




Endotoxin is considered to be one of the key triggers of fatal shock during severe sepsis and one of the main driving factors of systemic inflammation.1 Here, we report two cases of endotoxin adsorption in critically ill COVID-19 patients during ECMO.
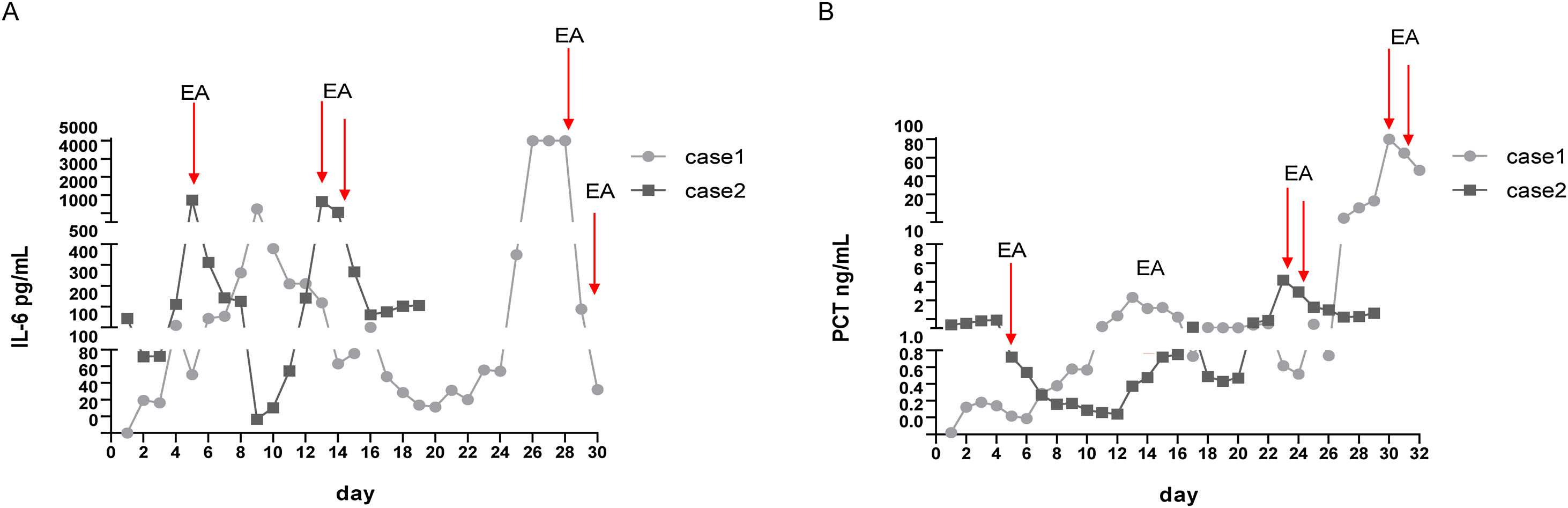
An 80-year-old woman was admitted to the hospital on October 24, 2021 due to the diagnosis of COVID-19. She received treatment in the awake prone position in the general ward. However, due to deterioration of lung disease and deterioration of renal function, he was transferred to ICU on November 4, 2021. On November 6, 2021, the patient underwent tracheal intubation and mechanical ventilation. Due to severe hypoxaemia, she received V-V ECMO treatment on November 07, 2021. On November 23, 2021, procalcitonin (PCT, 25.75ng/L) and interleukin-6 (IL-6, >5000pg/mL) levels increased significantly. The blood pressure dropped to 85/52mmHg. She received noradrenaline 1.0μg/kg/min continuous intravenous pumping, and her blood pressure was maintained at 98–110mmHg/65–78mmHg. She has severe metabolic acidosis and hyperlactic acidosis (>20mmol/L). She received endotoxin adsorption treatment (Oxiris) on 2021-11-24 and 2021-11-25. After endotoxin adsorption treatment, PCT decreased from 100ng/L to 66.42ng/L, and IL-6 decreased from 5000pg/mL to 52.21pg/mL. The dose of noradrenaline was reduced to 0.2μg/kg/min on November 26, 2021, and was withdrawn on November 28, 2021. The changes of patients’ IL-6 and PCT are shown in Fig. 1.
 and PCT level (B) in case 1 and case 2 during hospitalization. IL-6: interleukin-6; PCT: procalcitonin; EA: endotoxin adsorption.")
A 69-year-old female patient was admitted to the hospital on October 20, 2021 due to COVID-19. During the treatment, the patient developed fever (39°C) and fatigue and shortness of breath, and received high-flow oxygen. The patient was transferred to the ICU on October 27, 2021 due the worsening condition. She received endotracheal intubation and prone ventilation immediately after transfer to ICU. On the second day after ICU admission, the patient received V-V ECMO treatment. On October 31, 2021, the patient's temperature was 39.5°C and blood pressure dropped to 75/55mmHg. The PCT was 0.922ng/L and IL-6 was 1731.00pg/mL. We used noradrenaline 0.6μg/kg/min to maintain blood pressure (95/67mmHg). On November 1, 2021, she received endotoxins adsorption treatment once. The next day, her norepinephrine dose was reduced to 0.6μg/kg/min and her maximum temperature is 38.2°C. The rechecked IL-6 level also decreased to 414.00pg/mL. On November 4, 2021, her shock improved and norepinephrine was stopped. However, the patient suffered from septic shock again on November 19, 2021. She was received noradrenaline 0.5μg/kg/min to maintain blood pressure (102/74mmHg). Therefore, she received endotoxins adsorption treatment on November 20 and 21, respectively. After two endotoxins adsorption treatments, her septic shock was rapidly relieved. The dose of noradrenaline was 0.5μg/kg/min on November 23, 2021. On November 27, noradrenaline was withdrawn. The changes of patients’ IL-6 and PCT are shown in Fig. 1.
The increase in serum creatinine, D-dimer, lactate dehydrogenase, C-reactive protein, PCT, and white blood cell count may indicate superimposed infectious condition.2 Serum SARS-CoV-2 nucleic acid is closely related to cytokine storm and extremely high serum levels of IL-6. Cytokine storm is a disease caused by the extensive activation of the immune system, the result of which is the massive production of cytokines and chemokines. Since cytokine storms can lead to multiple organ failure, it is important to reduce or suppress inflammatory storms. Patients with viral respiratory infections often suffer from severe secondary bacterial infections, which are usually associated with high morbidity and mortality.3
Endotoxin adsorption is proposed to reduce the burden of cytokines by reducing the peak value of specific exogenous targets (endotoxin), thereby restoring immune homeostasis without prolonging the immunosuppressive state. A study showed that the use of polymyxin B hemoperfusion in patients with septic shock caused by various pathogens infected by COVID-19, and reported the decrease of SOFA score after two sessions of polymyxin B hemoperfusion.4 In the two patients we reported, after two consecutive endotoxin adsorption, the level of serum IL-6 in the patients was significantly decreased. In addition, the patient's PCT level also has a downward trend. However, neither of the two cases reported here has detected the level of endotoxin, so it can not directly show the efficacy of Toraymixin in absorbing endotoxin.
Ethical approvalThis report is supported by the medical ethics committee of the Affiliated Hospital of Zunyi Medical University. The consent was voided due to retrospective nature of the study. We presented only deidentified data.
FundingThis report has not received any funding support.
Conflict of interestThere is no conflict of interest.
We thank all the doctors, nurses and staff of Jiangjunshan Hospital.
