


Complaints of patients undergoing invasive percutaneous procedures are a frequent finding. Our objective was to assess the discomfort of patients undergoing cardiac catheterization using femoral or radial approach.
MethodsCross-sectional study with a non-probabilistic sample of adults undergoing catheterization. Data were collected through a questionnaire.
ResultsWe included 228 patients, of whom 205 underwent the procedure via the femoral approach and 23 by the radial approach. A 6F arterial sheath was used in all patients. Mean age was 60.0±11.5years and most of them were male (50.4%). The main complaints were lumbar pain in 65.8% and malaise in 32.0% of the cases. In a scale of 0 to 10, the average value assigned for lumbar pain intensity was 5.0±4.2 and 1.5±2.7 for pain at the puncture site. Patients who used the radial approach reported having more pain at the puncture site than patients who used the femoral access (26.8% vs. 52.2%; p=0.01). However, patients who used the femoral approach most often reported lumbar pain (69.8% vs. 30.4%; p < 0.01) and malaise (34.6% vs. 8.7%; p=0.01).
ConclusionsThe predominant discomfort after femoral puncture was lumbar pain and in patients undergoing radial puncture it was pain at the access site. Our findings corroborate the recommendations for a clinical practice that promotes better patient care, including comfort measures, such as the use of cushions, changes in body position, supervised ambulation and the creation of a welcoming environment.
Desconfortos Relatados Pelos Pacientes Após CateterismoCardíaco Pelas Vias Femoral ou Radial
IntroduçãoQueixas são frequentes por parte dos pacientes submetidos a procedimentos invasivos percutâneos. Nosso objetivo foi verificar os desconfortos de pacientes submetidos a cateterismo cardíaco pelas vias femoral e radial.
MétodosEstudo transversal, com amostra não probabilística de adultos submetidos a cateterismo. Os dados foram coletados por meio de questionário.
ResultadosForam estudados 228 pacientes, sendo 205 que realizaram procedimento pela via femoral e 23 pela radial. Em todos os pacientes, foi utilizado o introdutor arterial 6F. A média de idades foi de 60,0±11,5 anos, e a maioria era do sexo masculino (50,4%). As principais queixas foram dor lombar (65,8%) e mal-estar (32,0%). Em uma escala de zero a 10, o valor médio atribuído para a intensidade de dor lombar foi de 5,0±4,2 e de 1,5±2,7 para dor no local da punção. Pacientes que realizaram o procedimento pela via radial referiram ter mais dor no local da punção do que os que utilizaram a via femoral (26,8% vs. 52,2%; p=0,01). No entanto, os pacientes abordados por via femoral relataram mais frequentemente dor lombar (69,8% vs. 30,4%; p < 0,01) e mal-estar (34,6% vs. 8,7%; p=0,01).
ConclusõesO desconforto predominante pós-punção femoral foi a lombalgia e, naqueles submetidos à punção radial, foi a dor no local da punção. Nossos achados remetem a recomendações para a prática clínica que promova a qualidade da assistência, como instituir medidas de conforto ao paciente, como o uso de coxins, mudança de decúbito, auxílio na deambulação e criação de um ambiente acolhedor.
Studies have shown that, despite the increasing technological advancement and of the use of contemporary techniques of diagnostic or therapeutic coronary intervention, discomforts related to the procedures are still observed. 1,2 The radial approach is the option generally preferred by patients because of the increased comfort it brings, compared to the procedure performed via femoral artery. 3 However, the femoral access is still the operator’s choice, providing faster procedures, allowing for repeated interventions and the use of a greater range of materials, and requiring less training than the radial approach. 1 However, the choice of this route requires a period of bed rest, which leads to additional discomfort; furthermore, the in-hospital stay is longer. 4 The radial approach, on the other hand, has the advantage of early ambulation, but presenting, among its limitations, the difficulty of puncture and the small caliber of the artery. 5
It is observed that the manifestations of patients in relation to a prolonged bed rest in the supine position cause back pain and difficulty for physiological eliminations, besides the pain during compression of the access route. From the standpoint of the patient, the search for the origin of these complaints justifies this study. Thus, our goal was to describe the discomforts of patients undergoing cardiac catheterization, comparing radial and femoral access routes.
METHODSCross-sectional study, conducted on patients undergoing cardiac catheterization by radial or femoral access in a private hemodynamics service of Rio Grande do Sul, from April to June 2009. This service has a nurse on the morning-afternoon shift and six nursing technicians divided into two shifts. The sample was of the non-probabilistic type, and were included all patients who agreed to participate, of both genders, aged≥18 years and presenting no complications during the procedure.
Data were collected before the patients were discharged home or for their original unit (intensive care or hospital clinic) by our Hemodynamics Service. At the time of data collection, which was performed by one of the nurses involved in this research, the relevance of the study was explained, when the participation of the patient was requested. The questionnaire was administered after completion of a rest period of 6 hours for patients undergoing procedures via femoral artery, and of 3 hours for patients undergoing procedures via radial access.
The following independent variables – sociodemographic, clinical and procedure-related – were investigated. The dependent variables were: back pain, urinary difficulty, difficulty in walking, embarrassment, hematoma, bruising, discomfort, bleeding, nausea and vomiting. The pain at the puncture site was assessed as the fifth vital sign, noting the intensity through the use of a linear pain scale for comparison between groups (zero meaning total absence of pain; 1–3, pain of low intensity; 4–6, pain of moderate intensity; 7–9, pain of strong intensity, and 10, a excruciating pain). 2 Vascular complications such as hematoma, bruising and slight bleeding were considered according to the literature. 6 Urinary difficulty was assessed as a deficit or inability to urinate during the rest.
The data were analyzed using the Statistical Package for Social Science (SPSS) program, version 14.0. Continuous variables were described as mean±standard deviation. Categorical variables were described as absolute (n) and relative (%) frequencies. To compare means among variables with normal distribution, the t test was used; and to compare categorical variables, the chi-squared test was used. We considered as statistically significant a p-value < 0.05.
This study was approved by the Ethics and Research Committee, Instituto de Cardiologia do Rio Grande do Sul, under number 4246/08. For their inclusion in the study, all patients signed the Term of Free and Informed Consent.
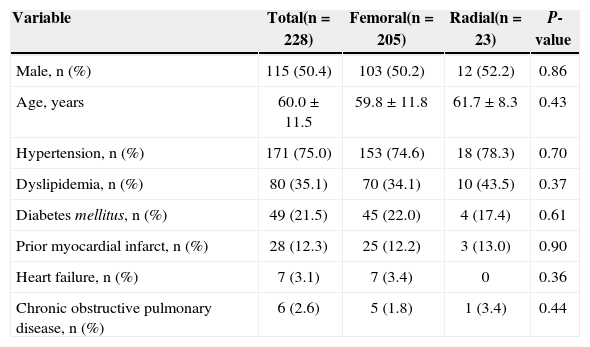
RESULTSOf the 232 patients considered for the protocol, 4 were excluded from analysis due to the occurrence of ischemic stroke, bradycardia, hypotension and allergic reaction. Thus, 228 patients were evaluated, and of these, 205 underwent the procedure via femoral approach, and 23 via radial access. In all patients, a 6F arterial sheath was used. The mean age of the participants was 60.0±11.5years, and most (50.4 %) were male. Other features evaluated can be seen in Table 1.
Sociodemographic and clinical characteristics
| Variable | Total(n=228) | Femoral(n=205) | Radial(n=23) | P-value |
|---|---|---|---|---|
| Male, n (%) | 115 (50.4) | 103 (50.2) | 12 (52.2) | 0.86 |
| Age, years | 60.0±11.5 | 59.8±11.8 | 61.7±8.3 | 0.43 |
| Hypertension, n (%) | 171 (75.0) | 153 (74.6) | 18 (78.3) | 0.70 |
| Dyslipidemia, n (%) | 80 (35.1) | 70 (34.1) | 10 (43.5) | 0.37 |
| Diabetes mellitus, n (%) | 49 (21.5) | 45 (22.0) | 4 (17.4) | 0.61 |
| Prior myocardial infarct, n (%) | 28 (12.3) | 25 (12.2) | 3 (13.0) | 0.90 |
| Heart failure, n (%) | 7 (3.1) | 7 (3.4) | 0 | 0.36 |
| Chronic obstructive pulmonary disease, n (%) | 6 (2.6) | 5 (1.8) | 1 (3.4) | 0.44 |
Of the total sample of patients, 70 (30.7 %) had previously a cardiac catheterization performed, 33 (14.5%) percutaneous coronary intervention and 11 (4.8%) coronary artery bypass grafting.
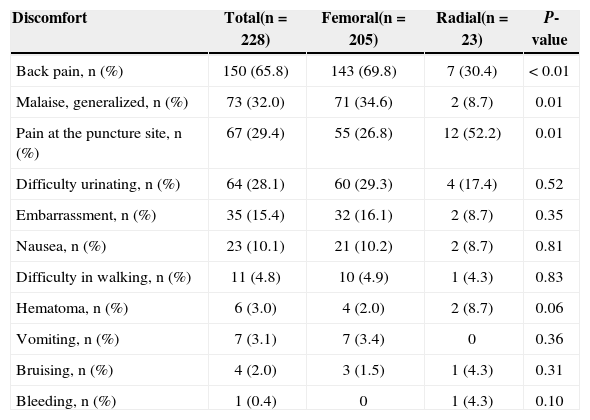
On a scale of zero to 10, the mean value attributed by patients to the intensity of low back pain was 5.0±4.2 and 1.5±2.7 for pain at the puncture site. Patients who underwent the procedure by radial approach reported having more pain at the puncture site than those who used the femoral artery (26.8 % vs. 52.2 %; p=0.01). However, patients approached via the femoral artery reported more often back pain (69.8 % vs. 30.4 %; p < 0.01) and a generalized malaise (34.6 % vs. 8.7 %; p=0.01). These data are shown in Table 2.
Discomforts and complications reported by patients
| Discomfort | Total(n=228) | Femoral(n=205) | Radial(n=23) | P-value |
|---|---|---|---|---|
| Back pain, n (%) | 150 (65.8) | 143 (69.8) | 7 (30.4) | < 0.01 |
| Malaise, generalized, n (%) | 73 (32.0) | 71 (34.6) | 2 (8.7) | 0.01 |
| Pain at the puncture site, n (%) | 67 (29.4) | 55 (26.8) | 12 (52.2) | 0.01 |
| Difficulty urinating, n (%) | 64 (28.1) | 60 (29.3) | 4 (17.4) | 0.52 |
| Embarrassment, n (%) | 35 (15.4) | 32 (16.1) | 2 (8.7) | 0.35 |
| Nausea, n (%) | 23 (10.1) | 21 (10.2) | 2 (8.7) | 0.81 |
| Difficulty in walking, n (%) | 11 (4.8) | 10 (4.9) | 1 (4.3) | 0.83 |
| Hematoma, n (%) | 6 (3.0) | 4 (2.0) | 2 (8.7) | 0.06 |
| Vomiting, n (%) | 7 (3.1) | 7 (3.4) | 0 | 0.36 |
| Bruising, n (%) | 4 (2.0) | 3 (1.5) | 1 (4.3) | 0.31 |
| Bleeding, n (%) | 1 (0.4) | 0 | 1 (4.3) | 0.10 |
The mean size of hematomata and bruising was 2.3±1.0cm and 2.3±0.5cm, respectively.
Other discomfort perceived by patients was reported, in addition to those inquired by researchers. The most commonly cited by patients were dyspnea (2.6%), headache (2.2%), dizziness (1.3%) and stomach pain (1.3%).
DISCUSSIONIn this study we identified the discomforts reported by patients undergoing cardiac catheterization by radial or femoral access, and this gave us subsidies to improve the care provided by the health team. The identification of the most frequent complaints of patients in daily care practice in our Hemodynamics Service is necessary, because it allow us to establish a qualified care, targeted for the resolution of problems.
The sample was composed mostly of male patients with a mean age of 60.2years, which shows that people of older age are being increasingly subjected to percutaneous procedures. The highest risk of vascular complications at the puncture site usually occurs in elderly patients, with the use of the femoral approach. 7 The identification of risk factors for vascular complications during or after such procedures is important, for the development of protocols in order to stop or minimize these complications. 7
Nevertheless, the findings of the present study allowed us to verify that there was no difference in the vascular complications in both access routes (radial and femoral). However, the study A Randomized Comparison of Percutaneous Transluminal Coronary Angioplasty by the Radial, Brachial and Femoral Approaches: The Access Study, or simply Access, as it is called, which compared 900 patients undergoing percutaneous coronary intervention by radial, brachial and femoral techniques, found a significant decrease in complications related to radial access, in relation to the other two routes. 8 On the other hand, in a meta-analysis evaluating 3,224 patients in 12 randomized studies comparing the radial and femoral techniques for coronary angiography and percutaneous coronary intervention procedures, it was demonstrated that the radial approach is safe and effective when compared to the femoral technique, with less access route complications (odds ratio [OR]=0.20, 95% confidence interval [CI], 0.09-0.42; p < 0.0001), even at the expense of higher chances of procedure failure (OR=3.30; 95% CI, 1.63-6.71; p < 0.001). 9
The results of this study demonstrate that the patients with procedures performed via femoral artery reported increased discomfort regarding back pain and malaise, with differences between groups. These complaints may be directly related to the prolonged bed rest. A randomized study of 169 patients was carried out to evaluate the effects of the application of a weight (sandbag) on the femoral access site after the procedure and of patient’s repositioning on the bed, compared to the rate of vascular complications and the severity of low back pain related to the duration of the post-procedure rest. 10 The results of this study indicate that the back pain was reported more frequently in patients whose positions were not changed and whose head end of the bed was raised (p < 0.05). 10 The same study suggested that, to increase comfort and diminish the back pain, the patients may change their position on the bed; and the head end of the bed can be positioned at about 30° or 45°. 10 Data from a randomized trial that evaluated the effect of intermittent mobilization on the bed after the completion of the catheterization via femoral route showed that patients in the intervention group reported less back pain than those in the control group (p=.00). There was no significant difference between the groups, regarding the presence of bleeding. 11
The change in sleeping position can also reduce the pain, promoting physical comfort and minimizing the possible negative feelings that patients have in relation to coronary angiography. 12 A quasi-experimental study involving 105 patients to investigate the effect of three protocols for positioning on back pain, heart rate, blood pressure and vascular complications after cardiac catheterization concluded that changing position on the bed and using a supporting pillow during the first hours after cardiac catheterization can effectively minimize the pain and the hemodynamic instability, without increasing possible vascular complications. 12 Another strategy to reduce low back pain is the use of devices such as the Siriraj Leg Lock ®, that are intended to immobilize only the limb punctured, allowing the mobility of other body parts. A randomized clinical trial that evaluated its use in 51 patients undergoing percutaneous coronary intervention (intervention group) showed significant reduction in back pain, compared to the control group (p < 0.001). 13
Several studies have shown that it is possible to reduce the time of absolute bed rest. A study conducted in São Paulo proved that this is possible with the use of 4F catheters via femoral artery, because even in the case of a percutaneous coronary intervention, early ambulation (mean 60±5min) did not cause more bleeding complications, besides being simpler, less traumatic and less invasive. 14 In another study, a randomized clinical trial in which the participants underwent intervention via femoral artery using an 6F arterial sheath and with an activated clotting time < 350 seconds, the sheath was removed at the end of the procedure, with ambulation after 3 hours of sleep. This study revealed that a careful nursing observation after a percutaneous intervention with removal of the arterial sheath and early ambulation offers comfort, safety and patient satisfaction. 4
The findings of this study motivate the development of strategies to minimize the most common complaints, besides providing a more humane care, relieving the patients’ physical and psychic pain. The nursing care before and after procedure should be directed to the prevention and detection of complications. 15 Attention to the patient must be careful, because on many occasions patients in pain may exhibit elevated blood pressure, thus leading to bleeding at the puncture site, and in some situations, leading to more serious complications.
Among other discomforts reported by our patients, we emphasize headache, shortness of breath and dizziness. These data demonstrate that patients in the periprocedural period have several complaints, which can be prevented and controlled by the multidisciplinary team. One must consider that the waiting period for the exam, the peculiarities of each patient, the complications that arise during the procedures and unexpected results are stressors, further aggravating the physical/mental condition. Therefore, the team must be aware of these signs and symptoms to, in so far as possible, mitigate them.
A study that evaluated the factors that predict the level of discomfort after a coronary angiography showed that patients who had previous experience with these procedures received prior information about the next procedure, showed no dysuria and slept well after the procedure. These patients were also less likely to complain of discomfort. 16 Finally, it is important to remember that each patient has special features, such as pre-existing diseases of the spine (herniated disc and previous surgeries), previous urinary difficulty (urinary retention and prostatic hyperplasia), increased sensitivity to pain, weakness, motor and cognitive difficulty – which often are associated with advanced age and/or associated diseases. This information should be investigated by the professional team before the procedure, so that an individualized plan be carried out to minimize the discomforts. Therefore, the choice of the access route, when possible, can be useful as a strategy for not enhancing these problems.
CONCLUSIONSIn evaluating the discomforts of patients undergoing cardiac catheterization by femoral and radial access, we identified that the predominant discomfort post-femoral puncture was low back pain and, in those undergoing radial puncture, was pain at the puncture site. When comparing the groups, it was found that patients who underwent procedures via the femoral artery reported increased discomfort regarding lower back pain and general malaise.
The findings of this study remit to recommendations for a clinical practice that promotes quality of care and how to establish measures of patient comfort (such as the use of cushions, change in position, helping with ambulation, a warm atmosphere and a constant monitoring of vital signs). Furthermore, the identification of risk factors for complications in the vascular bed or at the puncture site creates the opportunity for a more individualized care. The formulation of protocols can include basic and advanced measures of comfort, according to the chosen route of access for the procedure, making the period of rest something less tiring and uncomfortable. It is essential that the professional team be alert to the signs of discomfort expressed by patients to promptly minimizing them, promoting an earlier recovery and a more humanized care.
CONFLICTS OF INTERESTThe authors declare no conflicts of interest.
SOURCE OF FINANCINGNone.