


Introduction: Surgical treatment is the treatment of choice for the management of incomplete abortion. Uterine curettage is a procedure widely used; manual vacuum aspiration is another safe therapeutic option. Long-term complications of these methods are intrauterine adhesions and adenomyosis. This has been linked to abnormal uterine bleeding, and probably is the most frequent indication for a hysterectomy. Objective of this study is to determine if there is a relationship between surgical methods of treatment for incomplete abortion and the prevalence of adenomyosis in patients subject to a hysterectomy.
Material and methods: This is a retrospective, comparative cohort study. We reviewed medical records of patients who underwent a hysterectomy between 2007 and 2009. We evaluated age at the time of hysterectomy, preoperative diagnosis, number of pregnancies, cesarean sections, abortions, curettage and uterine evacuation by manual vacuum aspiration. Pathology reports were reviewed to document adenomyosis. Statistical analysis was made with chi square.
Results: From 794 patients who underwent a hysterectomy, we included 211 patients with incomplete abortions history. Uterine curettage was performed in 102 patients, manual vacuum aspiration in 92, and both procedures in 17. No differences were found in pre-operatory diagnoses, age, births, cesarean sections and abortions. We found adenomyosis in 15.6, 4.3 and 5.8% of patients respectively (p<0 .01)
Conclusions: Manual vacuum aspiration is associated with less trauma of the uterine cavity than uterine curettage for the management of incomplete abortion. We recommend manual vacuum aspiration as the method of choice for the management of incomplete abortion.
Introducción: El legrado uterino instrumentado y la aspiración manual endouterina son procedimientos utilizados en el tratamiento del aborto incompleto. Las complicaciones a largo plazo de estos métodos, incluyen formación de adherencias intrauterinas y la adenomiosis. Esta última se ha asociado con sangrado uterino anormal, y esto con una mayor incidencia de histerectomías. El objetivo del presente estudio es deter-minar si existe una relación entre los métodos de tratamiento quirúrgico del aborto incompleto, y la prevalencia de adenomiosis en pacientes sometidas a histerectomía.
Material y métodos: El presente es un estudio retrospectivo, comparativo de cohortes. Se revisaron los expedientes de pacientes sometidas a histerectomía entre 2007 y 2009. Se evaluaron: edad, diagnóstico preoperatorio, número de embarazos, cesáreas, abortos, legrados instrumentados y aspiraciones manuales endouterinas. Se revisaron los reportes de patología para documentar adenomiosis. El análisis estadístico se realizó con ji cuadrada.
Resultados: De 794 pacientes que se sometieron a histerectomía, se encontraron 211 pacientes con historia de aborto incompleto. De estas, 102 pacientes tenían historia de legrado uterino, 92 de aspiración manual endouterina y 17 de ambos procedimientos. No se encontraron diferencias entre los diagnósticos preoperatorios, edad, número de partos, cesáreas y abortos. La prevalencia de adenomiosis fue de 15.6, 4.3 y 5.8%, respectivamente (p<0.01).
Conclusiones: La aspiración manual endouterina se asocia con un menor trauma de la cavidad uterina, que el legrado uterino para el tratamiento del aborto incompleto. Se recomienda la aspiración manual endouterina, como el método de elección para el manejo quirúrgico del aborto incompleto.
Introduction
Spontaneous abortion is defined as spontaneous termination of pregnancy before the 20th week, counted from the first day of the last menstrual period, or an infant born with a birth weight less than 500 g. This complication occurs approximately in 15% of all pregnancies.1
Treatment of spontaneous abortion may be medical, surgical or expectant.2 Medical treatment and expectant management have been recently reported as therapeutic alternatives. Both options have been linked to a lower rate of complications.3 However, these strategies require a major health infrastructure to ensure the immediate availability of health resources for patients undergoing these therapeutic approaches. Unfortunately, not all patients have access to these resources.
Surgical treatment is the treatment of choice for the management of incomplete abortion. The instrumental uterine curettage (D&C) is a procedure widely used for this purpose around the world. It consists in removing the contents of the uterus mechanically with sharp devices.This procedure is performed under general or regional anesthesia.4
Manual vacuum aspiration (MVA) is a safe option for the treatment of incomplete abortion.5 This procedure is performed more frequently, however, still a large number of physicians prefer to use the traditional method of uterine curettage. The reasons for this attitude include lack of knowledge of the technique, lack of appropriate equipment, and distrust in the effectiveness of the procedure.6
One complication, often associated with surgical management of incomplete abortion, is the formation of intrauterine adhesions. These are linked to damage of the basement membrane of the endometrium in a pregnant uterus, just when it is more vulnerable.7 The consequences of this complication on fertility are yet to be defined.8 Other uterine pathology also associated with trauma of the basal layer of the endometrium is adenomyosis. Even without a universally accepted clinical picture, adenomyosis has been linked to, among other symptoms, with a high incidence of abnormal uterine bleeding.9 Abnormal uterine bleeding is probably the most frequent indication for a hysterectomy.
The objective of this study is to determine if there is a relationship between surgical methods of treatment of incomplete abortion (instrumental uterine curettage and manual vacuum aspiration) and the prevalence of adenomyosis in patients subjected to a hysterectomy for benign disease.
Material and methods
This is a retrospective, comparative cohort study; conducted at the "Dr. José E. González" University Hospital of Universidad Autónoma de Nuevo León in Monterrey, Mexico between the years 2010 and 2011. With prior approval of the Ethics Committee of our institution, we reviewed medical records of patients who underwent a hysterectomy between January 2007 and December 2009. Patients were contacted by telephone, e-mail or telegram to request their consent to participate in this study.
We evaluated age at the time of the hysterectomy, preoperative diagnosis, and number of pregnancies, cesarean sections, abortions, curettage and uterine evacuation by manual vacuum aspiration. Finally, the pathology report was revised to document adenomyosis.
Statistical analysis was performed using chi square test. We used the statistical package SPSS version 16 for MAC.
Results
We reviewed medical records of 794 patients who underwent hysterectomy during the period between January 2007 and December 2009. We detected 211 patients with a history of uterine curettage, manual vacuum aspiration or both procedures. The most common preoperative diagnoses for hysterectomy were abnormal uterine bleeding, uterine myoma and pelvic relaxation. The average age of patients was 43.9 years old, with a standard deviation ± 9.76.
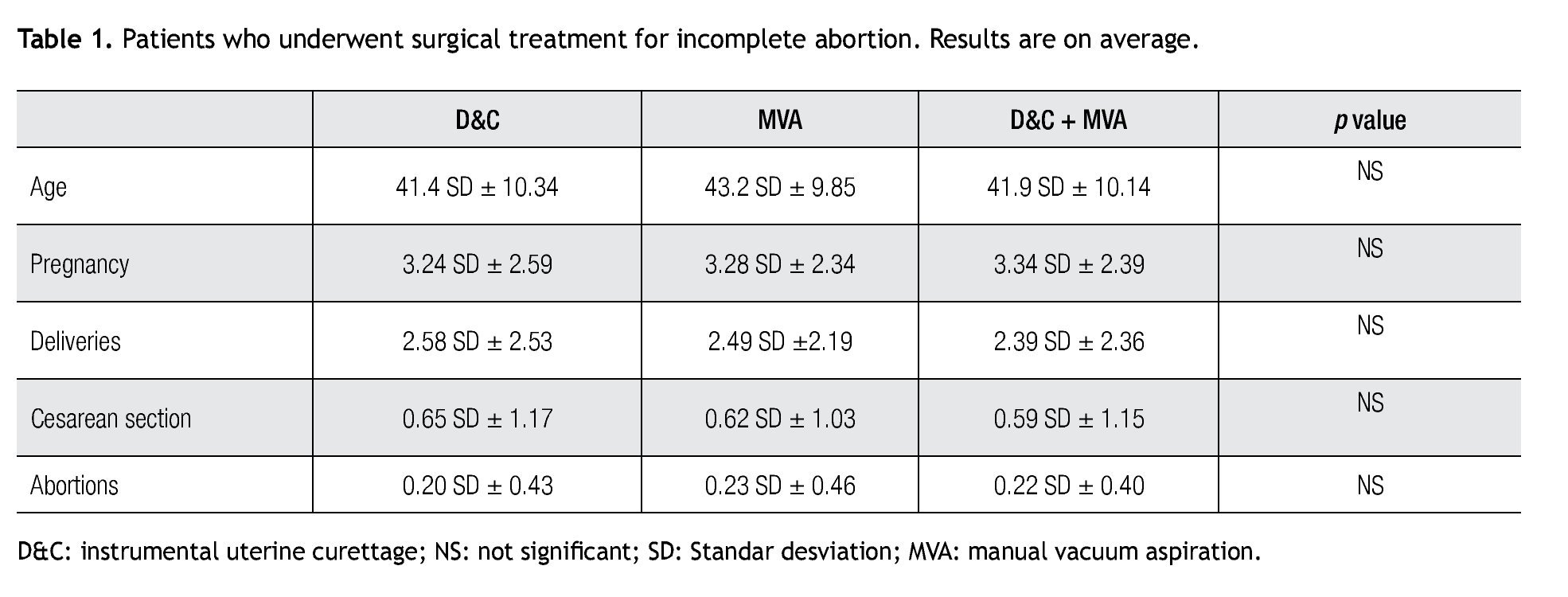
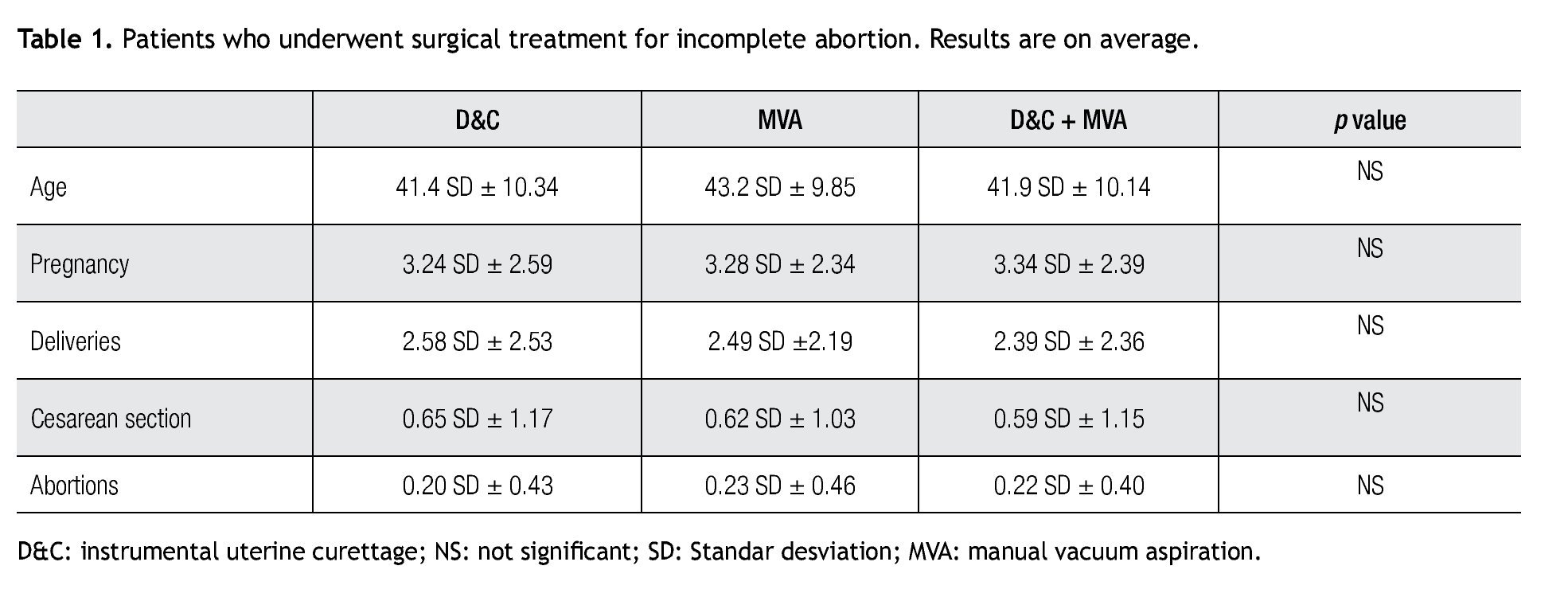
The number of pregnancies in the overall group was, on average, 3.6 with a standard deviation of ± 2.37. The number of births was in average 2.70 with a standard deviation of ± 2.44. The number of caesarean sections was 0.69 average with a standard deviation of ±1.12 and the number of abortions was on average of 0.25 with a standard deviation of ± 0.56. Uterine curettage was performed in 102 patients; manual vacuum aspiration in 92 patients, and in 17 patients both procedures had been made.
The preoperative diagnoses when patients were scheduled for hysterectomy were similar regardless of a history of uterine curettage, manual vacuum aspiration or both procedures. These preoperative diagnoses were in patients with history of uterine curettage: abnormal uterine bleeding in 46.0% (47/102), uterine myoma in a 34.3% (35/102), and pelvic relaxation in 9.8% (10/107). Similarly, in patients with a history of manual vacuum aspiration the most frequent diagnoses were: abnormal uterine bleeding in 44.5% (41/92), uterine myoma in 36.9% (34/92), and pelvic relaxation in the 8.6% (8/92). Other less frequent preoperative diagnoses were: low degree intra epithelial lesion, endometrial hyperplasia, severe pelvic inflammatory disease and adnexal mass. The frequency of these diagnoses was similar regardless of the procedure performed.
Upon comparing the results for age, number of pregnancies, births, caesarean sections and abortions in patients with a history of uterine curettage, manual vacuum aspirations or both procedures, no statistically significant differences were found. The results are shown in Table 1.
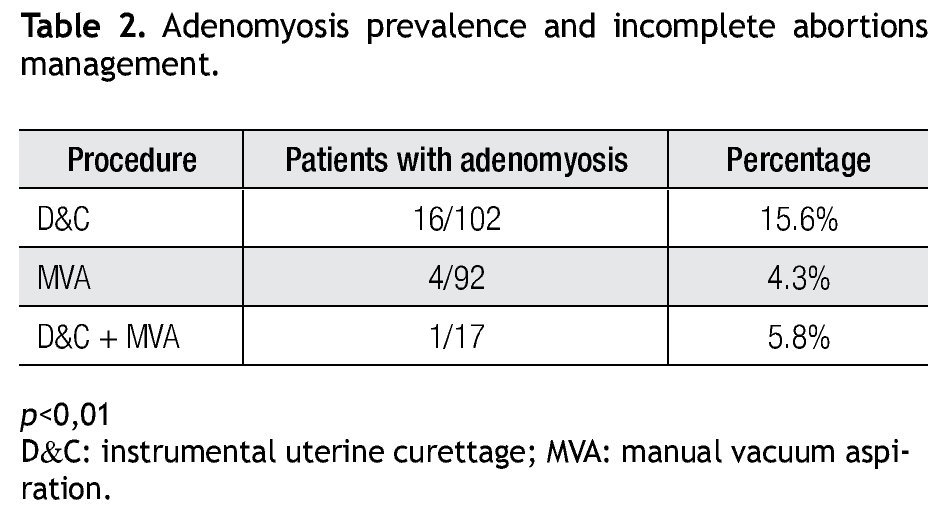
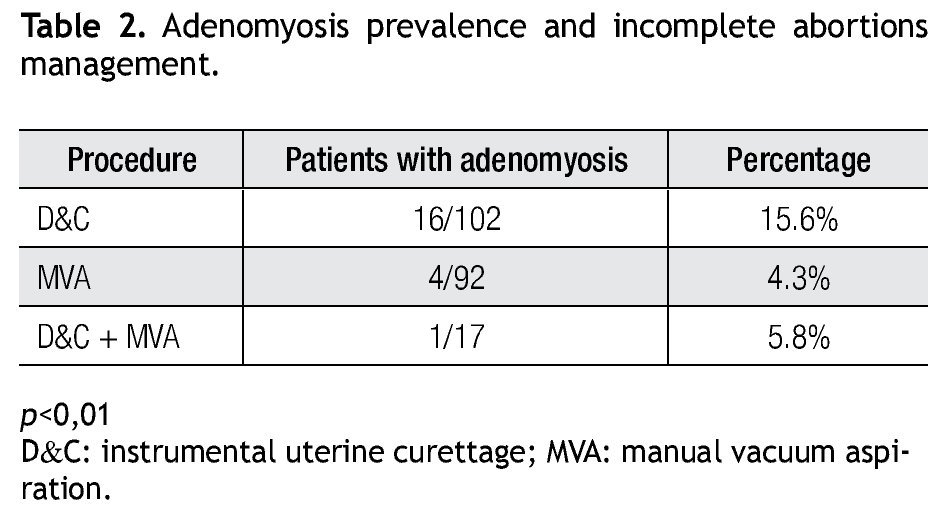
The prevalence of adenomyosis in patients with history of uterine curettage was 15.6% (16/102). On the other hand, in patients with history of manual vacuum aspiration the adenomyosis prevalence was 4.3% (4/92). The prevalence of adenomyosis in patients with history of both procedures was 5.8% (1/17). The difference was statistically significant (p<0.01) (Table 2).
Discussion
Adenomyosis is a benign condition that is defined as the presence of endometrial glands and stroma in the thickness of the myometrium.10
Many aspects of this disease are still controversial. However, it has been accepted than adenomyosis occurs due to the rupture of the basement membrane of the endometrium, producing an invasion of endometrial glands and stroma towards the interior of the myometrium.11
A related factor associated with the development of adenomyosis is uterine trauma.12,13 Uterine manipulation during uterine surgery, such as uterine curettage or myomectomy, has been previously associated with adenomyosis.9 Perhaps, injury caused during a uterine curettage could affect the endometrial basal membra- ne and facilitate the invasion of endometrial glands into the myometrium. It is important to note that in the study we found that the prevalence of adenomyosis was three times greater in patients who underwent uterine curettage when compared with patients who underwent manual vacuum aspiration for treatment of incomplete abortion. Increased uterine trauma, caused by sharp instruments used during uterine curettage, could probably be responsible for the increase in the prevalence of adenomyosis in these patients.
Considering that gestational loss in the first trimester of pregnancy oscillates around 15%,1 we can easily understand the importance of selecting the more effective and less traumatic way for the management of incomplete abortions. In this sense, manual vacuum aspiration has been described as a safe, effective and low cost strategy for incomplete abortion treatment.14
Manual vacuum aspiration can be made on an outpatient basis, with a lower rate of complications during the procedure than uterine curettage and with a lower rate of long-term complications.
This last is transcendental, the resulting aftermath of therapeutic strategies for the management of incomplete abortion include the formation of intrauterine adhesions2 and the development of adenomyosis.9 The importance of these consequences is that intrauterine adhesions have been linked with infertility.2 Likewise, adenomyosis has been linked with an increased incidence of abnormal uterine bleeding,15 a condition which, as it was previously commented, is one of the more frequent indications for hysterectomy.
In conclusion, with these results we can say that the use of manual vacuum aspiration is associated with less trauma of the uterine cavity than uterine curettage for the management of incomplete abortion. Thus, it can be associated with a lower number of long-term complications. Also considering the previously described benefits of this technique, we can recommend manual vacuum aspiration as the method of choice for management of incomplete abortions.
Received: October 2011. Accepted: March 2012
Corresponding autor:
Luis Humberto Sordia Hernández,
MD. Madero y Gonzalitos S/N,
Colonia Mitras Centro.
Z.P. 64400. Monterrey N.L. México.
E-mail:lsordia@prodigy.net.mx