




To describe the impact of the Covid-19 pandemic on the interventional radiology unit at our hospital in the first year of the pandemic.
Material and methodsThis prospective observational study included 83 consecutive patients with confirmed SARS-CoV-2 infections who underwent an interventional radiology procedure in the period comprising March 13, 2020 through March 13, 2021. We describe the repercussions of the situation on the unit's total activity, as well as on its activity during the different phases of the pandemic.
ResultsTechnical and clinical success were achieved in 96.43% and 82.14% of cases, respectively. During follow-up throughout the year, 68 patients remained alive and 15 died from their underlying disease. No complications related with interventional procedures occurred, and activity declined by only 12% in comparison with the same period in the previous year (2019-2020, without COVID). Similarly, the decrease in relative value units and radiology activity units was only 13% and 12%, respectively.
ConclusionThe Covid-19 pandemic has been a challenge in our daily work, leading to an overall decrease in the number of procedures. Nevertheless, the interventional radiology unit has been actively involved in caring for Covid-19 patients, performing a wide variety of necessary procedures. Following a series of specific measures and protocols has enabled us to perform interventional radiology procedures safely during the pandemic.
Describir el impacto que la pandemia de COVID-19 ha supuesto en la Unidad de Radiología Intervencionista de nuestro hospital a lo largo de un año.
Materiales y métodosSe ha realizado un estudio observacional prospectivo en 83 pacientes consecutivos con infección confirmada por COVID-19 a los cuales se les realizó algún tipo de procedimiento de radiología intervencionista durante el periodo comprendido entre el 13 de marzo del 2020 y el 13 de marzo de 2021. Se describe la repercusión de la situación en la actividad total de la unidad, así como en las diferentes fases de la pandemia.
ResultadosSe alcanzó el éxito técnico y clínico en el 96,43% y 82,14% de los casos, respectivamente. Durante el seguimiento a lo largo de un año, 68 pacientes seguían vivos y 15 fallecieron a causa de su enfermedad de base. No se produjeron complicaciones relacionadas con los procedimientos intervencionistas y nuestra actividad decayó solo un 12% en comparación con el mismo período del año 2019-2020 (no-COVID). Asimismo, solo se produjo una reducción en unidades relativas de valor y unidades de actividad radiológica del 13% y del 12%, respectivamente.
ConclusiónLa pandemia de COVID-19 ha supuesto un desafío en nuestro trabajo diario condicionando una reducción general en el número de procedimientos. No obstante, la radiología intervencionista ha participado activamente en la atención de los pacientes con COVID-19 mediante la realización de una amplia variedad de intervenciones necesarias. La atención de la radiología intervencionista pudo realizarse de forma segura durante la pandemia, siguiendo una serie de medidas y protocolos específicos.
From the start of the pandemic in Wuhan, China, in late 2019, to March 2021, the COVID-19 pandemic can be said to have represented a major challenge for healthcare systems worldwide, which have had no choice but to outdo themselves once again to achieve better care with whatever resources have been available at any given time.
This has had a significant impact on hospitals and health centres. In particular, it has had a significant impact on interventional radiology suites, the subject of this study. Consequently, ways of working have changed, schedules have been reorganised, steps have been taken to protect professionals and extreme measures for cleaning facilities and equipment have been established (Fig. 1).
 wearing personal protective equipment.")
The objective of this study is to report the impact of the COVID-19 pandemic on the interventional radiology unit at our hospital over the course of one year.
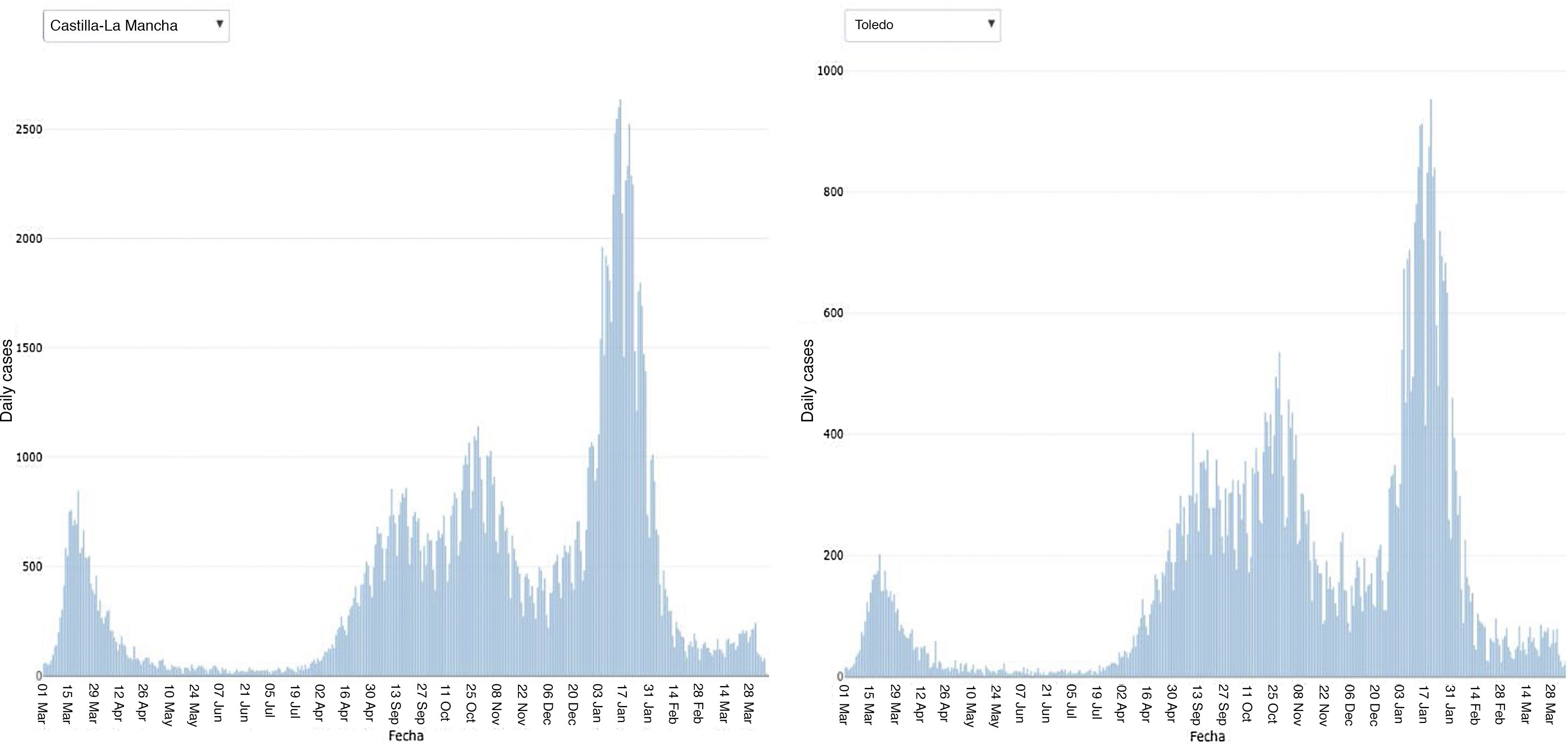
Epidemiology dataIn the context of the COVID-19 pandemic, the first cases reported in the province of Toledo occurred on 3 March; from that point on, numbers of cases, and with them numbers of admissions and deaths, increased exponentially, peaking in our region on 1 April 2020. The mortality rate during the first wave in our region was 147.74 deaths per 100,000 population.1 Numbers of cases recorded daily in Castilla-La Mancha and in Toledo in the course of the pandemic appear in Fig. 2.

Graph of daily cases over the course of one year of the pandemic in the Autonomous Community of Castilla-La Mancha and the province of Toledo.2
However, the pandemic has exhibited inconsistent behaviour over time, such that three phases or waves may be distinguished:
The first wave spanned 13 March to 21 June 2020 (the end of the first state of alarm); in it, 4,145 cases and 794 deaths (38.2% of all deaths during the pandemic) were recorded in the province of Toledo. During this phase, COVID-19 spread uncontrollably and cases grew exponentially. Hospital overload peaked on 1 April 2020, with 600 conventional beds occupied (80% of the total hospital capacity); a threefold increase in the number of intensive care unit (ICU) spots required (76 beds); and the need to open more critical-care beds at other hospitals in the city (Hospital Provincial [Provincial Hospital] and Hospital Nacional de Parapléjicos [National Hospital for Paraplegics]).
The second phase went from 22 August to 1 December 2020. The start of that phase was marked by the return of holidays and freer movement among Autonomous Communities, accounting for a gradual increase in new cases and ward and ICU hospitalisations, until the province of Toledo reached a cumulative incidence (CI) of 245 cases per 100,000 population. During this phase, a total of 30,036 new cases were reported, partly as a result of heightened availability of rapid tests and polymerase chain reaction (PCR) tests in comparison to the first wave, and 572 total deaths were documented. The peak of the pandemic during this phase occurred on 2 November, when 364 admissions to conventional beds and 34 admissions to ICU spots were reported.
The third phase started on 1 December 2020 and ended on 13 March 2021, the date on which this study was closed. That phase was defined by travel to and from national and regional festivities and family gatherings around Christmastime, again resulting in an unrelenting increase in new cases and admissions that peaked on 1 February, when 448 ward admissions were documented and 103 ICU beds were reported to be occupied. The number of deaths recorded in this phase was 1,772.
A year into the pandemic, on 13 March 2021, 62,611 individuals in the province of Toledo had had COVID-19 and 2,083 had died of the disease.
Material and methodsAn observational, prospective study was conducted of consecutive cases of patients with confirmed COVID-19 seen in our interventional radiology department during the pandemic, from 13 March 2020 to 13 March 2021. To conduct the study, the following were collected: demographic data (sex and age); intervention date; reason for the order and its urgency; and, as endpoints, the technical success and the clinical success of the procedure. Technical success was defined as a good final review of the interventional procedure, and clinical success was defined as improvement of patient symptoms. Patients were followed up until the date of submission of the paper. In addition, deaths during the follow-up period were counted. All patients signed the corresponding informed consent form, and the approval of the hospital's independent ethics committee (IEC) was obtained.
Overall healthcare activity on our unit during the period indicated was also recorded. The types of procedure performed, in accordance with the guidelines of the hospital board, were emergency and oncological procedures that could not be delayed. Elective cases were postponed, in particular during the first two waves of the pandemic. For the performance of these procedures, due to the high rate of infections transmitted by aerosols and through contact with contaminated surfaces,3 patients had to be divided into groups in order to prevent new infections.
Patient management was conducted according to the guidelines and protocols established by the World Health Organization (WHO),4 the Spanish Ministry of Health and the different Spanish Regional Ministries of Health, as well as the recommendations for action described by the Sociedad Española de Radiología Vascular Intervencionista [Spanish Society of Vascular and Interventional Radiology] (SERVEI),5 the Sociedad Española de Radiología Médica [Spanish Society of Medical Radiology] (SERAM)6 and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE),7 among others.
The reader is referred to an article by Cifuentes8 describing the manner in which angiography suites were reorganised and the measures that were implemented and carried out throughout the conduct of the study and that currently remain in place at our centre.
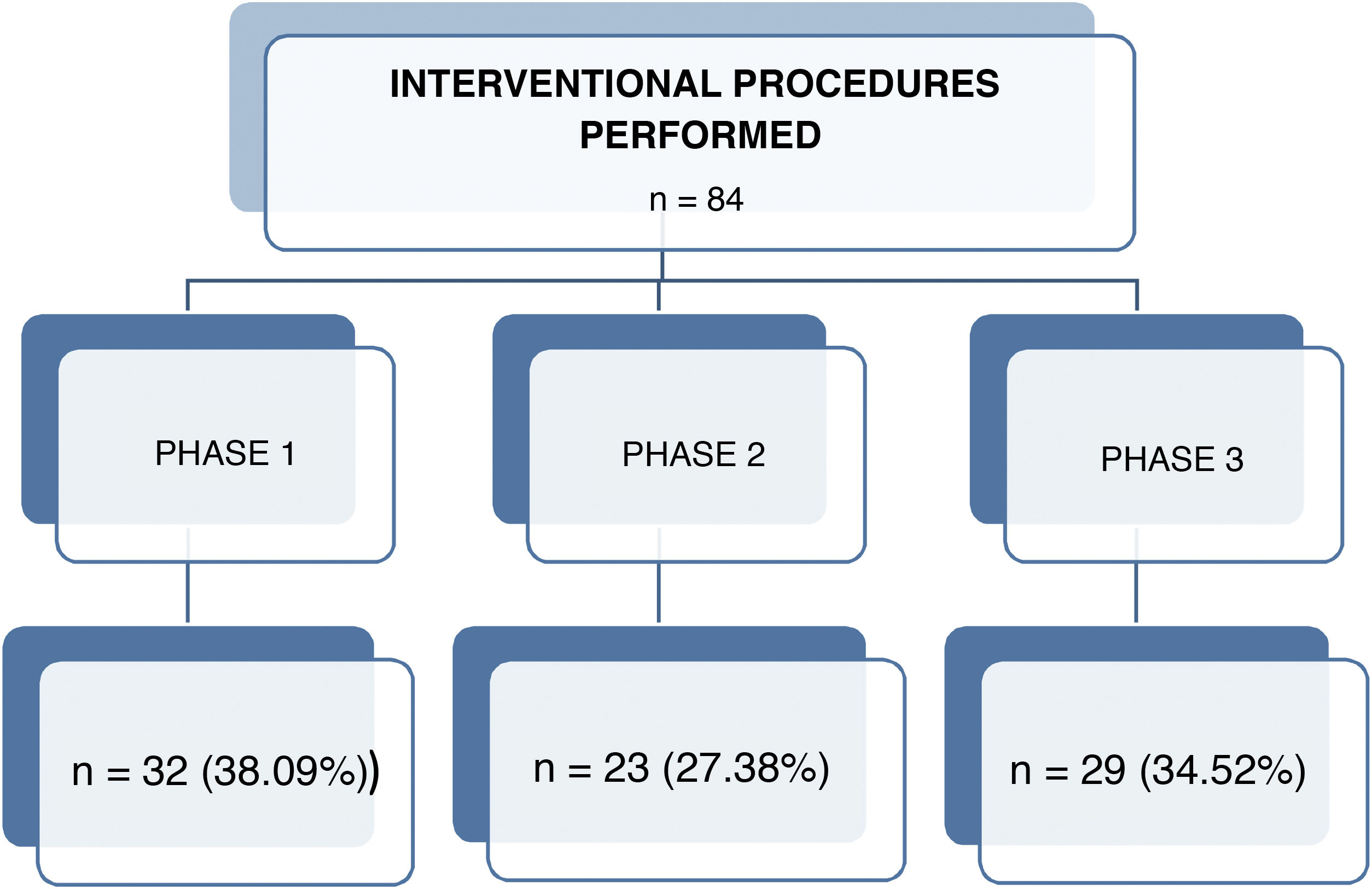
ResultsDuring the study period, a total of 2,326 interventional radiology procedures were performed; of them, 84 were performed in 83 patients with COVID-19 (mean age: 49 years; age range: 21-94 years; 45 men/38 women) (Fig. 3).

Out of all interventional procedures, 38.09% (n = 32) were performed in phase 1, 27.38% (n = 23) were performed in phase 2 and 34.52% (n = 29) were performed in phase 3; 50 procedures had been planned and 34 were emergency procedures.
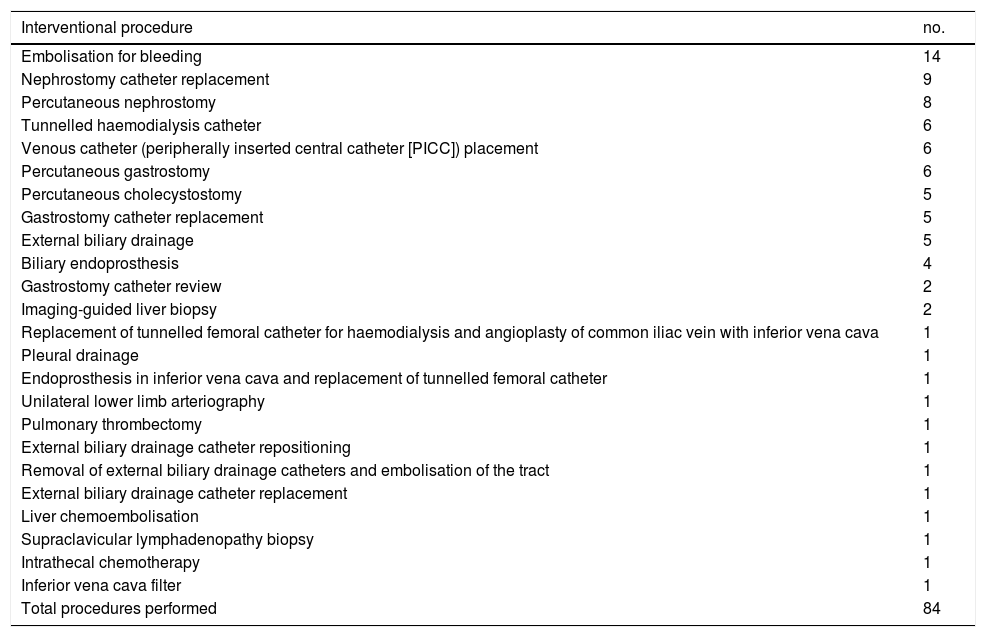
The different types of procedures performed in the patients included in our study appear in Table 1. Those performed most often were embolisation for bleeding (16.6%), central venous catheter placement (14.2%), nephrostomy catheter replacement (10.7%), percutaneous nephrostomy (9.5%), percutaneous gastrostomy (7.1%), percutaneous cholecystostomy (5.9%), gastrostomy catheter replacement (5.9%), external biliary drainage (5.9%) and biliary endoprosthesis placement (4.7%) (Figs. 4–6).
Interventional procedures performed in patients with COVID-19.
| Interventional procedure | no. |
|---|---|
| Embolisation for bleeding | 14 |
| Nephrostomy catheter replacement | 9 |
| Percutaneous nephrostomy | 8 |
| Tunnelled haemodialysis catheter | 6 |
| Venous catheter (peripherally inserted central catheter [PICC]) placement | 6 |
| Percutaneous gastrostomy | 6 |
| Percutaneous cholecystostomy | 5 |
| Gastrostomy catheter replacement | 5 |
| External biliary drainage | 5 |
| Biliary endoprosthesis | 4 |
| Gastrostomy catheter review | 2 |
| Imaging-guided liver biopsy | 2 |
| Replacement of tunnelled femoral catheter for haemodialysis and angioplasty of common iliac vein with inferior vena cava | 1 |
| Pleural drainage | 1 |
| Endoprosthesis in inferior vena cava and replacement of tunnelled femoral catheter | 1 |
| Unilateral lower limb arteriography | 1 |
| Pulmonary thrombectomy | 1 |
| External biliary drainage catheter repositioning | 1 |
| Removal of external biliary drainage catheters and embolisation of the tract | 1 |
| External biliary drainage catheter replacement | 1 |
| Liver chemoembolisation | 1 |
| Supraclavicular lymphadenopathy biopsy | 1 |
| Intrathecal chemotherapy | 1 |
| Inferior vena cava filter | 1 |
| Total procedures performed | 84 |
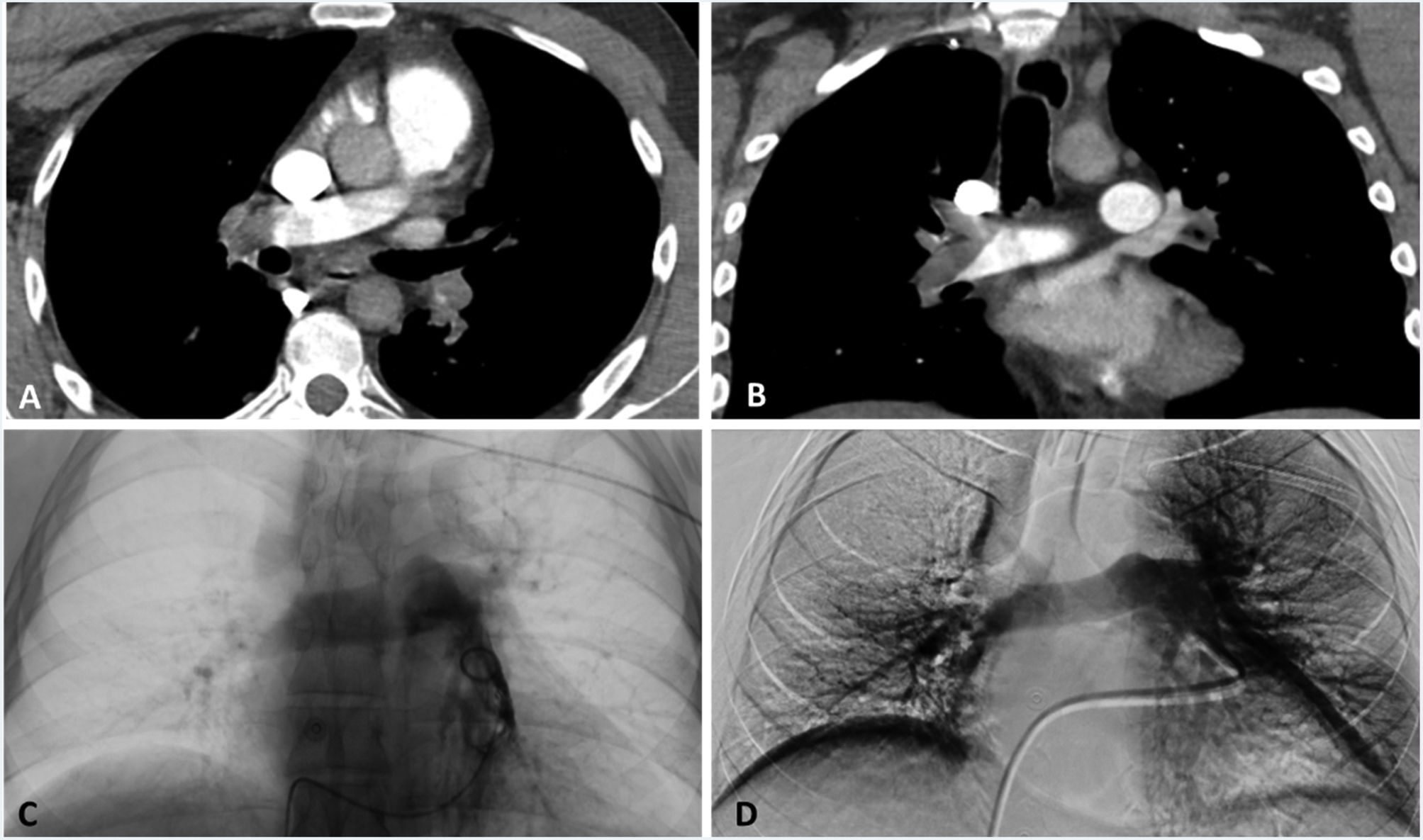
 showing findings consistent with bilateral acute pulmonary thromboembolism in both main pulmonary arteries, confirmed on angiography (C). Thromboaspiration was then performed, achieving partial repermeation of the pulmonary branches (D) with an approximately 70% reduction in thrombotic load.")
Pulmonary artery thrombectomy performed in phase 1. Computed tomography images on axial and coronal planes (A-B) showing findings consistent with bilateral acute pulmonary thromboembolism in both main pulmonary arteries, confirmed on angiography (C). Thromboaspiration was then performed, achieving partial repermeation of the pulmonary branches (D) with an approximately 70% reduction in thrombotic load.
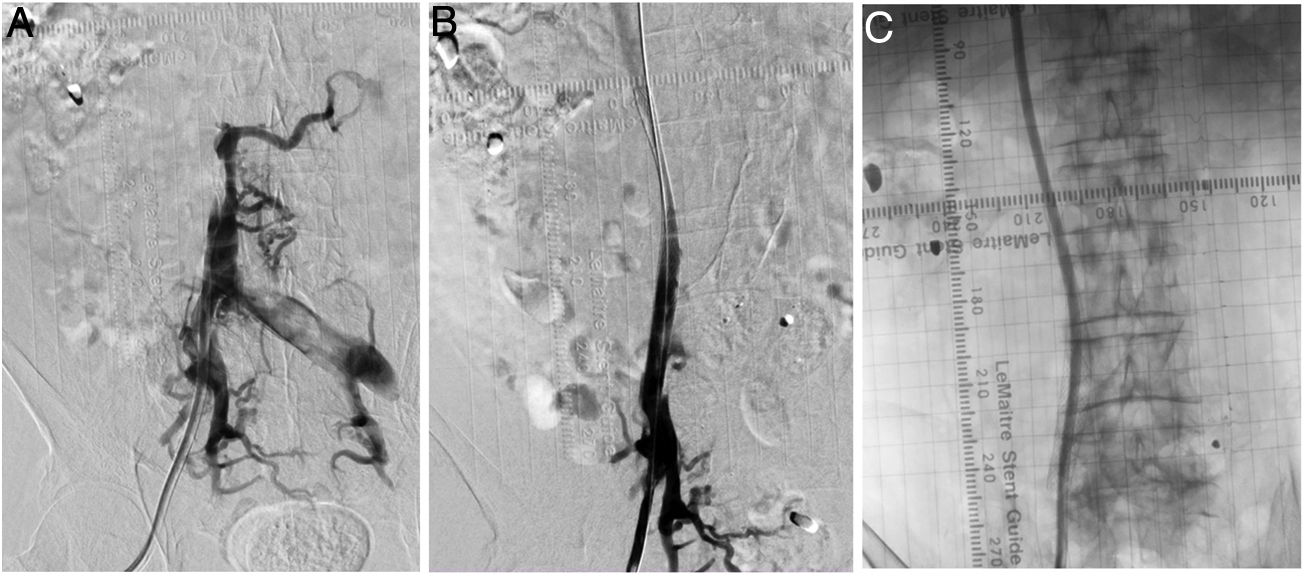
. Angioplasty and endoprosthesis repositioning were then performed in a second procedure (B), as was placement of a tunnelled femoral catheter through the endoprosthesis to the right atrium, all with satisfactory outcomes (C).")
Dysfunctional right femoral haemodialysis catheter in phase 2. An angiogram revealed severe inferior vena cava stenosis with drainage to collateral circulation (A). Angioplasty and endoprosthesis repositioning were then performed in a second procedure (B), as was placement of a tunnelled femoral catheter through the endoprosthesis to the right atrium, all with satisfactory outcomes (C).
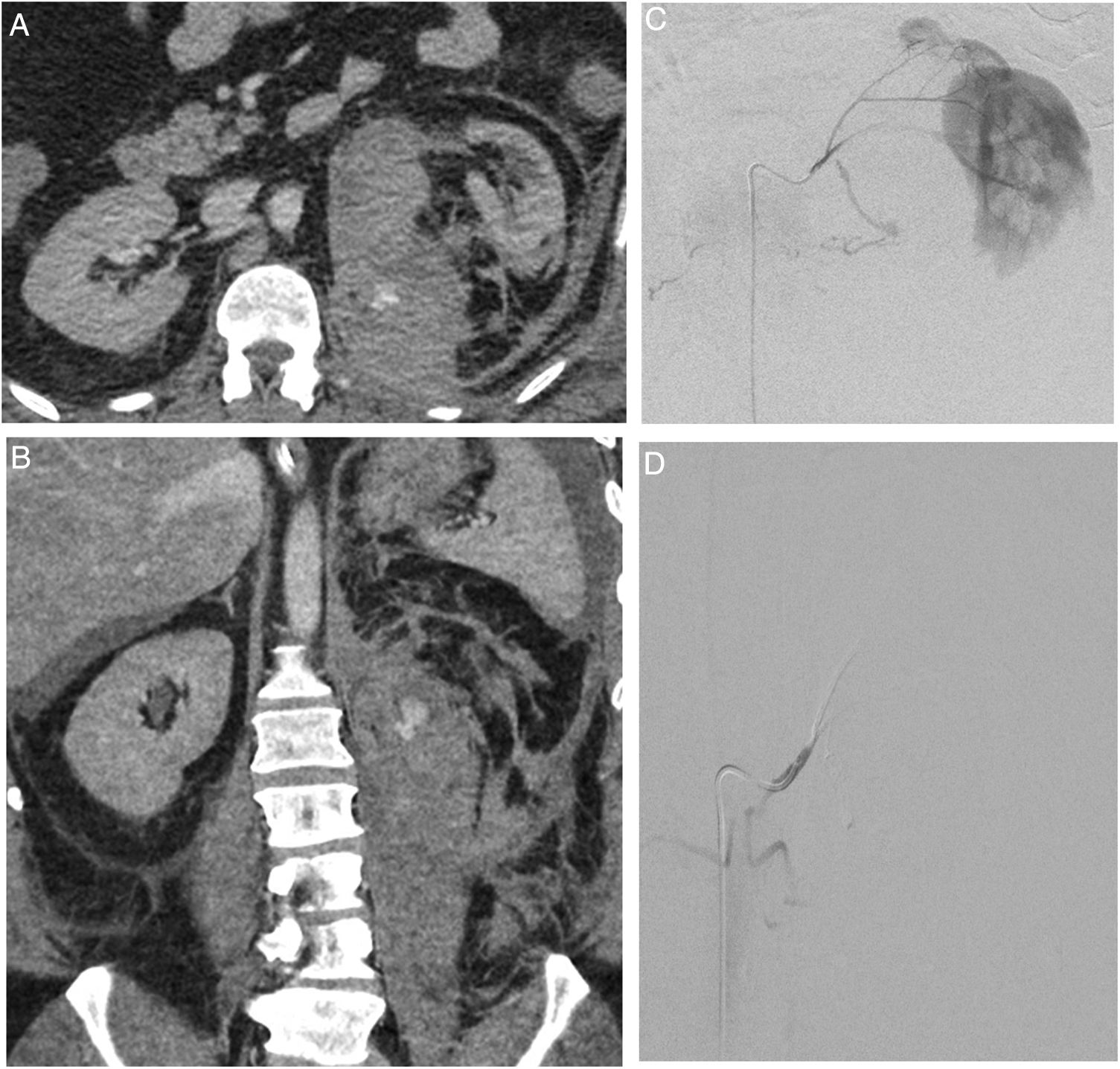
 showing findings consistent with left retroperitoneal haematoma with signs of active arterial bleeding confirmed on angiography (C). Contrast extravasation dependent on the superior left renal artery branch (C), which was embolised with particles and Glubran, achieving complete cessation of bleeding in the final check-up (D).")
Embolisation for active renal arterial bleeding performed in phase 3. Computed tomography images on axial and coronal planes (A-B) showing findings consistent with left retroperitoneal haematoma with signs of active arterial bleeding confirmed on angiography (C). Contrast extravasation dependent on the superior left renal artery branch (C), which was embolised with particles and Glubran, achieving complete cessation of bleeding in the final check-up (D).
Technical success was achieved in 96% of patients, and clinical success was achieved in 82%. None of the procedures were associated with any complications. During patient follow-up, 15 patients died due to underlying disease; 68 are still alive.
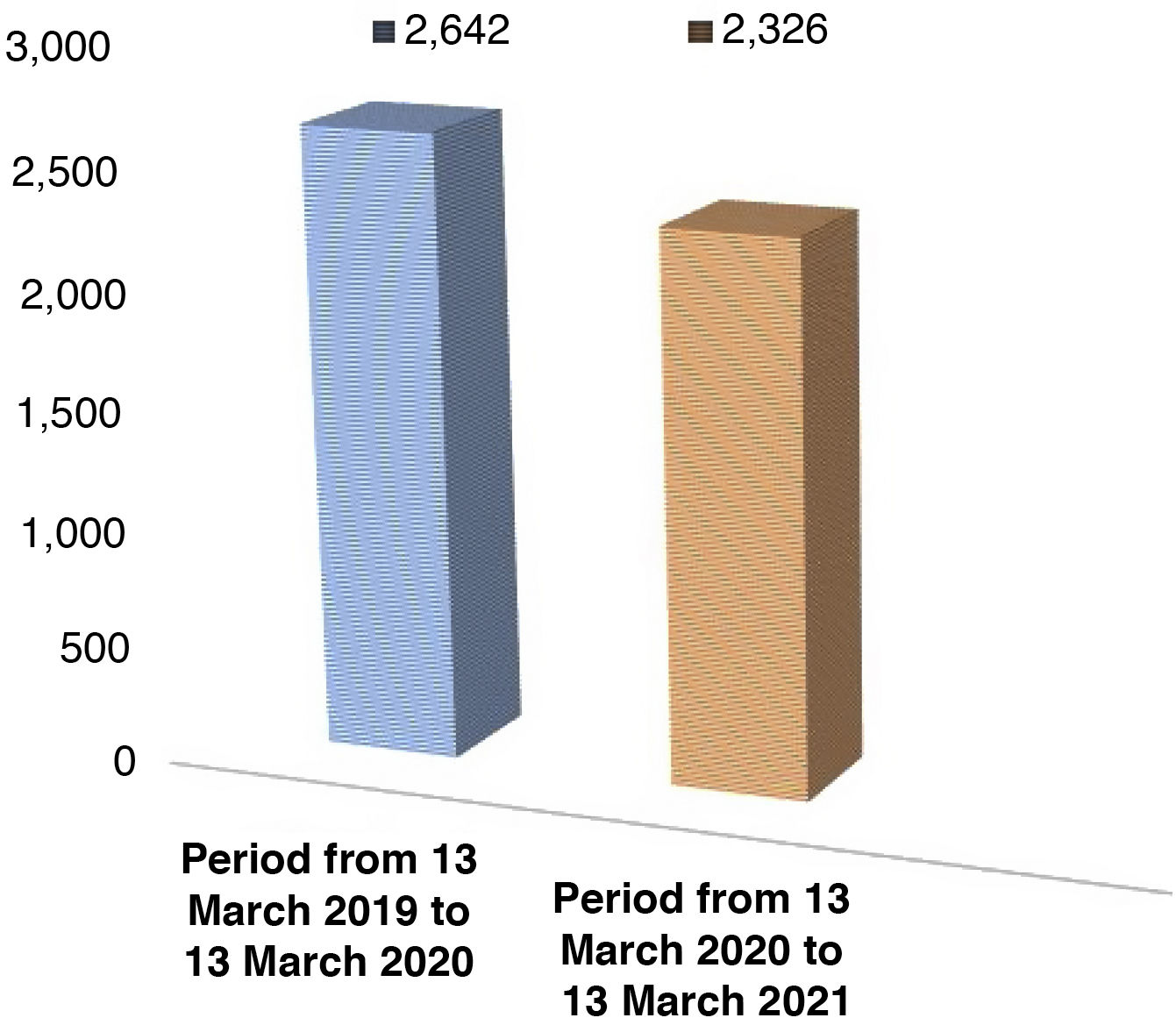
A comparison graph shows the total activity recorded in the period from 13 March 2019 to 13 March 2020 versus the period from 13 March 2020 to 13 March 2021 (Fig. 7), with a 12% decrease in healthcare activity having been reported compared to the same period in 2019 (2,326 current patients 2020-2021 versus 2,642 patients seen in 2019-2020), but with different behaviour depending on the phase: whereas in phase 1 activity decreased by 38.71%, in phases 2 and 3 there was a 9.61% upturn in activity in the 2020-2021 period.

In addition, relative units of value decreased by only 13% and units of radiological activity dropped by just 12%.
Concerning the extent to which interventional radiology suite staff were affected by COVID-19, just two staff members had the disease, in November and December; they had mild symptoms and adopted the corresponding isolation measures during the required quarantine period.
DiscussionVarious articles from around the world have been published on the organisation of interventional radiology suites and the management of these patients. Articles by Ierardi et al.,9 Da Zhuang et al.10 and Too et al.11 reported the preventive measures established at those authors' respective hospitals. Other authors such as Zhu et al.12 contributed numerical data on patients seen when the incidence of the disease peaked in their region.
In addition, more recent articles such as one by Dine et al.13 have referred to the recommendations of the Swiss Society of Vascular and Interventional Radiology for the preparation of a workflow to cope with the pandemic. Iezzi et al.14 compared the activity in the interventional radiology suite during the COVID era, from January to April 2020, to the same period during the non-COVID era, in 2019; examining only a 2.5-month period, Zhong et al.15 reported the impact of the pandemic on six interventional radiology departments in the United Kingdom, comparing a period of approximately one pre-pandemic month (March to April 2019) to the pandemic period (March to April 2020).
Finally, Lee et al.16 highlighted the role of interventional radiology in the treatment of patients hospitalised with COVID-19; they conducted a retrospective review of hospitalised patients positive for COVID who underwent some sort of interventional procedure at a leading tertiary hospital in New York City. After a mean follow-up of 4.3 months, 1.1% of patients remained hospitalised, 16.3% died and 82.6% were discharged.
At present, our study is the only one that has performed one-year follow-up of patients with COVID-19 having undergone some sort of interventional procedure and that has studied variables such as the age and sex of the patients and the technical and clinical success of the procedures. Our study also examined the impact of the pandemic during that year on overall interventional radiology suite activity, comparing the data collected in this regard to the same period in the previous year, and reported an overall 12% decrease in healthcare activity, but with different behaviour by phase. This reflected the scant delay afforded by interventional procedures; during phases 2 and 3, some postponed procedures had to be performed, resulting in an increase in activity.
Analysis of the patient and activity data recorded in the above-mentioned articles revealed a surprising reduction in activity mentioned in the article from China:10 60%, with all phases taken into account, compared to our 12%. This might have been related to either the extent of the measures demanded by the Chinese government to ensure control of infection transmission. Alternatively, it might have been tied to the high healthcare burden under normal conditions at the hospital in Zhongda — substantially higher than our own in terms of number of preferential procedures, which were the most heavily curtailed. Also notable was the reduction in activity cited in an article from the United Kingdom15 — 31% versus our 12% — which could perhaps be attributed to that article's one-month analysis period.
Also striking were the large numbers of patients with COVID-19 treated by us compared to Singapore.17 This difference may have been due to the duration of each study and the prevalence and incidence of the disease when each study was conducted.
Finally, as a limitation of our study we can mention that, as it was a prospective study, we focused on patients with COVID-19, such that it was not possible to have a control group of non-COVID patients during the year of the pandemic, and therefore we were unable to compare the data to said control group.
In conclusion, the COVID-19 pandemic has represented a challenge in our day-to-day work, with a general reduction in numbers of procedures. However, interventional radiology has actively participated in the care of patients positive for COVID-19 by performing a wide variety of necessary procedures that could be performed safely during the pandemic with adherence to a number of specific measures and protocols.18
Authorship- 1
Responsible for study integrity: PBR, ICG, CLP.
- 2
Study concept: PBR, ICG, CLP.
- 3
Study design: PBR, CLP.
- 4
Data collection: PBR, ICG, IDP, FA, VSML, CLP.
- 5
Data analysis and interpretation: PBR, CLP.
- 6
Statistical processing: PBR.
- 7
Literature search: PBR, CLP.
- 8
Drafting of the article: PBR, ICG, CLP.
- 9
Critical review of the manuscript with intellectually significant contributions: PBR, ICG, IDP, FA, VSML, CLP.
- 10
Approval of the final version: PBR, ICG, IDP, FA, VSML, CLP.
The authors declare that they have no conflicts of interest.
Please cite this article as: Barón-Ródiz PA, Cifuentes-García I, Domínguez-Paillacho ID, Antezana F, San Martín-Luque V, Lanciego Pérez C. Un año completo de pandemia COVID-19 y su impacto en la Unidad de Radiología Intervencionista. Radiología. 2022;64:3–10.

