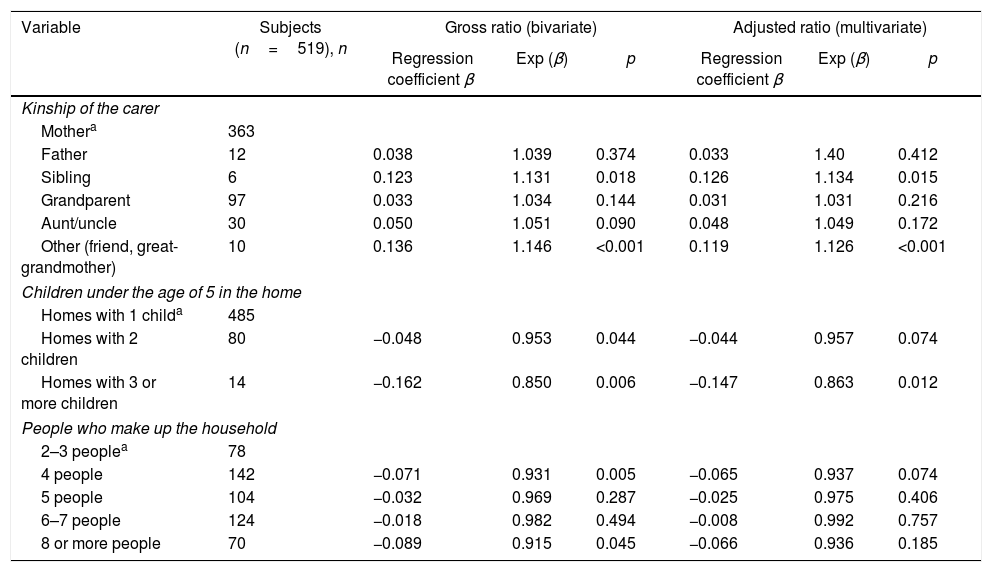
Regarding the appropriate skills for the adequate care of children, when the carer was a sibling, a friend or the great-grandmother, they had more skills for adequate care than when the carer was the mother. In contrast, when there were two or more children under the age of five in the homes, the skills for adequate care were 5–15% lower than in homes with only one child under the age of five. When the home was made up of four or more people, the number of skills for the adequate care of the child under the age of five could be reduced by up to 8% compared to those made up of two or three people. However, the differences found with homes made up of four to seven people did not reach statistical significance. This significance was only reached with homes made up of eight or more people (Table 5, gross ratio).
Relationship between sociodemographic variables and the number of appropriate skills for the care of children under the age of 5 in Cali, Colombia.
| Variable | Subjects (n=519), n | Gross ratio (bivariate) | Adjusted ratio (multivariate) | ||||
|---|---|---|---|---|---|---|---|
| Regression coefficient β | Exp (β) | p | Regression coefficient β | Exp (β) | p | ||
| Kinship of the carer | |||||||
| Mothera | 363 | ||||||
| Father | 12 | 0.038 | 1.039 | 0.374 | 0.033 | 1.40 | 0.412 |
| Sibling | 6 | 0.123 | 1.131 | 0.018 | 0.126 | 1.134 | 0.015 |
| Grandparent | 97 | 0.033 | 1.034 | 0.144 | 0.031 | 1.031 | 0.216 |
| Aunt/uncle | 30 | 0.050 | 1.051 | 0.090 | 0.048 | 1.049 | 0.172 |
| Other (friend, great-grandmother) | 10 | 0.136 | 1.146 | <0.001 | 0.119 | 1.126 | <0.001 |
| Children under the age of 5 in the home | |||||||
| Homes with 1 childa | 485 | ||||||
| Homes with 2 children | 80 | −0.048 | 0.953 | 0.044 | −0.044 | 0.957 | 0.074 |
| Homes with 3 or more children | 14 | −0.162 | 0.850 | 0.006 | −0.147 | 0.863 | 0.012 |
| People who make up the household | |||||||
| 2–3 peoplea | 78 | ||||||
| 4 people | 142 | −0.071 | 0.931 | 0.005 | −0.065 | 0.937 | 0.074 |
| 5 people | 104 | −0.032 | 0.969 | 0.287 | −0.025 | 0.975 | 0.406 |
| 6–7 people | 124 | −0.018 | 0.982 | 0.494 | −0.008 | 0.992 | 0.757 |
| 8 or more people | 70 | −0.089 | 0.915 | 0.045 | −0.066 | 0.936 | 0.185 |
The multiple negative binomial analysis confirmed the relationship of the level of education, kinship (grandparents) and the membership scheme (subsidiary) with the number of pieces of knowledge related to adequate care of the child under the age of five observed in the bivariate analysis. In terms of the origin of the carer, it was observed in the multiple analysis that the relationship with the carer who came from Chocó became not significant and became significant when the carer came from Risaralda. With this adjustment, it was revealed that carers from Risaralda have 21% less knowledge than those from Valle (Table 3, adjusted ratio).
Regarding motivation, the multiple binomial regression analysis showed that none of the variables that had shown a relationship with the motivation for the adequate care of children under the age of five confirmed their relationship.
With regard to the skills for the adequate care of children under the age of five, in the multiple negative binomial analysis it was observed that the relationship is maintained when the homes have three or more children under the age of five, but not when there are two children under the age of five in the home. In addition, the relationship between skills and homes with eight or more people also loses its significance (Table 5, adjusted ratio).
In general, the extent of the changes observed in the relationships of variables in the multiple analysis with respect to the bivariate analysis do not reveal the presence of confusion or interactions between variables. This indicates that the sociodemographic variables that were finally correlated with the number of appropriate KMS for the care of children under the age of five have an independent relationship with each other.
DiscussionIn this investigation, a high prevalence of KMS was found in carers of children under the age of five which could contribute to child abuse. In particular, it was revealed that carers justify abuse if the children are disobedient. This coincides with what was found in a study conducted in Cuba, where behaviour of the children which triggered lack of self-control in adults was reported.2
In this study, it was also found that poor school performance is considered by the carers to be one of the causes that justifies punishing children. There was a similar finding in a Mexican population, where physical and verbal abuse were resorted to in the face of unfavourable academic results.25
Low prevalences were also found regarding knowledge of carers against consequences generated by abuse. Nevertheless, it is worth highlighting that around half of carers participating in the study identified emotional consequences in children, which, although with less physical evidence, have greater connotations in the development of the individual.4 Similarly, in a study conducted in Colombia, it was identified that abused children can develop depression and low self-esteem.26
With regard to the motivation of carers regarding child abuse, a high percentage of carers who think that it is necessary to initiate timely dialogue about errors made in order to correct children was found, which leads to reflection as an educational tool. This finding is consistent with a qualitative study performed in Costa Rica, in which it was explained that the best way to solve a conflicting situation between parents and children is to speak about the issue.27 However, it should be noted that approximately all carers reported using dialogue as a means to correct children. The majority of them (80%) also assume that punishment is necessary to educate children and that, as they have the role of parents, they have the right to punish them physically and emotionally. This finding is similar to that reported by UNICEF, in which it was specified that 50% of adults think that using abuse against children is a valid form of education and punishment.4 The co-existence of dialogue and punishment in carers in Cali may indicate a socially desirable response against dialogue.
It was revealed that the mother of children under the age of five is the person who exercises punishment within the home (61.4%). This prevalence is similar to that reported in a cross-sectional study carried out in Mexico City, in which it was estimated that almost 60% of mothers demonstrated abusive behaviour in the upbringing of their children.28 This seems to occur because the mother is the person who spends most of the time caring for children and, in addition, as is referred to in worldwide studies, culturally it is considered that the mother is responsible for enforcing the rules and is the figure of authority in most homes.29,30 In this study, it was also made apparent that physical and verbal abuse is the most prevalent in society.4,31 Almost 50% of carers indicated that they use blows to the body and shouting as a means to correct and educate. These findings are consistent with those found in Chile, where similar prevalences were reported.31
Potentially predictive factors corresponding to sociodemographic variables related to the KMS of carers with regard to child abuse in children under the age of five were identified. Among them, it was found that the education of the carer, kinship, social security system membership, origin and composition of the household were statistically significant. Therefore, carers with postgraduate studies show that they have more elements to understand child abuse, the causes and consequences, as worldwide investigations have reported.2,32
In this investigation, it was also found that grandparents have greater prevalences of adequate knowledge on the care of children under the age of five, and are an important figure in their upbringing.33 In our society, it is common for parents to work during the day and entrust the grandparents to look after the children.34
Another predictor related to knowledge about child abuse is membership in the social security system in health. It was observed that carers belonging to the contributory scheme have greater knowledge about the prevention of this event. According to Colombian studies, this is due to the situation of fragility which people under a subsidised scheme experience, who present educational and economic shortcomings, which increase the likelihood of suffering from violence within their homes.35 In addition, this population has less access to health services, communication methods and educational programmes delivered by specialist professionals who ask people to understand child abuse as a multidimensional problem.36
In this study, it was also found that the origin of the carers is a decisive predictor in knowledge about child abuse. In particular, it was observed that carers from the Eje Cafetero [Coffee Axis] report low levels of knowledge on how to prevent child abuse compared to carers from the Pacific area of Colombia. This finding coincides with the report issued by the Instituto Colombiano de Bienestar Familiar in 2013 and with worldwide studies which emphasise that living conditions and social, political and cultural contexts influence the upbringing of children and people who are related to their care, and at the same time determine to some measure the likelihood of using punishment as a means of education for children.4,12,37,38
In this study, it was identified that the variable number of children under the age of five in the home has a relationship with the practices of carers in terms of child abuse. In particular, it was found that in homes where three or more children live there is a greater likelihood of having skills that contribute to child abuse. This finding is similar to that found in studies performed in Cuba and in Spain, in which it is considered that in extended families the relationships are more unstable, more conflicting and a common source of tension for the upbringing of children.28,29
The relationships found between KMS and sociodemographic variables are an advance towards the identification of child abuse predictors in populations with socioeconomic disadvantages. The identification of these predictors would enable the paediatric populations at greatest risk of abuse to be identified and to focus the promotion and prevention of child abuse interventions on them. Therefore, there would be a greater opportunity to act before the abuse causes physical, mental and emotional alterations in children.39,40
The results of this investigation highlight the importance of identifying and intervening in the carer and families at risk of abusing. They should be provided with the necessary tools through educational strategies in topics related to the development of children in each of the stages of the life cycle, healthy co-existence and in the acquisition of skills for the education of children. Despite the fact that this strategy has few studies in which its efficacy in the reduction of cases of child abuse is verified, direct and indirect results have been revealed in the strengthening of parents’ role.41–43
In recent years, it has been observed that the effects of child abuse on the development and adaptation of children is not homogenous, i.e. there are children who despite having suffered abuse manage to establish appropriate adaptive behaviour and reach cognitive, emotional and behavioural development which is very similar to that of non-abused children. Therefore, the recent investigation focused not only on identifying factors that contribute to child abuse, but also on identifying the conditions that facilitate resilience. The findings of investigations focused on resilience are now being incorporated into public health policies and programmes aimed at promoting appropriate childcare and the prevention of child abuse and its effects.44
The scope of this descriptive study makes it possible to establish that there is a large deficit in KMS in carers of children under the age of five in Cali, which reveals that children from areas of the city with socioeconomic disadvantages are at high risk of being abused by their carers, and the magnitude of the risk demands that the approach to this event be a matter of priority in public health policies and programmes. However, the relationships that were found in this study are still preliminary explanations that should be subjected to verification with studies with greater inferential capacity45,46 which, in combination with qualitative methods, may provide greater opportunities for understanding the problem, as this is an essential component for the design and implementation of interventions that promote the appropriate care of children under the age of five and the prevention of child abuse.44 Consequently, theoretical frameworks which provide greater explanatory opportunities should be accepted instead of an exploratory framework like that used in this cross-sectional study.47 This is fundamental so that strategies which promote appropriate childcare, prevent child abuse and modulate its effects by means of the promotion of resilience in Colombia can be incorporated into the community component of AIEPI.
Conflicts of interestThe authors have no conflicts of interest to declare.
This investigation was carried out thanks to the support of the Universidad del Valle using the advisory services of Dr. Sandra Lorena Girón, who participated as director of the research work from which this article was derived in the period from January 2014 to April 2016.
Please cite this article as: Zúñiga Bolívar SM, Holguín Ruiz JA, Mateus Solarte JC. Correlación entre conocimientos, motivaciones y habilidades relacionadas con cuidado infantil y aspectos sociodemográficos en Cali, Colombia. Rev Colomb Psiquiatr. 2019;48:156–165.
