




We present a case of a 53-year-old man with a pT1G3 bladder carcinoma confirmed by transurethral resection (TURBT). The patient developed bacterial cystitis and after resolution, he was started on Bacillus-Calmette-Guérin (BCG) therapy (BCG OncoTice® 2−8 × 108) during six sessions.
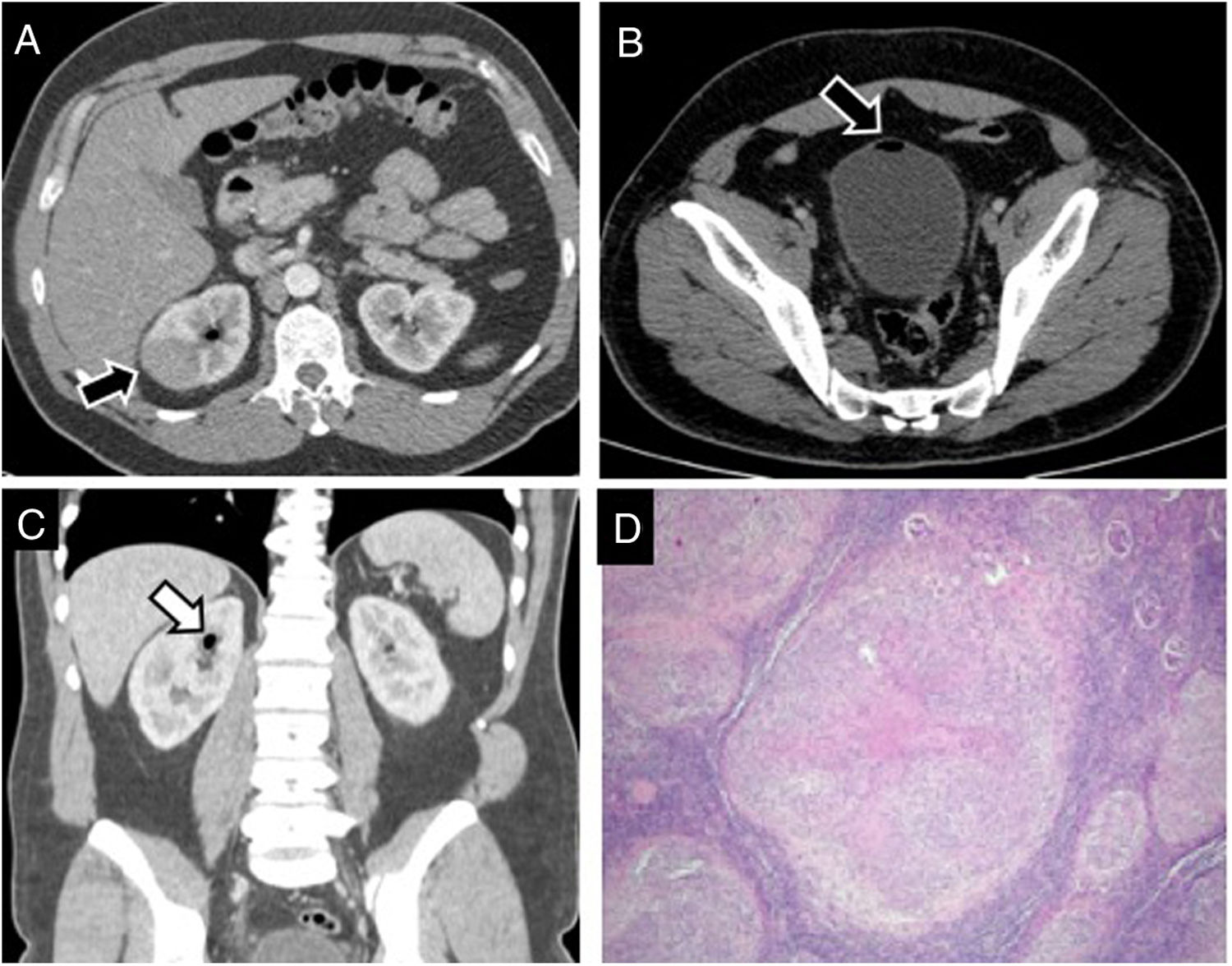
After TURBT, a routine follow-up CT was performed that showed a homogeneous solid mass in the right kidney upper pole (Fig. 1A–C), firstly diagnosed as a renal tumour, suspected to be a renal cell carcinoma.
 show a hypoattenuated focal lesion (arrow) in the upper pole of the right kidney. B, C. Presence of gas into the bladder (arrow in B) and the superior collector system (arrow in C) is seen that presumes vesicoureteral reflux after transurethral resection. D. Low power examination of renal parenchyma revealing the presence of multiple nodular lesions throughout the whole specimen (hematoxylin and eosin staining, 4×).")
A. Contrast-enhanced venous phase CT images (A, B axial; C, coronal view) show a hypoattenuated focal lesion (arrow) in the upper pole of the right kidney. B, C. Presence of gas into the bladder (arrow in B) and the superior collector system (arrow in C) is seen that presumes vesicoureteral reflux after transurethral resection. D. Low power examination of renal parenchyma revealing the presence of multiple nodular lesions throughout the whole specimen (hematoxylin and eosin staining, 4×).
The patient underwent partial nephrectomy obtaining tissue samples without malignant cells. Pathology examination demonstrated caseating and non-caseating granulomas (Fig. 1D).
A follow-up CT examination, performed eighteen months after TURBT, demonstrated a new hypoenhancing solid lesion similar to the initial mass and located in the right kidney upper pole near previous scar (Fig. 2). Relapsing of granulomatous affectation was suspected and patient was treated with rifampicin, isoniazid and ethambutol with a complete resolution on posterior imaging studies.
 obtained after surgical resection of the renal lesion show a new hypoattenuated focal lesion (arrows) next to the renal scar with similar characteristics of the removed one.")
BCG is an effective medical treatment for carcinoma in situ and non-muscle invasive bladder cancer after transurethral resection. It has demonstrated to be more effective than TURBT alone or intravesical chemotherapy following TURBT.1 The activation of the immune system after BCG administration into the bladder induces a complex inflammatory response that is the base of the therapeutic effect of this treatment.
Intravesical BCG instillation is well tolerated and expected complications are not severe. Short-term symptoms of cystitis occur in up to 90% of patients due to the immune stimulation. Also, mild hematuria, low-grade fever and myalgias are common and usually of limited duration. Serious systemic complications are rare; life-threatening BCG sepsis has been reported in only 0.4% of patients.2
Development of a granulomatous affectation in solid organs is a rare (<1%) but a potentially serious side effect which can occur several years after treatment.2
Renal complications after BCG include granulomatous affectation, abscesses, pyelonephritis and interstitial nephritis.3,4 BCG can reach the upper urinary tract by not completely understood mechanism. Hematogenous dissemination and/or direct seeding by vesicoureteral reflux are the proposed mechanisms.
Hematogenous spread as an etiologic mechanism is based in the lower incidence of renal affectation compared to vesicoureteral reflux incidence after TURBT.3 This fact, combined with the described granulomatous affectation in other solid organs, indicates that it can be a result of systemic blood spread.3 In order to decrease the incidence of complications, it has been recommended to delay the BCG treatment after a recent TURBT, macroscopic hematuria, bacterial bladder infection or urologic interventional procedures.1
Therapy with isoniazid and/or rifampicin after the procedure is recommended to prevent systemic side effects.4
Another mechanism by which the kidney is affected is vesicoureteral reflux, which explains the preference for affectation in the upper renal poles.3 According to previous reports, there is a preference for abscess and granuloma formation in the upper renal pole because they tend to be more affected by the reflux.3
Renal granulomas present in imaging as a single or multifocal solid masses, mimicking papillary renal cell carcinoma or parenchymal infiltration by transitional cell carcinoma.5 Renal ultrasound commonly shows an echogenic mass. On contrast-enhanced CT they appear as hypovascular mass compared to surrounding renal parenchyma.1,3 On MRI, they are characteristically hypo to isointense on T1WI with variable signal intensity on T2WI depending on the inflammation and fibrotic component. After contrast, they present low enhancement as on CT.3
The diagnosis of BCG complications requires, theoretically, a positive BCG culture and the presence of granulomas at histopathologic analysis. Urine cultures and fine-needle aspiration can be useful to distinguish bacterial abscesses. However, cultures have a low yield probably due to the attenuated state of the bacilli.
Differentiation of renal granulomas from malignant tumours only by imaging is challenging. In most of the published cases, a definitive diagnosis was established after the pathological examination.
A high degree of suspicion is crucial to include renal granuloma in the differential diagnosis of a kidney mass in this scenario. Renal biopsy should be recommended to avoid unnecessary surgery.
Please cite this article as: Martínez Maicas H, Torregrosa Andrés A. Afectación renal granulomatosa después de tratamiento con BCG de un tumor vesical. Radiología. 2022;64:179–181.

