



The 2019 coronavirus disease (COVID-19) has caused an unprecedented pandemic. In Spain, it led to a mandatory confinement between March 23rd and June 21st of 2020, causing a stall or cessation of the usual healthcare activity, particularly in the form of the cancellation or delay of medical consultations, diagnostic testing, and non-essential surgical procedures.1
In the case of cancer patients, both diagnosed or currently undergoing diagnostic procedures, many centers opted to limit in-person consultations, avoid endoscopic and surgical testing,2 and individualize studies based on the patients’ risk. In this regard, a decrease in both the diagnoses of all types of cancers, including lung cancer,3 and the number of new cancer diagnoses, owing to the reduced number of visits to lung cancer screening clinics and lung biopsies,4 has been described in relation to the pandemic. On the other hand, an increase in overall cancer mortality due to diagnostic delays caused by the pandemic has also been reported,5 in addition to the fact that even short delays in treatment initiation can have a significant impact on the survival of cancer patients.1
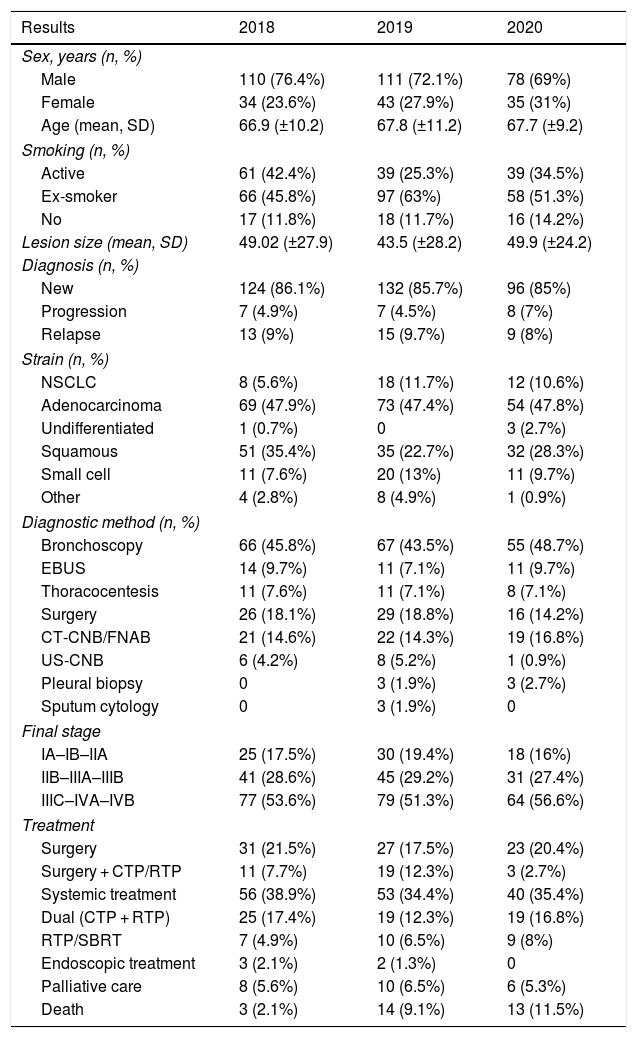
To determine the situation in this regard at our own center, we carried out a retrospective, observational study to analyze lung cancer diagnoses after the confinement period in a referral University Hospital, as well as the diagnostic methods, oncological stage, and time elapsed until the first treatment. To this end, lung cancer diagnoses were recorded between the months of May and October 2020 and compared with those reached during those same months in 2019 and 2018. The characteristics of the patients and their tumors, as well as the diagnostic process, final oncological stage, treatment received, and time elapsed between the first diagnostic test and the first treatment were reviewed. Data on all these variables are shown in Table 1 below.
Results.
| Results | 2018 | 2019 | 2020 |
|---|---|---|---|
| Sex, years (n, %) | |||
| Male | 110 (76.4%) | 111 (72.1%) | 78 (69%) |
| Female | 34 (23.6%) | 43 (27.9%) | 35 (31%) |
| Age (mean, SD) | 66.9 (±10.2) | 67.8 (±11.2) | 67.7 (±9.2) |
| Smoking (n, %) | |||
| Active | 61 (42.4%) | 39 (25.3%) | 39 (34.5%) |
| Ex-smoker | 66 (45.8%) | 97 (63%) | 58 (51.3%) |
| No | 17 (11.8%) | 18 (11.7%) | 16 (14.2%) |
| Lesion size (mean, SD) | 49.02 (±27.9) | 43.5 (±28.2) | 49.9 (±24.2) |
| Diagnosis (n, %) | |||
| New | 124 (86.1%) | 132 (85.7%) | 96 (85%) |
| Progression | 7 (4.9%) | 7 (4.5%) | 8 (7%) |
| Relapse | 13 (9%) | 15 (9.7%) | 9 (8%) |
| Strain (n, %) | |||
| NSCLC | 8 (5.6%) | 18 (11.7%) | 12 (10.6%) |
| Adenocarcinoma | 69 (47.9%) | 73 (47.4%) | 54 (47.8%) |
| Undifferentiated | 1 (0.7%) | 0 | 3 (2.7%) |
| Squamous | 51 (35.4%) | 35 (22.7%) | 32 (28.3%) |
| Small cell | 11 (7.6%) | 20 (13%) | 11 (9.7%) |
| Other | 4 (2.8%) | 8 (4.9%) | 1 (0.9%) |
| Diagnostic method (n, %) | |||
| Bronchoscopy | 66 (45.8%) | 67 (43.5%) | 55 (48.7%) |
| EBUS | 14 (9.7%) | 11 (7.1%) | 11 (9.7%) |
| Thoracocentesis | 11 (7.6%) | 11 (7.1%) | 8 (7.1%) |
| Surgery | 26 (18.1%) | 29 (18.8%) | 16 (14.2%) |
| CT-CNB/FNAB | 21 (14.6%) | 22 (14.3%) | 19 (16.8%) |
| US-CNB | 6 (4.2%) | 8 (5.2%) | 1 (0.9%) |
| Pleural biopsy | 0 | 3 (1.9%) | 3 (2.7%) |
| Sputum cytology | 0 | 3 (1.9%) | 0 |
| Final stage | |||
| IA–IB–IIA | 25 (17.5%) | 30 (19.4%) | 18 (16%) |
| IIB–IIIA–IIIB | 41 (28.6%) | 45 (29.2%) | 31 (27.4%) |
| IIIC–IVA–IVB | 77 (53.6%) | 79 (51.3%) | 64 (56.6%) |
| Treatment | |||
| Surgery | 31 (21.5%) | 27 (17.5%) | 23 (20.4%) |
| Surgery + CTP/RTP | 11 (7.7%) | 19 (12.3%) | 3 (2.7%) |
| Systemic treatment | 56 (38.9%) | 53 (34.4%) | 40 (35.4%) |
| Dual (CTP + RTP) | 25 (17.4%) | 19 (12.3%) | 19 (16.8%) |
| RTP/SBRT | 7 (4.9%) | 10 (6.5%) | 9 (8%) |
| Endoscopic treatment | 3 (2.1%) | 2 (1.3%) | 0 |
| Palliative care | 8 (5.6%) | 10 (6.5%) | 6 (5.3%) |
| Death | 3 (2.1%) | 14 (9.1%) | 13 (11.5%) |
CT-CNB/FNAB: computed tomography-guided core needle biopsy/fine needle aspiration biopsy; CTP: chemotherapy; EBUS: endobronchial ultrasound; NSCLC: non-small cell lung carcinoma; RTP: radiotherapy; SBRT: stereotactic body radiotherapy; SD: standard deviation; US-CNB: ultrasound-guided core needle biopsy.
When comparing the number of lung cancer diagnoses made throughout these months in 2020, we detected a marked decrease in the number of diagnoses recorded compared with the previous two years (Fig. 1). In terms of the diagnostic methods used, we detected a slight decrease in the diagnoses reached with the aid of endoscopic and surgical techniques, albeit not statistically significant, as well as a decrease in staging by invasive methods (23.9% in 2020 vs. 29.2% in 2019 and 27.1% in 2018) with respect to radiological staging, with no significant increase being found in the conduct of punctures guided by computed tomography (CT). However, when exclusively analyzing the confinement period, we did observe a decrease in the use of endoscopic techniques.
To study the differences in the time elapsed until the administration of the first treatment over the years, we carried out a oneway analysis of variance (ANOVA), detecting differences between the years under study (F [2408] = 3.67; p = 0.026). A subsequent post hoc Tukey test revealed that the differences between 2018 and 2020 was statistically significant (p = 0.037). In contrast, when comparing 2019 with 2020, we observed a trend that was not statistically significant (p = 0.054). A chi-squared (χ2) test was carried out to compare the different cancer stage frequencies, without detecting any differences in the distribution of cancer stages throughout the years (p = 0.737), although both the delay and decrease in the number of diagnoses could have resulted in a diagnostic delay and, consequently, an increase in the percentage of advanced stages in the following months. No statistically significant differences were found in the type of treatment received.
These results may be due to the discontinuation of medical consultations in both primary care centers and hospitals, the interruption or delay of diagnostic testing, as well as the fact that patients themselves avoided visiting health centers and hospitals because of the pandemic situation.
The findings of this study confirm a decrease in the diagnoses of new cases of lung cancer during the first months of the COVID-19 pandemic, as well as a significant increase in the time elapsed until the first treatment. However, our results do not allow us to demonstrate that the decreased healthcare activity during said months implied, for the time being, an increase in the number of patients presenting with more advanced cancer stages in our setting. A longer follow-up will likely shed more light on the effects of the first phase of the COVID-19 pandemic on lung cancer diagnosis and its prognostic implications.
Conflicts of interestThe authors of this paper declare no conflicts of interest.
Please cite this article as: Serra Mitjà P, Àvila M, García-Olivé I. Impacto de la pandemia por COVID-19 en el diagnóstico y tratamiento del cáncer de pulmón. Med Clin (Barc). 2022;158:139–140.
