







To determine the healthy life years (HLY) lost as a result of mental disorders and nervous system diseases in Medellin from 2006 to 2012.
MethodsDescriptive study using a secondary information source according to the Global Burden of Disease (GBD) framework. To calculate the years of potential life lost (YPLL), we used vital statistics data; to calculate disability-adjusted life years (DALY), we used morbidity data from individual records managed by health service providers, outpatient clinics and other research studies. HLY are the sum of YPLL and DALY.
ResultsIn Medellin, from 2006 to 2012, out of 1,242,407 HLY related to mental disorders and nervous system diseases, the vast majority (99.39%) were due to disability. Most HLY were found in females (70.22%) and 81% were found in people aged 15–59. The disorders representing the greatest burden were unipolar depressive disorder (81%), Alzheimer’s disease and other types of dementia (4.82%), schizophrenia (3.5%) and drug use disorders (2.78%).
ConclusionsOur results indicate a significant increase in the disease burden due to mental disorders and nervous system diseases. Public policy decision-makers in the city of Medellin should take note, as health problems of this type can result in a substantial rise in healthcare costs.
Determinar la pérdida de años de vida saludables (AVISA) por trastornos mentales y enfermedades del sistema nervioso en Medellín, de 2006 a 2012.
MétodosEstudio descriptivo, con fuente de información secundaria bajo lineamientos teóricos del Estudio la Carga Global de la Enfermedad (CGE). Para calcular los Años Potenciales de Vida Perdidos (APVP), se empleó información de las estadísticas vitales; para los Años de Vida Ajustados por Discapacidad (AVD), la de morbilidad de los Registros Individuales de Prestación de Servicios de Salud (RIPS), de consulta externa y otras investigaciones. Los AVISA se obtuvieron de sumar los APVP y AVD.
ResultadosEn Medellín, durante el septenio, de 1.242.407 AVISA por trastornos mentales y enfermedades del sistema nervioso, la mayor carga se debió a discapacidad (99,39%). Las mujeres aportaron más AVISA (70,22%). El 81% de los AVISA se concentraron en el grupo de 15 a 59 años. Los trastornos que mayor carga representaron fueron, en este orden, el trastorno depresivo unipolar (81%), el Alzheimer y otras demencias (4,82%), la esquizofrenia (3,45%) y los trastornos por consumo de drogas (2,78%).
ConclusionesSe sustenta un importante incremento de la carga de la enfermedad por trastornos mentales y enfermedades del sistema nervioso, lo que debe llamar la atención de los tomadores de decisiones sobre la política pública del municipio, ya que estos problemas de salud pueden significar un gran aumento en los costos de atención en salud.
The number of people with a disability is increasing around the world due to multiple causes. Some are due, largely, to the ageing of the population and the increase of chronic diseases generating disability, such as cardiovascular diseases, diabetes and mental disorders.1 Since the 1960s, a change started to be observed in the profiles of morbidity and mortality, and infectious diseases in developing countries, which until then had been those which most concern was shown for. They started to be replaced by non-communicable diseases, in particular long-term conditions and those which progress slowly.2
Mental health is a particularly big challenge and a priority within the field of modern public health as, despite the fact that mental disorders and diseases of the nervous system do not cause a large number of direct deaths, they represent a significant total burden of disease which is difficult to prevent, attend to and rehabilitate.3,4 Therefore, it is necessary to integrate mental health into all aspects of health and social policy, not only due to the magnitude and costs that neuropsychiatric conditions represent, but also due to their individual, family and social impact, which translates into a suffering which goes beyond the figures and disability that it causes.2
Despite the fact that mental health is as important as physical health for the well-being of individuals, social transformations and the increase in longevity have been the focus of attention for many governmental bodies in many countries.4 At the start of this century, almost 450 million people were suffering from neuropsychiatric conditions; currently, more than 25% of the population suffers from at least one mental or behavioural disorder throughout life.5
The International Statistical Classification of Diseases and Related Health Problems (ICD-10) defines mental disorders as a group in which symptoms vary substantially and are characterised in general by any combination of abnormalities in thought processes, emotions, behaviour and relationships with others. These include unipolar depressive disorder, bipolar disorder, and disorders due to use of alcohol and certain psychoactive substances, Alzheimer's disease and other dementias, post-traumatic stress disorder, obsessive compulsive disorder and panic disorder and primary insomnia.5
People who suffer from mental disorders have very high rates of disability and mortality, and those who suffer from major depression or schizophrenia have a 40–60% higher probability of premature death than the general population.6 It is calculated that mental and behavioural disorders represent 12% of the total burden of disease; among the top 10 causes of disability in the world, four are mental disorders.5 These have a financial impact on societies and on the quality of life of individuals and their families, as approximately one in every four families has at least one member affected by a mental or behavioural disorder.7
In order to deal with the growing health burden that the current epidemiological profile represents with a high prevalence of mental disorders, it is necessary to understand and to constantly monitor their behaviour not only in terms of morbidity and mortality, but in a way which makes it possible to quantify the chronicity of disorders and the disability that they cause, as they are events that lead more often to a disability than the premature death of the patient.5 For this, the World Bank (WB) and the World Health Organization (WHO) have promoted studies on burden of disease in terms of epidemiological indicators which facilitate obtaining population information on the magnitude of diseases, integrating mortality and morbidity in terms of years of potential life lost (YPLL) due to premature mortality and healthy life years (HLY) lost.3,8,9
The approach to tackle the burden of disease due to mental disorders and nervous system diseases is due to Murray and López,10,11 a method which seeks to evaluate trends and to establish general health priorities through the YPLL and disability-adjusted life years (DALYs), which together represent the HLY lost; the latter also makes it possible to measure the gap between the current status and the ideal situation in which all individuals live until old age without suffering from illnesses or disability.4,8,9
The burden represented by mental illnesses is becoming increasingly more significant throughout the world; in 1990, mental disorders caused 10% of the total HLY lost due to illnesses and lesions. In 2000, this burden had increased by 2% and it is expected that by 2020 it will reach up to 15%. Among the most common, and for the most part causing considerable disabilities, are depressive disorders (which impose a burden 50% higher in women than in men and affect more than 350 million people worldwide), those due to the use of psychoactive substances and alcohol (which are among the top 10 causes of disability in low-, medium- or high-income countries), schizophrenia (affects around 21 million people all over the world), epilepsy and Alzheimer's disease.5 Estimates from the WHO in 2005 show that neuropsychiatric disorders also contribute to mortality, as they cause 1.2 million deaths every year and 1.4% of all the HLY lost (largely due to dementia, Parkinson's disease and epilepsy).4
In Latin America and the Caribbean, 21,361,776 life years are lost as a result of neuropsychiatric disorders which account for 22% of the total burden of disease and have a significant impact in terms of mortality, morbidity and disability in all stages of life. In 1990, psychiatric and neurological conditions explained 8.8% of the HLY lost. In 2002, this burden had risen to 22.2%, a similar figure to the burden of disease in developed countries. Among adults with the greatest risk (15–59 years), the disorders which affect the greatest number of people are major depression, dysthymia, generalised anxiety disorder and alcohol abuse or dependence. Depressive disorder (the main cause among women and fourth among men) and alcohol abuse or dependence (the second cause after violence in men) each affect approximately 38 million adults at some point in their lives.4
Mental health studies in Colombia reflect important psychopathology data. Data from the Mental Health Study in 2003 indicate that 40.1% of the Colombian population have had a mental disorder at some point in their life.12
Mental disorders in Colombia particularly affect children, adolescents and young adults, a situation which worsens the prognosis, academic and economic productivity of the population to a great extent and, ultimately, the total capital, which includes personal, symbolic, cultural and relational factors. According to the Encuesta Nacional de Salud Mental de Colombia (National Mental Health Survey of Colombia) in 2015, the prevalence of mental disorders in children was 4.7%, higher in girls (5.6%) than in boys (3.8%); in adolescents it was 4.4% and in adults it was observed that one in every 25 people have one of the mental disorders assessed in the past 12 months and nine in every 100 have suffered from them throughout their life. In this age group, the most prevalent mental disorders were major depressive disorder and social phobia, and the affective and anxiety disorders studied were more common in adult women and people aged 18–44.13
According to the study on the burden of disease in Colombia in 2005, the country lost 280 HLY/1000 people, 74% due to disability. Neuropsychiatric problems such as unipolar major depression (47 total HLY), bipolar disorders (5 total HLY), schizophrenia (3 HLY) and epilepsy (2 total HLY) cause 21% of the burden of HLY lost per thousand people in Colombia.14 In 2010, Colombia had a total of 269 HLY/1000 people, 211 corresponding to DALYs; among men, unipolar major depression was the second cause with more HLY lost 37 and, in women, it was the condition with the greatest impact 68 HLY lost.15
In the particular case of the city of Medellín, an analysis of the burden of disease through the calculation of its relevant indicators, YPLL and DALYs, has not been carried out since 1995, when 513,847 HLY were lost, 56.6% due to premature mortality, and more than half (56% were due to lesions; neuropsychiatric diseases represented a loss of 8226 HLY, of which 78.8% were due to disability (DALY), with which it was located in twelfth position in the burden of disease of Medellín of 1996.16
Mental disorders are a priority problem for public health, as they start at an early age, have a high comorbidity and cause serious disability, which means a burden for the families, the community and governmental bodies. This therefore presents the magnitude of the loss of HLY due to mental disorders and nervous system diseases by the population of Medellín in the period 2006–2012.
MethodsIt is a descriptive study, registered in the analytical empirical approach, with secondary sources of information, the target population of which are inhabitants of the municipality of Medellín between 2006 and 2012. The aspects defined in the Global Burden of Disease (GBD)9,17,18 study were taken into account for its methodological approach. In order to comply with the objective proposed, the following disorders assessed on a national scale were selected due to their impact and their representativeness in this subgroup of causes14,15: unipolar depressive disorder, bipolar disorder, schizophrenia, epilepsy, alcohol use and drug use disorders, Alzheimer's disease and other dementias, Parkinson's disease, multiple sclerosis, post-traumatic stress disorder, obsessive compulsive disorder, panic disorder, insomnia (primary) and migraine, coded according to the ICD-10.
As sources of information, the population census of Medellín for age and gender was used for each study year; for the calculation of the YPLL, the mortality database supplied by Medellín's Department of Health, which was adjusted for the under-reporting of mortality was used, in accordance with the Pan American Health Organization (PAHO) method of proportional distribution19,20 and the Preston-Coale method21; for DALYs, as the quantification of the severity of non-fatal events was required, the incidence of each event was taken into account and, for that, the Registros Individuales de la Prestación de Servicios [Individual Service Provision Records] (RIPS) on an Outpatient Basis, were taken initially as a source of information. The distribution of the incidence obtained from there was adjusted through the functions of the software DisMod II according to the distribution of other indicators such as mortality and prevalence. For the prevalence data, those reported in the ENSM 2003 and the first mental health population study for Medellín 2011–2012 were taken into account, given that they were the population surveys that were available on the date that the calculations were made; experts in each area validated the distributions obtained.
Experts in the area, most with training in epidemiology, validated the incidences and prevalences concerning mental disorders and nervous system diseases of which there were no reports in previous studies. The DALYs were calculated from the incidences obtained with the software DISMOD II using exponential smoothing and after the experts validated those of the events whose magnitude in previous studies was unknown or when the source of information was not the official source, a special case or they were the RIPS. The mortality rates were calculated to carry out the descriptive analysis of the study and, just like the incidences and prevalences of events with little information, they were presented to the experts in order to reaffirm the coherence and validity of these results.
The work with the experts was carried out by face-to-face meetings (one or two) in which the estimates of the indicators were presented and their validity was obtained in accordance with their knowledge and experience in the area.
For the estimation of the YPLL, the standard methodology11 which considers life expectancy at birth for different ages, derived from a standard life table (Coale and Demeny West model) similar to that of Japan,21 a weighting function of the years lived at ages for which the deceased person would have lived and a discount rate of future years of life lost equivalent to 3%. For the calculation of the DALYs, it was necessary to obtain an approximation of the incidences of each one of the events considered, which were assessed from the RIPS on an outpatient basis according to medical and epidemiological criteria, after they were adjusted using the software DisMod II, while also considering the prevalences found in the population studies and the estimated rates of mortality. These adjusted calculations were validated with experts. In addition to the above, the following were taken into account as basic parameters for their estimation: average duration and age of onset of the disease broken down by gender and age groups; the burden of disability generated by each cause; the weighting function of the time lived at different age; and a discount rate of 3%.
To conclude, the estimate of the HLY lost was obtained by adding up the YPLL and the DALYs for each one of the breakdowns considered (group and subgroup of diseases and/or lesions, and specific causes by year, gender and age groups).
ResultsBetween 2006 and 2012, Medellín lost 7.5 million HLY, which accounts for a rate of 463.12 HLY/1,000 inhabitants. In the seven-year period, and in each one of the years, non-communicable diseases were the cause of the highest number of HLY lost (91.8%); a marked difference was perceived in the contribution of each component (disability and mortality) when it was analysed in general and by group of causes. While in general less than a quarter of the HLY lost were explained by premature deaths (13.0%), it was observed that the lesions explained almost 98% of the HLY lost. Furthermore, 87.0% of the HLY lost were due to DALYs, and, of these, non-communicable diseases were also the cause of a high percentage (93.6%). In the study period, it stands out that the subgroups of causes made up of cardiovascular diseases, mental disorders and nervous system diseases cause 75.1% of HLY lost; this latter subgroup of causes was the second biggest (16.5%).
Mental disorders and nervous system diseasesYears of life lost due to premature deathIn general, during the seven-year period in Medellín, 7625 life years were lost due to premature death because of the mental disorders and nervous system diseases under consideration, with an average of 1089 YPLL/year and a rate of 0.47 YPLL/1000 inhabitants; the years 2007, 2008 and 2009 are those which contribute to almost 53% of the YPLL in the period (Fig. 1). During the seven study years, men suffered greater premature loss of life than women (56.6 and 43.4% of YPLL, respectively), a pattern that coincides every study year, except for 2008 and 2010, in which women suffered a greater loss (52.4 and 54.4%. Both men and women had a variable loss throughout the period, with a slight tendency to reduce from 2009 in men 0.79 YPLL/1000 men is the highest figure of the period and from 2008 in women 0.62 YPLL/1000 women Fig. 1).

Furthermore, it was observed that both the total number of YPLL and the rate of YPLL in each age group were higher among men, in contrast to children under the age of four and adults over the age of 80, groups in which the contribution of the female gender was higher. A positive gradient was observed from the age of 30, i.e. as the age increased, the rates of YPLL due to mental disorders and nervous system diseases in both genders increased (Fig. 2). A total of 56.3% of the YPLL was focussed on the 15–59 years age group, with a greater predominance in the 15–29 years age group 1628 YPLL, 21.34%) followed by the 45–59 years age group 1425 YPLL; 18.69%).

In the study period, the greatest loss of life years due to premature death caused by mental disorders and nervous system diseases in the city of Medellín was due mostly to epilepsy 5214 YPLL; 68.37%; 0.32 YPLL/1000 inhabitants, followed by Alzheimer's disease and other dementias 1,588 YPLL; 20.83%; 0.10 YPLL/1000 inhabitants) and Parkinson's disease (388 YPLL; 5.09%; 0.02 YPLL/1000 inhabitants); these three causes represented 94.29% of the YPLL in general. The highest number of YPLL due to epilepsy was focused in males (62.09%), while those caused by Alzheimer's disease and other dementias, Parkinson's disease and multiple sclerosis were representative in women (57.22, 53.97 and 5.45%, respectively).
Specifically by age group, among those under the age of four, the highest number of YPLL due to mental disorders and nervous system diseases were due to epilepsy (840 YPLL, of which women had 60.56%); among children aged 5–14 and young people aged 15–29, this same condition was the cause of 91.5% (0.17 YPLL/1,000 under the age of 5–14) and 91.19% 0.37 YPLL/1000 young people of the YPLL, respectively. Epilepsy and Alzheimer's disease and other dementias were involved in the greatest burden due to mortality presented among adults under the age of 69, and among individuals over the age of 70, Alzheimer's disease and other dementias and Parkinson's disease had a leading role.
Disability-adjusted life yearsIn Medellín, a burden of disability due to mental disorders and nervous system diseases of 1,234,781 years (76.12 DALYs/1,000 inhabitants) was presented in 2006–2012, with an annual average of 176,397 DALYs. It was observed that, in the seven-year period and in each one of the years, women 101.27 DALYs/1000 women had a higher loss of DALYs for this subgroup of causes than men 29.61%; 47.87 DALYs/1000 men. In general, by the year 2012 244,623 DALYs the DALYs increased by approximately 95% with regard to the initial study year (125,258 DALYs); both men and women had a stable loss, with a marked tendency to increase from 2009 (Fig. 3).

A total of 81.11% of the DALYs by the subgroup of causes assessed was focused in the group aged 15–59; young people aged 15–29 and adults aged 30–44 are those who presented the highest loss of DALYs (31.03%, 95.31 DALYs/1000 inhabitants and 29.97%; 107.72 DALYs/1000 inhabitants. Likewise, it was observed that both the total number of DALYs and the rate of DALYs were higher in women over the age of 15. Among men, a negative gradient was presented from the age of 15, and in women from the age of 30.
Between 2006 and 2012, 95.81% of the burden of disability caused by mental disorders and nervous system diseases was due mainly to unipolar depressive disorder (1,001,450 DALYs; 61.74 DALYs/1000 inhabitants), Alzheimer's disease and other dementias (58,264 DALYs; 3.59 DALYs/1000 inhabitants), schizophrenia (42,818 DALYs; 2.64 DALYs/1,000 inhabitants), drug use disorders (34,468 DALYs; 2.12 DALYs/1000 inhabitants), epilepsy (23,223 DALYs; 1.43 DALYs/1000 inhabitants) and migraine (22,810 DALYs; 1.41 DALYs/1000 inhabitants), in this order (Fig. 4).

In both men and women, unipolar depressive disorder had a significant contribution to DALYs lost (72.84 and 84.58%, respectively), followed by schizophrenia (5.97%), Alzheimer's disease and other dementias (5.76%) and drug use disorders (5.26%) in men, and due to Alzheimer's disease and other dementias (4.28%), schizophrenia (2.42%) and migraine (2.38%) in women.
By age group, it was observed that among those under the age of four, 97.71% of the DALYs due to mental disorders and nervous system diseases were caused by unipolar depressive disorder 3181 DALYs; 88.53%; 3.11 DALYs/1,000 children under the age of 4) and epilepsy (0.32 DALYs/1,000 children under the age of 4); among children aged 5–14, 94.24% of the DALYs were due to unipolar depressive disorder (82,750 DALYs; 85.76%; 36.45 DALYs/1000 children aged 5–14, bipolar disorder 4415 DALYs; 1.94 DALYs/1000 and epilepsy 1.66 DALYs/1000; among young people aged 15–29, there was a greater share of unipolar depressive disorder (314,069 DALYs; 81.96%; 78.12 DALYs/1,000 young people aged 15–29), drug use disorders (4.98%; 4.74 DALYs/1000, schizophrenia 4.84%; 4.61 DALYs/1000 and migraine 2.75%; 2.62 DALYs/1000; among adults aged 30–44, 93.35% of the DALYs lost were unipolar depressive disorder (323,042 DALYs; 87.29%, 94.03 DALYs/1,000 adults aged 30–44), schizophrenia (3.49%; 3.76 DALYs/1000 and drug use disorders 2.56%; 2.76 DALYs/1000; unipolar depressive disorder and Alzheimer's disease and other dementias caused approximately 86% of the DALYs of people between the ages of 45 and 79; and among those over the age of 80, Alzheimer's disease and other dementias were the cause of the highest percentage of DALYs (12,935 DALYs; 67.80%; 46.80 DALYs/1000 adults over the age of 80, followed by unipolar depressive disorder 22.3%; 15.40 DALYs/1000 and Parkinson's disease 7.01%; 4.84 DALYs/1000.
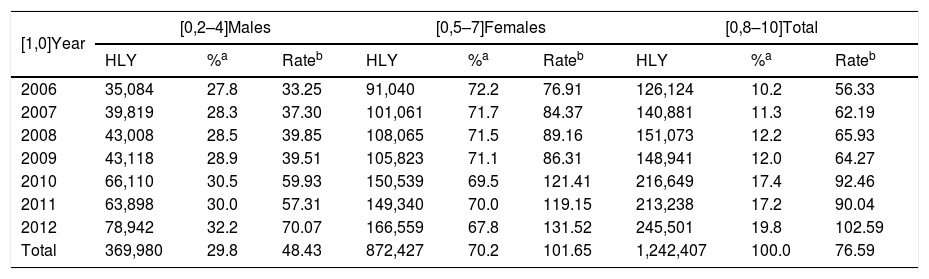
Healthy life years lostFrom 2006–2012, Medellín lost 1,242,407 HLY in total due to mental disorders and nervous system diseases, which involves a rate of 76.59 HLY/1000 inhabitants and an average of 177,487 HLY/year. The significant increase 95%) in absolute numbers of HLY lost in the population of Medellín between 2006 (126,124 HLY) and 2012 (245,501), accompanied also by an 82% increase in the rate of 56.33 HLY/1000 inhabitants in 2006 to 102.59 in 2012 is striking. In general, and in particular by year, women had a leading role in the contribution of HLYs lost by subgroup of causes assessed 70.2%) (Table 1).
Distribution of the total, percentage and rate of HLY lost due to mental disorders and nervous system diseases by year and gender. Medellín, 2006–2012.
| [1,0]Year | [0,2–4]Males | [0,5–7]Females | [0,8–10]Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HLY | %a | Rateb | HLY | %a | Rateb | HLY | %a | Rateb | |
| 2006 | 35,084 | 27.8 | 33.25 | 91,040 | 72.2 | 76.91 | 126,124 | 10.2 | 56.33 |
| 2007 | 39,819 | 28.3 | 37.30 | 101,061 | 71.7 | 84.37 | 140,881 | 11.3 | 62.19 |
| 2008 | 43,008 | 28.5 | 39.85 | 108,065 | 71.5 | 89.16 | 151,073 | 12.2 | 65.93 |
| 2009 | 43,118 | 28.9 | 39.51 | 105,823 | 71.1 | 86.31 | 148,941 | 12.0 | 64.27 |
| 2010 | 66,110 | 30.5 | 59.93 | 150,539 | 69.5 | 121.41 | 216,649 | 17.4 | 92.46 |
| 2011 | 63,898 | 30.0 | 57.31 | 149,340 | 70.0 | 119.15 | 213,238 | 17.2 | 90.04 |
| 2012 | 78,942 | 32.2 | 70.07 | 166,559 | 67.8 | 131.52 | 245,501 | 19.8 | 102.59 |
| Total | 369,980 | 29.8 | 48.43 | 872,427 | 70.2 | 101.65 | 1,242,407 | 100.0 | 76.59 |
HLY: healthy life years.
The highest proportion of HLY lost was concentrated in the group aged 15–59 (81% of the HLY), but the highest peak was presented among adults aged 30–44 (108.08 HLY/1000 inhabitants), behaviour followed by women (31.8%; 149.83 HLY/1000 women; among men, young people aged 15–29 had the greatest loss of healthy life (34.8%; 64.30 HLY/1000 men.
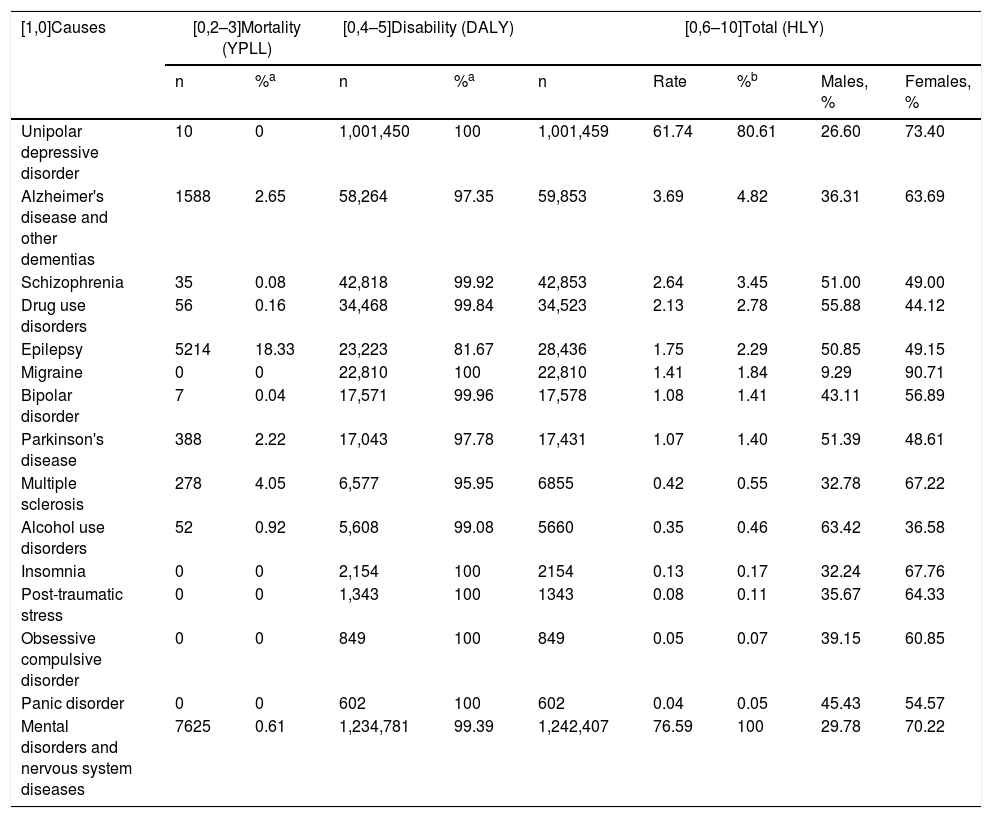
An important difference was observed in the contribution of each component (mortality and disability), as the largest part (99.39%) of HLY lost by Medellín as a result of mental disorders and nervous system disease was due to disability, a pattern followed in each one of the years contemplated and cause of specific disease (Table 2).
Healthy life years lost due to mortality and due to disability as a result of mental disorder/illness. Medellín, 2006–2012.
| [1,0]Causes | [0,2–3]Mortality (YPLL) | [0,4–5]Disability (DALY) | [0,6–10]Total (HLY) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | %a | n | %a | n | Rate | %b | Males, % | Females, % | |
| Unipolar depressive disorder | 10 | 0 | 1,001,450 | 100 | 1,001,459 | 61.74 | 80.61 | 26.60 | 73.40 |
| Alzheimer's disease and other dementias | 1588 | 2.65 | 58,264 | 97.35 | 59,853 | 3.69 | 4.82 | 36.31 | 63.69 |
| Schizophrenia | 35 | 0.08 | 42,818 | 99.92 | 42,853 | 2.64 | 3.45 | 51.00 | 49.00 |
| Drug use disorders | 56 | 0.16 | 34,468 | 99.84 | 34,523 | 2.13 | 2.78 | 55.88 | 44.12 |
| Epilepsy | 5214 | 18.33 | 23,223 | 81.67 | 28,436 | 1.75 | 2.29 | 50.85 | 49.15 |
| Migraine | 0 | 0 | 22,810 | 100 | 22,810 | 1.41 | 1.84 | 9.29 | 90.71 |
| Bipolar disorder | 7 | 0.04 | 17,571 | 99.96 | 17,578 | 1.08 | 1.41 | 43.11 | 56.89 |
| Parkinson's disease | 388 | 2.22 | 17,043 | 97.78 | 17,431 | 1.07 | 1.40 | 51.39 | 48.61 |
| Multiple sclerosis | 278 | 4.05 | 6,577 | 95.95 | 6855 | 0.42 | 0.55 | 32.78 | 67.22 |
| Alcohol use disorders | 52 | 0.92 | 5,608 | 99.08 | 5660 | 0.35 | 0.46 | 63.42 | 36.58 |
| Insomnia | 0 | 0 | 2,154 | 100 | 2154 | 0.13 | 0.17 | 32.24 | 67.76 |
| Post-traumatic stress | 0 | 0 | 1,343 | 100 | 1343 | 0.08 | 0.11 | 35.67 | 64.33 |
| Obsessive compulsive disorder | 0 | 0 | 849 | 100 | 849 | 0.05 | 0.07 | 39.15 | 60.85 |
| Panic disorder | 0 | 0 | 602 | 100 | 602 | 0.04 | 0.05 | 45.43 | 54.57 |
| Mental disorders and nervous system diseases | 7625 | 0.61 | 1,234,781 | 99.39 | 1,242,407 | 76.59 | 100 | 29.78 | 70.22 |
DALY: disability-adjusted life years; HLY: healthy life years; YPLL: years of potential life lost.
Observe the importance that unipolar depressive disorder had on the burden of disease in Medellín between 2006 and 2012, which represented approximately 81% of the total of HLY lost due to mental disorders and nervous system diseases, with a rate close to 62 HLY/1000 inhabitants, affecting mainly women 73.40%; Alzheimer's disease and other dementias 3.69 HLY/1000 inhabitants were in second place, with a greater loss in women 63.69%), and schizophrenia (2.64 HLY/1000 inhabitants) and drug use disorders (2.13 HLY/1000 inhabitants), both causes more predominant in men (Table 2).
Men had a greater loss of HLY in the period in question due to alcohol use disorders (63.42%), drug use disorders (55.88%), Parkinson's disease (51.39%), schizophrenia (51%) and epilepsy (50.85%); in the rest of the disorders considered in this study, the share of women was significant (Table 2).
Children under the age of four presented a greater loss of HLY due to unipolar depressive disorder and epilepsy (97% due to both causes); 94% of the HLY lost by individuals under the age of 14 was due to unipolar depressive disorder (85%), bipolar disorder (5%) and epilepsy (4%); among young people aged 15–29, the greatest burden of disease was due to unipolar depressive disorder (82%), drug use disorders (5%) and schizophrenia (4.8%); among adults aged 30–44, unipolar depressive disorder, schizophrenia and drug use disorders represented 93% of the HLY lost; 90.7% of the HLY lost by adults aged 45–59 was due to unipolar depressive disorder (83.6%), Alzheimer's disease and other dementias (4.2%) and schizophrenia (2.9%); those aged 60–69 suffered loss of HLY mainly due to unipolar depressive disorder (66%), Alzheimer's disease and other dementias (18%) and Parkinson's disease (8%); loss of HLYs among individuals aged 70–79 was due to Alzheimer's disease and other dementias (43%), unipolar depressive disorder (41%) and Parkinson's disease (10%); to conclude, in the group over the age of 80, behaviour was similar to that of the previous age group, but in different proportions (68, 22 and 7%, respectively).
DiscussionIn Medellín, during the seven-year period considered, the results revealed that, of the 1,242,407 HLY lost, the greatest burden of disease due to mental disorders and nervous system diseases was due largely (99.39%) to the disability that they cause, behaviour followed equally by each one of the causes included; women (70.22%) were those that lost most HLY contributed by the subgroup of causes assessed. In general, 81% of the HLY lost was concentrated in the group aged 15–59; in women, the highest peak was observed in the group aged 30–44 149.83 HLY/1000 women, and in men it was greater among young people aged 15–29 64.30 HLY/1000 men.
During the study period, an increase of HLY lost was found year on year. Of the 1,242,407 HLY lost due to mental disorders and nervous system diseases, 99.39% correspond to disability. This behaviour can be understood from the epidemiological and demographic transition, given that it is not only interesting to explain the changes in mortality, but also in morbidity. In the case of mental or nervous system disorders, they go from being an acute process which frequently ends in death to a chronic state in which many people, mainly elderly, suffer for long periods of life with progressive disability.
Between 2006 and 2012, unipolar depressive disorder had a leading role in the burden of disease in Medellín due to mental disorders and nervous system diseases, as it represented 81% of the total HLY lost, followed by Alzheimer's disease and other dementias (4.82%), schizophrenia (3.45%) and drug use disorders (2.78%); it was also observed that women presented a greater proportion of HLY lost than men in nine of the 14 cases evaluated, with a more pivotal role in the HLY lost due to migraine, unipolar depressive disorder, insomnia and multiple sclerosis; and a greater participation of HLY lost by men than by women was observed in alcohol use disorders, drug use disorders, Parkinson's disease and schizophrenia.
The excess of disability contributed by mental disorders and nervous system diseases is related, in part, to the fact that they occur at increasingly earlier ages than other chronic diseases5; it is also known that around 450 million people in the world suffer from mental disorders, with similar prevalence in men and women; however, they have greater probability of suffering from mood disorders or anxiety disorders (especially depression) and those of suffering disorders related to the control of impulses and substance abuse,22 a situation which it has been possible to observe in Medellín from 2006 to 2012 through the HLY lost due to these mental disorders.
In line with the international and national data on the burden represented by mental disorders, in the results of this study, mental disorders and nervous system diseases that accounted for the greatest loss of HLY are unipolar depressive disorder, Alzheimer's disease and other dementias, schizophrenia and drug use disorders. According to the study on total burden of disease, unipolar depression is one of the three main causes of the burden of disease in the regions of America, Europe and the Western Pacific, and across the world represents 4.3% of the total of HLY lost, ranking third, and it is expected that by 2030 this condition will be the cause with the highest proportion of HLY lost worldwide, with a representation of 6.2%.23
Similarly, in Latin America and the Caribbean, unipolar depressive disorders represent 6.9% of all the HLY lost, and alcohol use disorders also cause a significant proportion (3.9%).4 According to the study on the burden of disease in Colombia from 2005,14 neuropsychiatric problems such as unipolar major depression, bipolar disorders, schizophrenia and epilepsy caused 21% of the total burden of HLY lost. In Medellín, during 2006–2012, these same causes led to 14% of all the HLY lost.
In particular, it is known that depressive disorders are characterised by a combination of sadness, lack of interest for activities and reduced energy, and they are more common in women than in men3; a condition that was observed in this study, where women presented a greater proportion of HLY lost due to unipolar depressive disorder (73.4%) than men. Although depression may occur at any time of life, cases of depression are increasingly being identified in adolescents and young adults, as was perceived in this study, given that unipolar depressive disorder was representative in the first three mental disorders considered and, on average, 83% of the HLY lost by adolescents and young adults of the population of Medellín was due to this type of depressive disorder.
Schizophrenia, which is a serious condition that can affect educational and job performance and generally starts in adolescence or the first years of adult life, ranks third among mental disorders and nervous system diseases taken into account in this study, with a loss of 42,853 HLY (3.45%), with a slightly higher proportion of men (51%), which may be related to the fact that this condition in women tends to start later in life and have a more favourable progression and prognosis (WHO).3,8
These results again support the gradual and constant development of the population dynamics towards ageing which, along with the worsening of social problems and social agitation, make it possible to predict an increase in the number of individuals affected by non-communicable diseases, particularly mental disorders and nervous system diseases.3,6 In Colombia, and particularly in Medellín, violence, displacement and unemployment have a significant impact on the mental health of the population, which is why this health component should take priority in the city's social, economic and health agenda, as children and young people are the most affected, followed by women and elderly people.4
According to the Pan American Health Organization, the care of chronic non-communicable diseases is a global problem, which should increasingly attract the attention of decision makers in relation to the public policy of the regions, given that these health problems, such as mental disorders, may mean a considerable increase in the costs of health care. It has been demonstrated that these patients do not receive the necessary care, as around half are diagnosed and half of these are treated.8,15 Furthermore, the WHO reports show that the psychiatric burden of disease in the world is underestimated; of the 10 main causes of disability in the world, measured in HLY lost, 50% are psychiatric conditions.13
Finally, this study has also made it possible to identify the lack of epidemiological information of several conditions as, at the time of obtaining the incidences and prevalences of the conditions and/or disorders considered, it was perceived that most of these events do not have pertinent, representative and/or up-to-date national or local sources of information, which made it largely difficult to calculate the DALYs, the incidence of which was a fundamental indicator.
Similarly, it should be considered that the results described here may be underestimated, as from the same source of information used for the calculation of incidences, the individual records of the provision of services on an outpatient basis (RIPS), as indicated, only take into account the people who access health services; therefore, in general terms, the lack of knowledge of the real health situation of a population has been converted into a limitation of decision-making in terms of the prioritisation and distribution of resources.7 These limitations bring with them implications, given that the information on mortality is not linked to morbidity or, in other words, there is no information system, of a data warehouse type, which enables a joint assessment of its consistency and a holistic management of the data and enables the minimisation of errors, especially of the information on morbidity, related to mental disorders and nervous system diseases. The fact that there is insufficient information and good quality data, combined with the absence of analytical epidemiological studies which have calculated the incidences, prevalences and fatality associated with mental disorders and nervous system diseases, is a factor which calls into question the robustness of the estimates of the indicators of the burden of disease for the above-mentioned events. Studies in the city which take account of the assessment of interventions in mental disorders and nervous system diseases, in particular, in mental health or in general, are not known either which is an obstacle to carrying out an evaluation of the efficacy of policies and a cost-benefit analysis.
Given the objective and study characteristics, it was not pertinent to identify risk factors associated with mental disorders and nervous system diseases in the population of Medellín and, therefore, its specific burden, which analytical studies keep an eye on in the sense that they enable the knowledge of exposure, associated comorbidities and the calculation of population attributable risks.
Considering that mental health refers to well-being, the prevention of mental disorders and the treatment and rehabilitation of people affected by these disorders and that the WHO studies show that these continue to be one of the health problems which have the greatest impact on the quality of life of people and economic costs for the individual, society and health systems,24 with a significant impact on the life expectancy of people who suffer from them, as it is 20 years shorter than that of those who do not have them,25 in addition to the fact their onset is related to factors such as poverty, unemployment and lack of social relations,26 and that, added to this, there is a health social security system which has not operated adequately, where mental health care is limited. This research reveals the magnitude of one of the health problems which requires the greatest cross-sectional effort in the city, where it is necessary to implement mental health policies that not only take care of mental disorders but create actions which promote settings and life conditions that enable people to adopt and maintain healthy lifestyles, from a governmental and non-governmental level, in that the health sector has the participation of the education, work, justice, transport, environment, housing or social care sectors, as indicated by the WHO.
Similarly, the decisions, policies and programmes which take place regarding the situation observed in the research should serve to prepare people so that they enjoy healthy ageing, with the offer of different opportunities which increase the independence and self-esteem of the population.
Furthermore, this type of research enables policies and health programmes which are promoted in the area to be based on scientific evidence on the health needs of the population; therefore, for the scientific community, developing these types of studies and applying new knowledge to health development needs makes it possible to strengthen their communication and cooperation with political leaders in charge of local and regional decision-making.
This exercise reveals the major problem of how mental disorders and nervous system diseases require priority care in the city's public agenda.
FundingMedellín's Department of Health funded the conduct of the original project from which this study is derived.
Conflicts of interestThe authors have no conflicts of interest to declare.
To Medellín's Department of Health and the members of the Research Group on Demographics and Health of the Universidad de Antioquia (University of Antioquia).
Please cite this article as: Grisales-Romero H, González D, Porras S. Años de vida saludable perdidos a causa de trastornos mentales y enfermedades del sistema nervioso de la población de Medellín, 2006–2012. Rev Colomb Psiquiat. 2020;49:29–38.
