


The aim of the study was to determine the somatotype of Mexican type 2 diabetes patients, using the Heath and Carter somatotype method.
MethodsThe study was conducted on 180 subjects, who underwent an anthropometry following the restricted format established by the International Society for the Advancement of Kinanthropometry (ISAK). A database was elaborated and we obtained descriptive measures such as age, weight, height and the 3 somatotype components.
ResultsThe average age was 58 years (±11 SD); 58.6 years (±10.9 SD) for males and 56.8 years (±11 SD) for females. The average weight was 77.5kg (±16.7); 80.7kg (±14.6 SD) for males and 75kg (±17.8 SD) for females. The results indicate that the mean somatotype for Mexican type 2 diabetes patients was 6.3, 6.4, 0.6. Diabetic females have higher mean values for endomorphy (7.3) and mesomorphy (6.7) and lower mean values for ectomorphy (0.4) than their male counterparts (5.0, 6.0 and 0.8, respectively). It is evident that endomorphy is predominantly in females, in contrast to males, since there are known differences in fat and muscular mass between both genders.
ConclusionsThe results are similar to previous studies presented for other diabetic populations. Sex differences are significant and especially higher for the endomorphic component, with generally higher values in females. It is important to continue this research direction with bigger samples and the study of other risk factors that directly affect the somatotype of type 2 diabetes.
Diabetes mellitus is a global health problem, as well as the most well-known disorder for centuries. However, the knowledge of its etiology, natural history and epidemiology remain incomplete.1–2 The worldwide prevalence of diabetes mellitus has increased exponentially. In the last three decades, the number of people with type 2 diabetes has doubled.3 Despite being an elderly related disease, in the last few years the number of young people diagnosed with the disease is on the rise. Within its pathophysiology, the genetic component is of great importance in diabetes mellitus; nevertheless, it has been linked to obesity and scarce physical activity or a sedentary lifestyle.4
Mexico has suffered the fastest changes ever recorded in the history of food and diet patterns and physical activities resulting in obesity. Diabetes plays a major role, being responsible for almost 14% of all deaths. The increasing prevalence of obesity in children and adults, in addition to the metabolic syndrome, suggests that the situation could have a greater impact in the next few years.5 The National Health and Nutrition Survey of 2012 estimated that 9.2% of Mexican adults had already been diagnosed with diabetes mellitus. This reflects an important increase in comparison to the observed results in 2000, where the rate was 5.8%, and 2006, with 7%.6
The somatotype is a method used to evaluate, study and comprehend body shape and composition in terms of bone, muscle and fatty tissue dimensions.7 First described by Sheldon et al. in 1940, later modified by Heath and Carter in 1967, it was defined as the expression of the current typology of the individual.8,9 The first component, endomorphy, refers to the relative fat and thinness. The second component, mesomorphy, refers to the relative musculoskeletal development by size unit. And the third component, ectomorphy, refers to the relative linear aspect, based mostly on the size/weight ratio. Ectomorphy assesses the form and degree of longitudinal distribution of the first and second component.7,8
An important and visually useful tool, individually and for averages, is the somatochart. This should be used on a more routine basis. It is the graphic representation of a two-dimensional format which uses X and Y coordinates from the obtained measurements. The way a somatochart is distributed for a sample provides useful information and should be accompanied by a statistical analysis. The relationship between the somatotype and different diseases was first described by Sheldon et al. in 1940. In 2002, Koleva et al. evaluated the relationship between the somatotype and its main components with the prevalence of several chronic diseases. In five groups of patients, the prevalence was significantly linked to the somatotype.10
Type 2 diabetes mellitus is a metabolic disorder, and as such it affects the patients’ body composition elements. The changes that the disease induces in patients complement its anthropological characteristics. In fact, it is well-known that obesity has a strong positive connection with the development of diabetes mellitus.2,11 Tafeit et al. utilized optical equipment (lipometer) to perform subcutaneous fatty tissue measurements in different parts of the body on patients with type 2 diabetes as well as in a control group. They documented a higher fat percentage in the upper limbs than in the lower limbs, in both male and female.12
Several studies have made determinations of the somatotype in patients with type 2 diabetes. In 2013, Baltadijev determined the average somatotype in diabetic Bulgarian women between 40 and 60 years old; observing a mesomorph–endomorph somatotype, differing from the mesomorphic somatotype of the control group. Endomorphy and mesomorphy significantly predominated, while ectomorphy was significantly lower.13,14 He also observed and determined the somatotype of the male counterpart within the same age interval and those who presented an endomorph–mesomorph somatotype. Mesomorphy was greater, followed by endomorphy. Ectomorphy was also substantially lower.11
Currently, there are no papers where the somatotype of patients with type 2 diabetes has been established, specifically in the Mexican population. Therefore, the objective of this study was to establish the somatotype of patients with type 2 diabetes of the “Dr. José Eleuterio González” University Hospital in Monterrey, Nuevo León, Mexico, in order to have a phenotype for this type of population and begin a new line of research.
MethodsThis study was conducted at the “Dr. José Eleuterio González” University Hospital in Monterrey, Nuevo León, Mexico. The subjects were Mexican patients with a previous diagnosis of type 2 diabetes mellitus selected from the Out Patients Clinics of Internal Medicine, General Medicine, Endocrinology, and Sport Medicine and Rehabilitation wards during the months of December 2013 through April 2014. The patients needed to be willing to have the necessary measurements taken to establish their somatotype. The exclusion criteria were conditions or complications which could alter body composition such as: lower limb edema, amputations or pregnancy. Additionally, other exclusion criteria were situations or conditions which limited their ability to stand up, such as fractures or recent surgeries.
The study included 180 subjects with type 2 diabetes, previously diagnosed. All subjects underwent an anthropometry, under the restrained profile established by the International Society for the Advancement of Kinanthropometry (ISAK).
The ISAK restrained anthropometry profile consists of the taking of base measurements (weight and size), skin folds (triceps, biceps, subscapular, iliac crest, supraspinal, abdominal, anterior thigh, and medial calf), circumferences (relaxed arm, flexed arm, waist, hips and calves) and diameters (biepicondylar humerus and femur breadth). Regarding skinfolds, circumferences and diameters, these were obtained from the subject's right hemibody as established by ISAK as a standardization method. All measurements were taken by the same measurer in order to avoid variability. Furthermore, in order to reduce variability, the measurer was Level I ISAK certified.
Different equipment was necessary to obtain anthropometric measurements: Fat analyzer TANITA (model TBF-305), to determine weight, and a SECA wall-mounted measuring tape (model 206) to determine size. A body marker to establish reference points, and a Lufkin metallic tape (model W696PM) for circumferences. A CESCORF sliding anthropometer (INNOVARE 16cm) and a Slim Guide plicometer (constant pressure 10gr/mm2) were used to obtain bone diameters and skin folds, respectively.
Once the anthropometry measurements were collected, the following mathematical equations were made to obtain the three components of the somatotype:
ENDOMORPHY: −0.7182+0.1451(x)−0.00068(x2)+0.0000014(x3), where x is the sum of the folds (triceps, subscapular and supraspinal) multiplied by (70.18/size in cm).
MESOMORPHY: (0.858×H)+(0.601×F)+(0.188×B)+(0.161×P)−(0.131×E)+4.5, where H is the biepicondylar humerus breadth, F is the biepicondylar femur breadth, B is the perimeter of the contracted arm, P is the medial calf perimeter and E is height.
ECTOMORPHY: in order to obtain this parameter there are 3 formulas based on the weight index, which is the result of the following formula WI=SizeWeighta
If WI is ≥40.75 then the formula will be: 0.732×WI−28.58
If WI is <40.75 but >38.25 then the formula will be: 0.463×WI−17.63
If WI is ≤38.25 the value the given value will be 0.1.
With the obtained results we created a database using Microsoft Excel 2013. This database was imported to SPSS 21.0. Before conducting the statistical analysis, we analyzed the data in order to obtain implausible values or errors; abnormality and normality indexes were evaluated. A descriptive statistical analysis was conducted where frequencies and proportions were reported according to age, size, weight and the three somatotype components.
Mean values with t-distribution comparison tests were performed where normality could be assumed, with a statistical significance of 95%. When normality could not be assumed, medians comparison tests were performed.
ResultsOut of the 180 subjects who underwent an anthropometry, 2 subjects were eliminated, being detected as atypical cases. This way, we could obtain a normalized sample and avoid skewed results. Out of the 178 remaining, 77 were males and 101 were females. The mean age was: 57.6 years old (±11 SD); 58.6 for males and 56.8 for females. The mean weight was 77.5kg (±16.7 SD) where males weighted 80.7kg (±14.6 SD) and females 75kg (±17.8 SD).
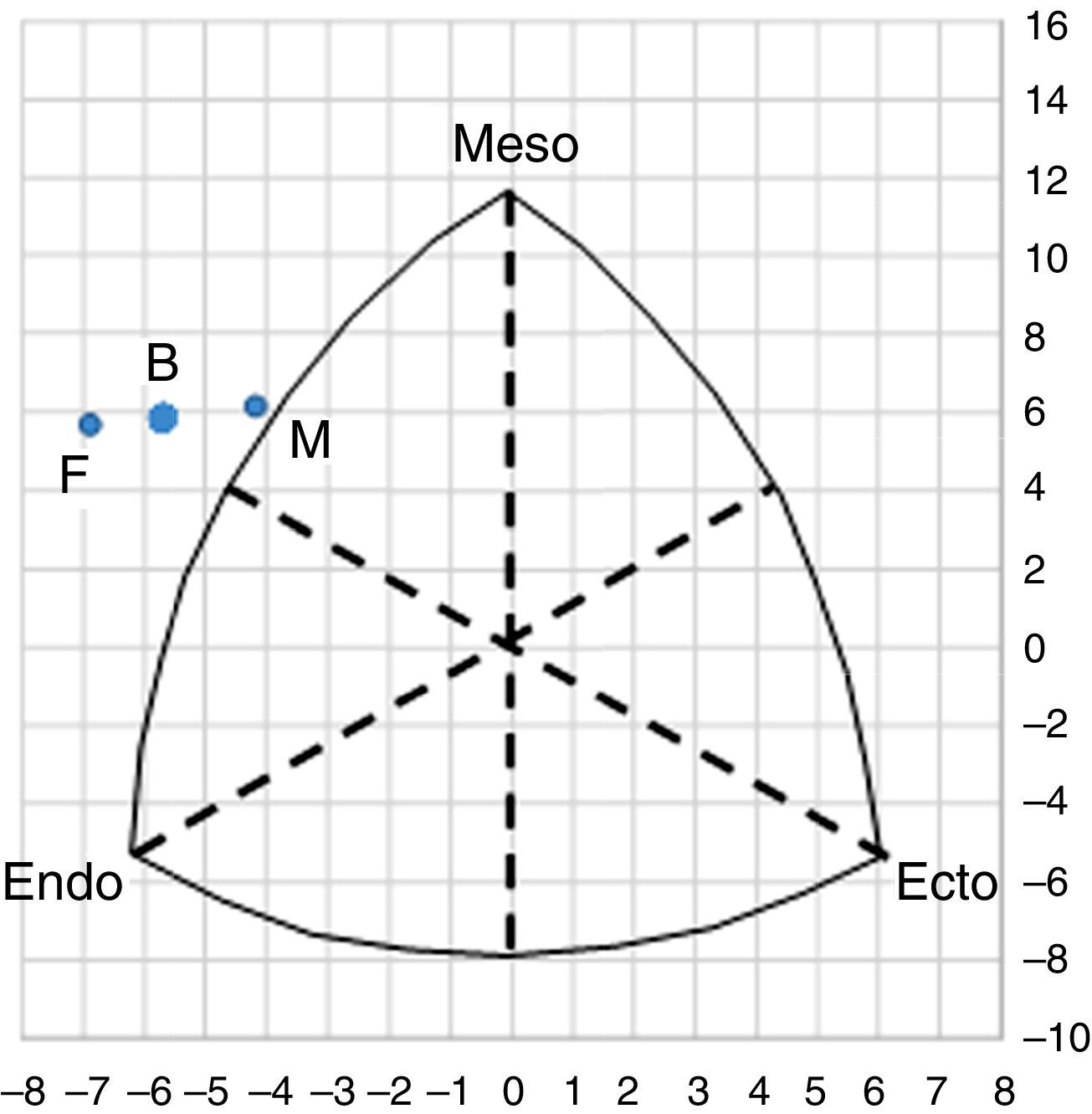
From the collected data, we were able to observe an average somatotype for patients with type 2 diabetes of 6.3-6.4-0.6, which corresponds to an endomorph–mesomorph somatotype. The somatotype for females was 7.3-6.7-0.4, corresponding to a mesomorph–endomorph somatotype; while for males, it was 5.0-6.0-0.8, corresponding to an endomorphic–mesomorph somatotype (see Table 1). According to these results, we are able to say that in this population of patients with type 2 diabetes, the endomorphic and mesomorphic components were dominant while the ectomorphic component was significantly lower. Relative fat was predominant in females, while the muscular component was predominant in males. In both groups the relative linearity was lower.
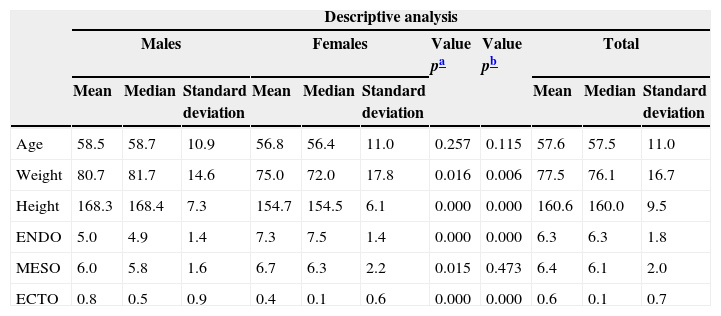
Descriptive analysis of anthropometric measurements of patients with type 2 diabetes at the “Dr. José Eleuterio Gonzàlez” University Hospital, 2014.
| Descriptive analysis | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | Value pa | Value pb | Total | |||||||
| Mean | Median | Standard deviation | Mean | Median | Standard deviation | Mean | Median | Standard deviation | |||
| Age | 58.5 | 58.7 | 10.9 | 56.8 | 56.4 | 11.0 | 0.257 | 0.115 | 57.6 | 57.5 | 11.0 |
| Weight | 80.7 | 81.7 | 14.6 | 75.0 | 72.0 | 17.8 | 0.016 | 0.006 | 77.5 | 76.1 | 16.7 |
| Height | 168.3 | 168.4 | 7.3 | 154.7 | 154.5 | 6.1 | 0.000 | 0.000 | 160.6 | 160.0 | 9.5 |
| ENDO | 5.0 | 4.9 | 1.4 | 7.3 | 7.5 | 1.4 | 0.000 | 0.000 | 6.3 | 6.3 | 1.8 |
| MESO | 6.0 | 5.8 | 1.6 | 6.7 | 6.3 | 2.2 | 0.015 | 0.473 | 6.4 | 6.1 | 2.0 |
| ECTO | 0.8 | 0.5 | 0.9 | 0.4 | 0.1 | 0.6 | 0.000 | 0.000 | 0.6 | 0.1 | 0.7 |
In the somatogram we are able to see where the somatotypes are represented and offer an overview of the dominance of each component explained earlier (See Fig. 1).
Discussion
Body composition and its evaluation can be performed through the somatotype. There is scarce literature on the characteristics of the somatotype of patients with type 2 diabetes and almost none offering data on the Mexican population.13
Buffa et al., conducted an analysis on an Italian population of patients with type 2 diabetes using the same Heath-Carter method.15,16 Fredman et al., also evaluated the somatotype of Tamil Indians with type 2 diabetes, who presented a somatotype with a predominant mesomorphic component compared to healthy individuals.17
There was a great development of the mesomorphic component in both groups for diabetic patients, male and female, as observed in previously mentioned literature.13,14 In this study, patients with type 2 diabetes were characterized by certain peculiarities regarding somatotype. Patients with type 2 diabetes presented a similar predominance to the endomorphic and mesomorphic components, while the ectomorphic component was significantly lower. The differences between genders are significant, and are especially high for the endomorphic component, which has higher values in females, as proven in previous researches.15,17
The somatotype can be considered a useful tool to evaluate the physical and health status of sick subjects, patients with diabetes being one of these study groups. Additionally, it can be used to develop intervention programs in these populations.
Contrary to other anthropometric measurements, like the body mass index (BMI) and waist–hip ratio (WHR), the somatotype can help us evaluate the patient's body composition in a more precise way and be able to link it to its health risks, in addition to working as a follow-up and control tool.
It is important to continue with this line of research and with the study of other risk factors that may directly affect type 2 diabetes physiopathology and which directly affect these patients’ somatotype.
FundingNo financial support was provided.
Conflict of interestThe authors have no conflicts of interest to declare.