



Commercial video games are considered an effective tool to improve postural balance in different populations. However, the effectiveness of these video games for patients with multiple sclerosis (MS) is unclear.
ObjectivesTo analyse existing evidence on the effects of commercial video games on postural balance in patients with MS.
Material and methodWe conducted a systematic literature search on 11 databases (Academic-Search Complete, AMED, CENTRAL, CINAHL, WoS, IBECS, LILACS, Pubmed/Medline, Scielo, SPORTDiscus, and Science Direct) using the following terms: “multiple sclerosis”, videogames, “video games”, exergam*, “postural balance”, posturography, “postural control”, balance. Risk of bias was analysed by 2 independent reviewers. We conducted 3 fixed effect meta-analyses and calculated the difference of means (DM) and the 95% confidence interval (95% CI) for the Four Step Square Test, Timed 25-Foot Walk, and Berg Balance Scale (BBS).
ResultsFive randomised controlled trials were included in the qualitative systematic review and 4 in the meta-analysis. We found no significant differences between the video game therapy group and the control group in Four Step Square Test (DM: −.74; 95% CI, −2.79 to 1.32; P=.48; I2=0%) and Timed 25-Foot Walk scores (DM: .15; 95% CI, −1.06 to .76; P=.75; I2=0%). We did observe intergroup differences in BBS scores in favour of video game therapy (DM: 5.30; 95% CI, 3.39–7.21; P<.001; I2=0%), but these were not greater than the minimum detectable change reported in the literature.
ConclusionsThe effectiveness of commercial video game therapy for improving postural balance in patients with MS is limited.
El uso de videojuegos comerciales ha sido considerado una herramienta eficaz para mejorar el equilibrio postural en diferentes poblaciones. Sin embargo, los beneficios reportados en pacientes con esclerosis múltiple (PEM) no están claros.
ObjetivosAnalizar la evidencia existente sobre los efectos de las terapias con videojuegos comerciales en el equilibrio postural en PEM.
Material y métodoSe realizó una búsqueda en las bases de datos Academic-Search-Complete, AMED, CENTRAL, CINAHL, WoS, IBECS, LILACS, Pubmed/Medline, Scielo, SPORTDiscus, ScienceDirect utilizando los términos multiple sclerosis, videogames, video games, exergam*, postural balance, posturography,postural control, balance. El riesgo de sesgo fue analizado por 2 revisores independientes. Se realizaron 3 metaanálisis modelos de efectos fijos calculando la diferencia de medias (DM) y el intervalo de confianza (IC) del 95% para las variables Four-Step-Square-Test, Timed-25-Foot-Walk y Berg-Balance-Scale.
ResultadosCinco ensayos clínicos controlados aleatorizados fueron incluidos en la síntesis cualitativa, mientras que 4 fueron incluidos en el metaanálisis. No se observaron diferencias entre las terapias con videojuegos y los grupos controles para la variable Four-Step-Square-Test (DM: –0,74; IC 95%: –2,79 a 1,32; p=0,48; I2=0%) y Timed-25-Foot-Walk (DM: –0,15; IC 95%: –1,06 a 0,76; p=0,75; I2=0%). Sin embargo, la variable Berg-Balance-Scale mostró diferencias a favor del grupo de videojuegos (DM: 5,30; IC 95%: 3,39 a 7,21; p<0,001; I2=0%), aunque estos resultados no fueron superiores al mínimo cambio detectable reportado en la literatura científica.
ConclusionesLa eficacia de las terapias con videojuegos comerciales sobre el equilibrio postural en PEM es escasa.
Multiple sclerosis (MS) is a chronic, inflammatory demyelinating disease of unknown, probably multifactorial origin. The disease is associated with a wide range of symptoms, including depression, fatigue, pain, muscle weakness, and gait and balance alterations.1 Postural imbalance is one of the most disabling symptoms of MS, affecting approximately 80% of patients.2
Commercial video games constitute a promising tool for improving postural balance in various populations.3–5 They are inexpensive and widely accessible, and increase patient motivation and satisfaction with treatment, which makes them a useful tool both in clinical practice and in the home environment.6 “Exergames” involve such activities as dancing, running, throwing, cycling, boxing, or playing tennis; players use their arms and legs to activate commands in order to accomplish objectives. This stands in contrast with traditional video games, which are usually played in a seated position.7 Despite increasing evidence on the use of exergames in different populations,3–5 their benefits for MS are not clear and further research is required.
This systematic review and meta-analysis aims to analyse the available evidence on the effects of exergames on postural balance in patients with MS.
Material and methodsDesignWe performed a systematic review of randomised controlled clinical trials using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.8
Search strategy and databasesWe performed a literature search on 11 electronic databases: Academic Search Complete, Allied and Complementary Medicine Database (AMED), Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL, Web of Science Core Collection, IBECS, LILACS, PubMed/Medline, Scielo, SPORTDiscus, and ScienceDirect.
We used the following search terms: multiple sclerosis, videogames, video games, exergam*, postural balance, posturography, postural control, and balance. These were combined using the Boolean operators AND and OR. We also reviewed the references cited in the studies identified in the literature search. The last search was conducted on 9 October 2017. Additional information on the search strategy used is provided in the Supplementary Material.
Eligibility criteriaWe gathered randomised controlled clinical trials evaluating the effects of commercial video games on postural balance in patients with MS and published in full-text format in international, peer-reviewed journals. Studies combining video games with other types of therapy were excluded from our review.
Study selection and data collection processStudies were selected by 2 independent reviewers, who first read the titles and abstracts of the studies gathered during the electronic search, and then read the full texts of those articles potentially relevant to our review.
We used the PICO approach8 to gather data on participant characteristics (sample size, age, sex, level of disability), type of intervention (type of exercise; video game used; session intensity, frequency, and duration; duration of the intervention), characteristics of the control group, and impact on postural balance. We also gathered data on study characteristics (author, year of publication) and the tools used by the authors to evaluate balance.
Risk of biasWe assessed the risk of bias of the studies reviewed using the tool recommended by the Cochrane Handbook for Systematic Reviews of Interventions,9 which evaluates sequence generation, allocation sequence concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other potential threats to validity. Two independent reviewers evaluated the risk of bias; disagreements were resolved by a third reviewer.
Statistical analysisA meta-analysis was conducted in cases where 2 or more studies measured the same outcome variable. We calculated the difference in means (DM) and the 95% confidence interval (CI) for each relevant outcome from each of the studies selected. The results of the meta-analysis are presented in the form of forest plots; statistical significance was set at P≤.05. The I2 index was used to assess the heterogeneity of the studies included.
The fixed-effects model was applied when the I2 index detected no significant heterogeneity (P>.05); otherwise, the random-effects model was used. Egger's regression test was used to assess publication bias. A non-zero intercept indicated publication bias (P≤.05).
Statistical analysis was performed with RevMan 5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) and a Microsoft® Excel 2010 template.
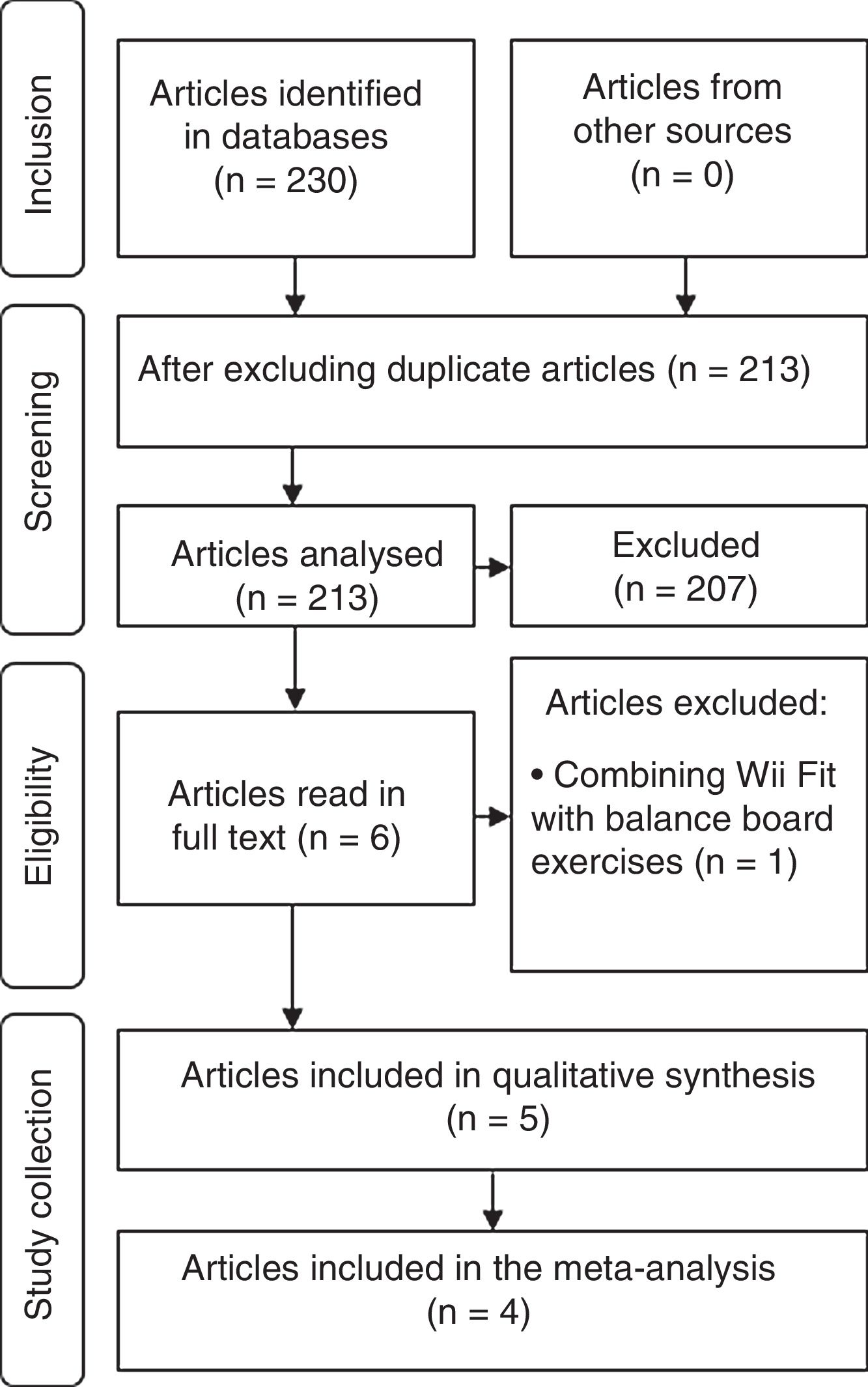
ResultsStudy selectionWe identified a total of 230 studies in the electronic databases used. We excluded duplicate articles and selected 6 potentially eligible studies, which were read in full text format. One of these was excluded as it combined Wii Fit with balance board exercises. Five studies were included in the qualitative analysis, and 4 were selected for the meta-analysis (Fig. 1).
Study characteristics and risk of bias
We included randomised controlled clinical trials published between 2013 and 2015.10–14
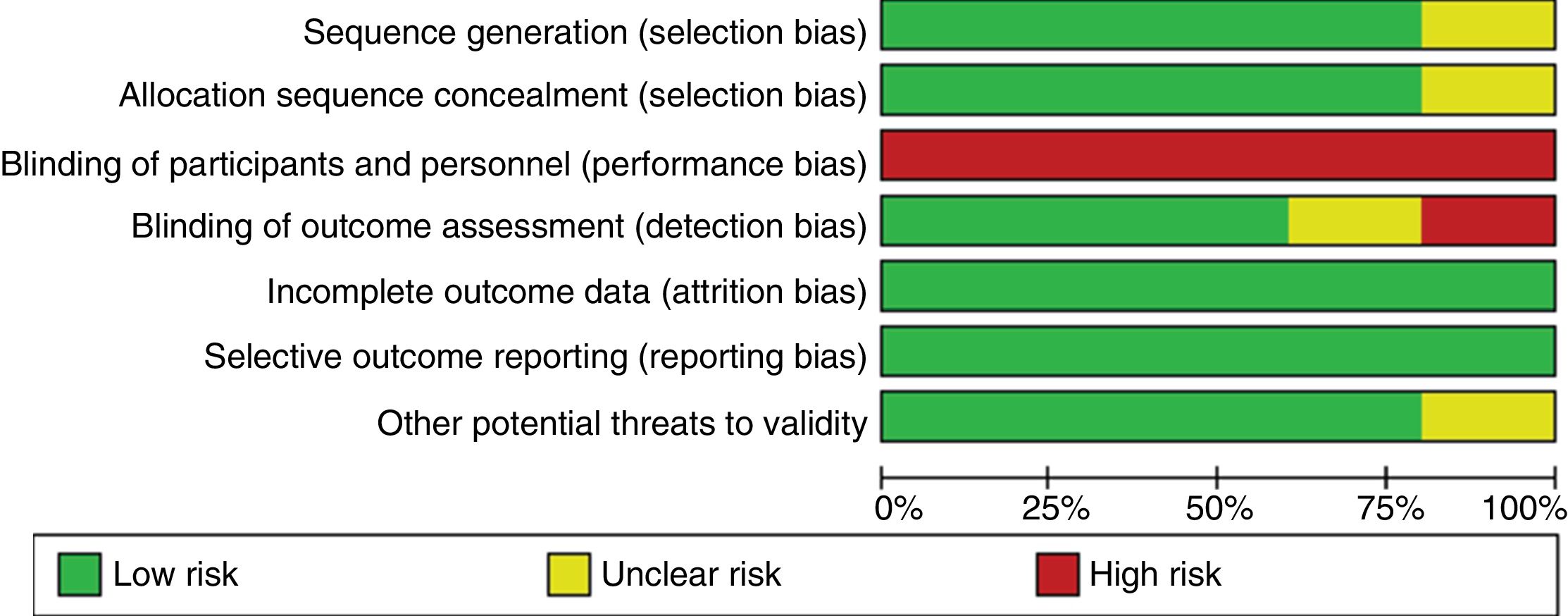
In general terms, the articles included show a low risk of bias for all domains, except for blinding of participants and personnel, which had a high risk of bias (Fig. 2).10–14 Eighty percent of studies showed adequate sequence generation and allocation sequence concealment.10,11,13,14 Assessors were blinded in 60% of studies.10,11,13 The domains “selective outcome reporting” and “incomplete outcome data” presented a low risk of bias in all studies.10–14 Additional information on the risk of bias assessment is provided in the Supplementary Material.
Patient characteristics
A total of 259 patients (176 women, 86 men) with MS and moderate disability (Expanded Disability Status Scale scores 3-6) were included in our systematic review. Patient ages ranged from 35.3 to 53.9 years.
Characteristics of the interventionExperimental groups used different commercial video game systems, including the Nintendo Wii® for the videogames Wii Fit® and Wii Fit Plus®,10,12–14 and the Xbox 360® for the videogames Kinect Sports®, Kinect Joy Ride®, and Kinect Adventures®.11
In some studies, controls received conventional physical therapy with strength, proprioception, and gait exercises, as well as stretching or balance board exercises,10,11,14 whereas in others they received no treatment.12–14
Exergaming training was performed between 2 and 5 times per week, with sessions lasting 30-60minutes; the duration of the intervention ranged from 4 to 12 weeks. Session intensity was adjusted by progressively increasing the game's difficulty level.11–14
Patient assessment toolsDynamic balance was assessed with a wide range of functional tests and scales: the Timed Up and Go test, Cognitive Timed-Up-and-Go dual-task test, Timed Chair Stand test, Four Step Square Test (FSST), Timed 25-Foot Walk (T25-FW), Dynamic Gait Index (DGI), Activities-Specific Balance Confidence Scale, Berg Balance Scale (BBS), and Tinetti Balance and Gait Assessment Scale.10–13 Some authors used stabilometric parameters to assess static balance with the eyes open and closed, including centre of pressure (CoP) displacement, CoP sway area, CoP velocity, and CoP displacement range in the anteroposterior and mediolateral axes.10,13,14
Effects of exergaming on postural balanceThe studies included generally reported improvements in the short term (4 to 12 weeks) in all balance variables analysed in patients receiving exergame therapy as compared to controls receiving no treatment14 or performing strength and proprioception exercises10,11,13 (Table 1).
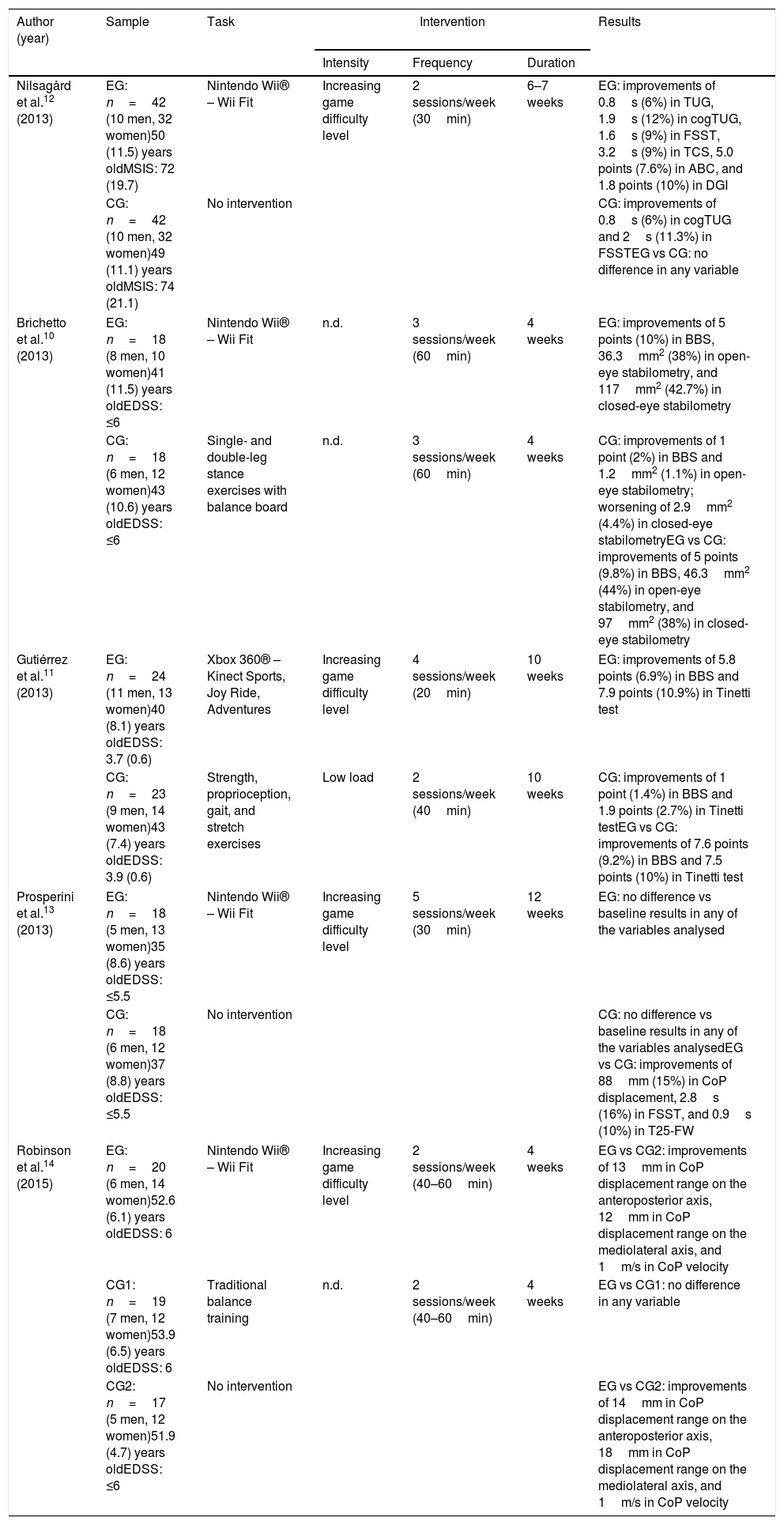
Characteristics of the studies included.
| Author (year) | Sample | Task | Intervention | Results | ||
|---|---|---|---|---|---|---|
| Intensity | Frequency | Duration | ||||
| Nilsagård et al.12 (2013) | EG: n=42 (10 men, 32 women)50 (11.5) years oldMSIS: 72 (19.7) | Nintendo Wii® – Wii Fit | Increasing game difficulty level | 2 sessions/week (30min) | 6–7 weeks | EG: improvements of 0.8s (6%) in TUG, 1.9s (12%) in cogTUG, 1.6s (9%) in FSST, 3.2s (9%) in TCS, 5.0 points (7.6%) in ABC, and 1.8 points (10%) in DGI |
| CG: n=42 (10 men, 32 women)49 (11.1) years oldMSIS: 74 (21.1) | No intervention | CG: improvements of 0.8s (6%) in cogTUG and 2s (11.3%) in FSSTEG vs CG: no difference in any variable | ||||
| Brichetto et al.10 (2013) | EG: n=18 (8 men, 10 women)41 (11.5) years oldEDSS: ≤6 | Nintendo Wii® – Wii Fit | n.d. | 3 sessions/week (60min) | 4 weeks | EG: improvements of 5 points (10%) in BBS, 36.3mm2 (38%) in open-eye stabilometry, and 117mm2 (42.7%) in closed-eye stabilometry |
| CG: n=18 (6 men, 12 women)43 (10.6) years oldEDSS: ≤6 | Single- and double-leg stance exercises with balance board | n.d. | 3 sessions/week (60min) | 4 weeks | CG: improvements of 1 point (2%) in BBS and 1.2mm2 (1.1%) in open-eye stabilometry; worsening of 2.9mm2 (4.4%) in closed-eye stabilometryEG vs CG: improvements of 5 points (9.8%) in BBS, 46.3mm2 (44%) in open-eye stabilometry, and 97mm2 (38%) in closed-eye stabilometry | |
| Gutiérrez et al.11 (2013) | EG: n=24 (11 men, 13 women)40 (8.1) years oldEDSS: 3.7 (0.6) | Xbox 360® – Kinect Sports, Joy Ride, Adventures | Increasing game difficulty level | 4 sessions/week (20min) | 10 weeks | EG: improvements of 5.8 points (6.9%) in BBS and 7.9 points (10.9%) in Tinetti test |
| CG: n=23 (9 men, 14 women)43 (7.4) years oldEDSS: 3.9 (0.6) | Strength, proprioception, gait, and stretch exercises | Low load | 2 sessions/week (40min) | 10 weeks | CG: improvements of 1 point (1.4%) in BBS and 1.9 points (2.7%) in Tinetti testEG vs CG: improvements of 7.6 points (9.2%) in BBS and 7.5 points (10%) in Tinetti test | |
| Prosperini et al.13 (2013) | EG: n=18 (5 men, 13 women)35 (8.6) years oldEDSS: ≤5.5 | Nintendo Wii® – Wii Fit | Increasing game difficulty level | 5 sessions/week (30min) | 12 weeks | EG: no difference vs baseline results in any of the variables analysed |
| CG: n=18 (6 men, 12 women)37 (8.8) years oldEDSS: ≤5.5 | No intervention | CG: no difference vs baseline results in any of the variables analysedEG vs CG: improvements of 88mm (15%) in CoP displacement, 2.8s (16%) in FSST, and 0.9s (10%) in T25-FW | ||||
| Robinson et al.14 (2015) | EG: n=20 (6 men, 14 women)52.6 (6.1) years oldEDSS: 6 | Nintendo Wii® – Wii Fit | Increasing game difficulty level | 2 sessions/week (40–60min) | 4 weeks | EG vs CG2: improvements of 13mm in CoP displacement range on the anteroposterior axis, 12mm in CoP displacement range on the mediolateral axis, and 1m/s in CoP velocity |
| CG1: n=19 (7 men, 12 women)53.9 (6.5) years oldEDSS: 6 | Traditional balance training | n.d. | 2 sessions/week (40–60min) | 4 weeks | EG vs CG1: no difference in any variable | |
| CG2: n=17 (5 men, 12 women)51.9 (4.7) years oldEDSS: ≤6 | No intervention | EG vs CG2: improvements of 14mm in CoP displacement range on the anteroposterior axis, 18mm in CoP displacement range on the mediolateral axis, and 1m/s in CoP velocity | ||||
Data are expressed as means (SD) or number (%).
ABC: Activities-specific Balance Confidence; BBS: Berg Balance Scale; CoP: centre of pressure; DGI: Dynamic Gait Index; EDSS: Expanded Disability Status Scale; FSST: Four Step Square Test; CG: control group; EG: experimental group; MSIS: Multiple Sclerosis Impact Scale; min: minutes; n.d.: no data; TCS: Timed Chair Stands test; T25-FW: Timed 25-Foot Walk test; TUG: Timed Up and Go test; cogTUG: Cognitive Timed-Up-and-Go dual-task test.
Exergaming improved dynamic balance by 9%-16%, as measured with the BBS (+5 to +7.6 points), the Tinetti scale (+7.5 points), the T25-FW (−0.8s), and the FSST (−2.8s).10,11,13 Static balance also improved in terms of CoP displacement (−88mm), CoP velocity (−1m/s), and CoP displacement range in the mediolateral (−12 to −18mm) and anteroposterior axes (−13 to −14mm).13,14 Furthermore, CoP sway area decreased by 44% (−46.3mm2) and 38% (−97mm2) during open-eye and closed-eye stabilometry, respectively.10
Two of the studies included report no differences in any of the variables analysed between the intervention group and controls receiving no treatment12 or traditional balance training (e.g., standing with feet together after perturbations, straight line walking, wobble board).14
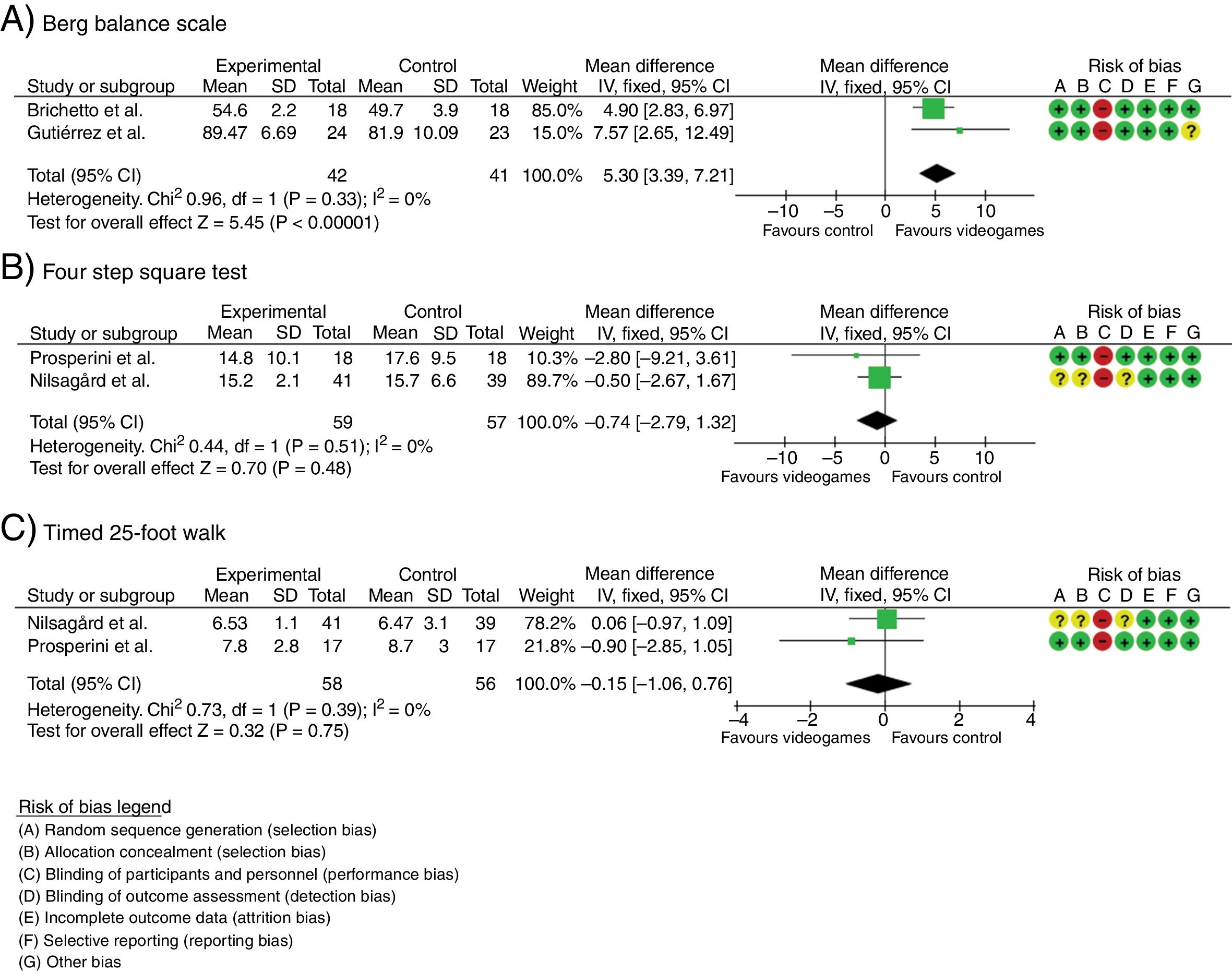
Meta-analysisWe performed 3 meta-analyses to assess the effects of exergaming on BBS, FSST, and T25-FW scores. We used the fixed-effects model, as the heterogeneity analysis revealed no significant differences between studies for any of the variables analysed (BBS: χ2=0.96, P=.33, I2=0%; FSST: χ2=0.44, P=.51, I2=0%; T25-FW: χ2=0.96, P=.33, I2=0%).
Improvements in BBS scores were more marked in patients receiving exergame therapy than in controls performing strength, proprioception, and postural balance exercises (DM: 5.30; 95% CI, 3.39-7.21; P<.001; Fig. 3A). However, no significant differences were observed between patients in the intervention group and controls receiving no treatment in FSST (DM: −0.74; 95% CI, −2.79 to 1.32; P=.48; Fig. 3B) or T25-FW scores (DM: −0.15; 95% CI, −1.06 to 0.76; P=.75; Fig. 3C).
, the Four Step Square Test (B), and the Timed 25-Foot Walk (C). 95% CI: 95% confidence interval; df: degrees of freedom; IV: inverse variance; SD: standard deviation.")
Egger's regression test showed no significant differences between studies for any of the variables analysed (P>.10), which points to an absence of publication bias; we should nonetheless bear in mind that our study analysed a small sample of articles.
DiscussionOur systematic review and meta-analysis analysed the available evidence on the impact of exergames on postural balance in patients with MS.
In the studies analysed, FSST and T25-FW scores and CoP displacement, velocity, and displacement range improved in patients using exergames as compared to those receiving no treatment.13,14 Exergame therapy also achieved more marked improvements in BBS and Tinetti scale scores and in CoP sway area with open and closed eyes than conventional therapy with proprioceptive, strength, and stretching exercises.10,11
However, the magnitude of change for FSST and T25-FW scores (+2.8s and +0.9s, respectively) was below the minimal detectable change (MDC) reported in the literature for patients with MS (4.6s and 12.6s, respectively)15,16; MDC refers to the smallest amount of change required to distinguish a true change after an intervention from a change due to variability or measurement error.17 Furthermore, meta-analysis detected no intergroup differences in any of the variables analysed except for BBS scores, with a magnitude of change of +5.3points in the exergame therapy group; this is below the MDC reported in the literature for this variable in patients with MS (7 points).15 Our results suggest that the magnitude of change for each variable cannot be interpreted as a true change in patients’ clinical status but rather is due to variability in the assessment tool. To our knowledge, the MDC for Tinetti scale scores and static stabilometry variables has not been established for patients with MS; our results for these variables should therefore be interpreted with caution.
Future studies should use assessment tools whose sensitivity to change has been analysed in patients with MS, in order to be able to determine whether changes are attributable to the intervention or to measurement errors.
LimitationsDespite rigorous data collection and analysis, our study is not without limitations. Despite increasing interest in treatment with commercially available exergames for balance training in patients with MS, few studies have analysed the effects of this type of intervention.10–14 In any case, the studies analysed show a low risk of bias for most domains.
This review identifies methodological issues that may be accounted for in future research into the effects of exergame therapy on postural balance in patients with MS.
ConclusionsFew data are available on the effectiveness of commercial exergames on postural balance in patients with MS. Future studies should use appropriate assessment tools to analyse the effects of this type of intervention on postural balance in MS before it can be recommended in clinical practice.
Conflicts of interestThe authors have no conflicts of interest to declare.
The following are the supplementary data to this article:
Please cite this article as: Parra-Moreno M, Rodríguez-Juan JJ, Ruiz-Cárdenas JD. Efectos de la terapia con videojuegos comerciales sobre el equilibrio postural en pacientes con esclerosis múltiple: revisión sistemática y metaanálisis de ensayos clínicos controlados aleatorizados. Neurología. 2019. https://doi.org/10.1016/j.nrl.2017.12.001
