

The purpose of this case report is to introduce a method for a successful treatment of high astigmatism with a new orthokeratology design, called FOKX (Falco Kontaktlinsen, Switzerland). This novel toric orthokeratology contact lens design, the fitting approach and the performance of FOKX lenses will be illustrated in the form of a case report. Correcting astigmatism with orthokeratology offers a new perspective for all patients suffering astigmatism.
El objetivo de este informe de caso es presentar un método para el tratamiento satisfactorio del astigmatismo de alto grado con un nuevo modelo de ortoqueratología llamado FOKX (Falco Kontaktlinsen, Suiza). Este nuevo modelo de lente de contacto tórica de ortoqueratología, el modo de colocación y la eficacia de las lentes FOKX se ilustrarán en un informe de caso. La corrección del astigmatismo por ortoqueratología ofrece una nueva perspectiva para todos los pacientes astigmáticos.
Orthokeratology is a reversible1 method for myopia reduction. The FDA approved myopia reduction up to −6.00D with the ParagonCRT©2 but most manufacturers (eg. Paragon, Procornea, Galifa, Technolens, Ultravision etc.) declare the maximal possible myopia correction between −3.50D and −4.50D on their websites. In this range a successful reduction of myopia should be achieved. The higher the myopia to be treated, the larger increase higher in order aberrations (i.e. coma, spherical aberration) with negative impact in visual acuity.3 This doesn’t mean that higher amount of myopia can’t be treated successfully (Tung HS. Global Orthokeratology Symposium 2004; Free Paper Session), but the patient should be informed about potential visual distortions, especially during night vision.
Regular astigmatism rarely present a challenge to the professional optometric eyecare. However for orthokeratology, astigmatism can make simple fits very complicated. Greater amounts of astigmatism were suggested to be impossible to be treated with orthokeratology.4 The limit for astigmatism treatment during orthokeratology was adopted from most of the manufacturers throughout the world as 1.50D for with-the-rule and 0.75D for against-the-rule astigmatism. However, does not seem to be a rationale for such limitations. To understand such limitations that question we have to think about the basic procedure of reshaping the cornea during orthokeratology. Accelerated orthokeratology uses reverse geometry contact lenses for flattening the corneal curvature. This will lead in reducing the power of the cornea and myopia of the whole eye. Astigmatism produces two major problems during orthokeratology. First, due to the fact that with symmetric lens designs (equal sagital depth in each meridian) we only can flatten the flattest meridian and insufficiently transform the steeper meridian, as a worst scenario, we will increase instead of decreasing the amount of astigmatism. Second, achieving proper and stable fitting is almost impossible with a rotational symmetric lens design. The contact lens will rock and decenter along the two meridians, leading into smiley face (high ride) or frowny face (low ride) topography pattern. Both complications are reducing the visual acuity to unacceptable levels.
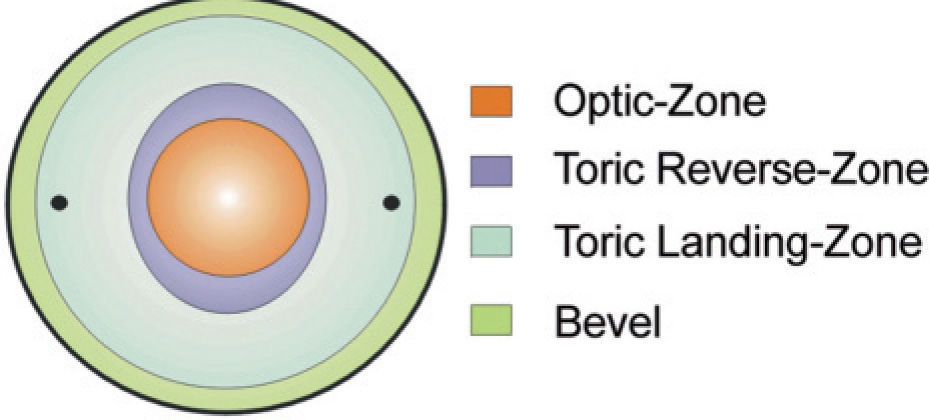
Falco Kontaktlinsen (Switzerland) introduced 2003 the new toric orthokeratology design FOKX. This design allows the treatment of astigmatism up to 7.00D. The backsurface contact lens design is illustrated in Figure 1.
.")
A retrospective, multi-center study presented at the Global Orthokeratology Symposium 2006 showed that out of 102 patients 82.5% were successful fitted. (Baertschi M. Global Orthokeratology Symposium 2005). This case report will concentrate only on the fitting approach and treatment of high astigmatism with the FOKX contact lens design.
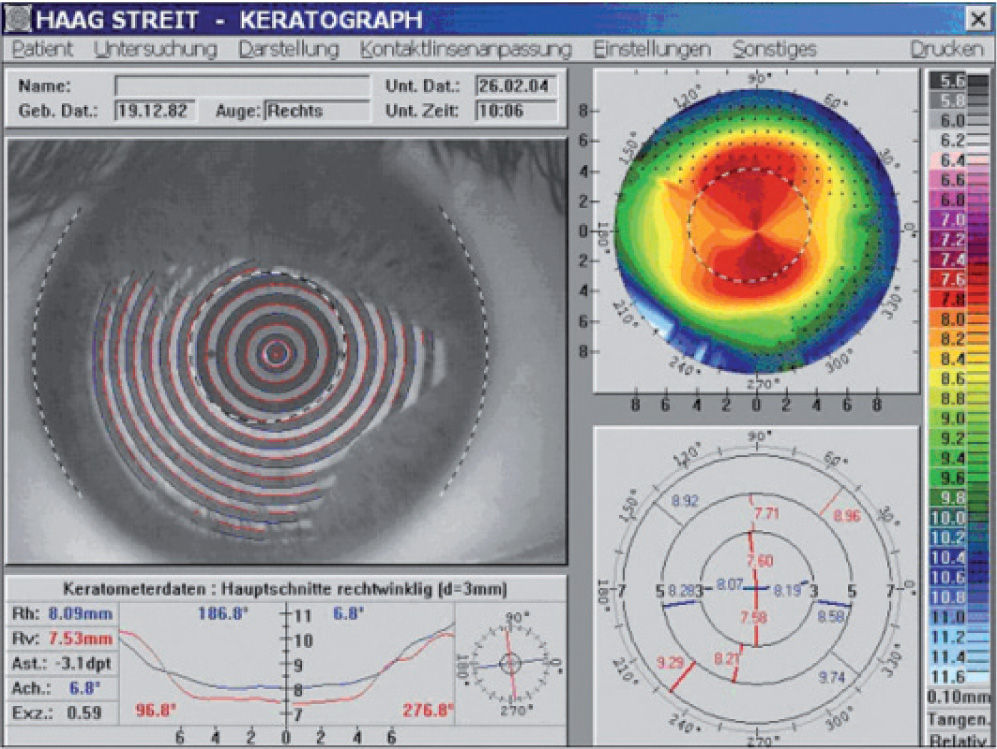
Case reportA 22 years-old male presented with a subjective refraction of −4.25D −3.75D × 8° in the right eye. Best spectacle corrected visual acuity was 20/25 in that eye. Corneal astigmatism was −3.10D × 7° of with-the-rule astigmatism (difference in radii of 0.56 mm) (Figure 2).

It is critical to compare the amount of astigmatism presented on the cornea with spectacle correction. With orthokeratology only the cornea astigmatism can be corrected. This will lead in this patient, after successful orthokeratology fitting, to a residual astigmatism of about half a diopter at 8°. This marginal failure should be presented to the patient with glasses, so that the patient can decide if he is willing to undergo the treatment or not.
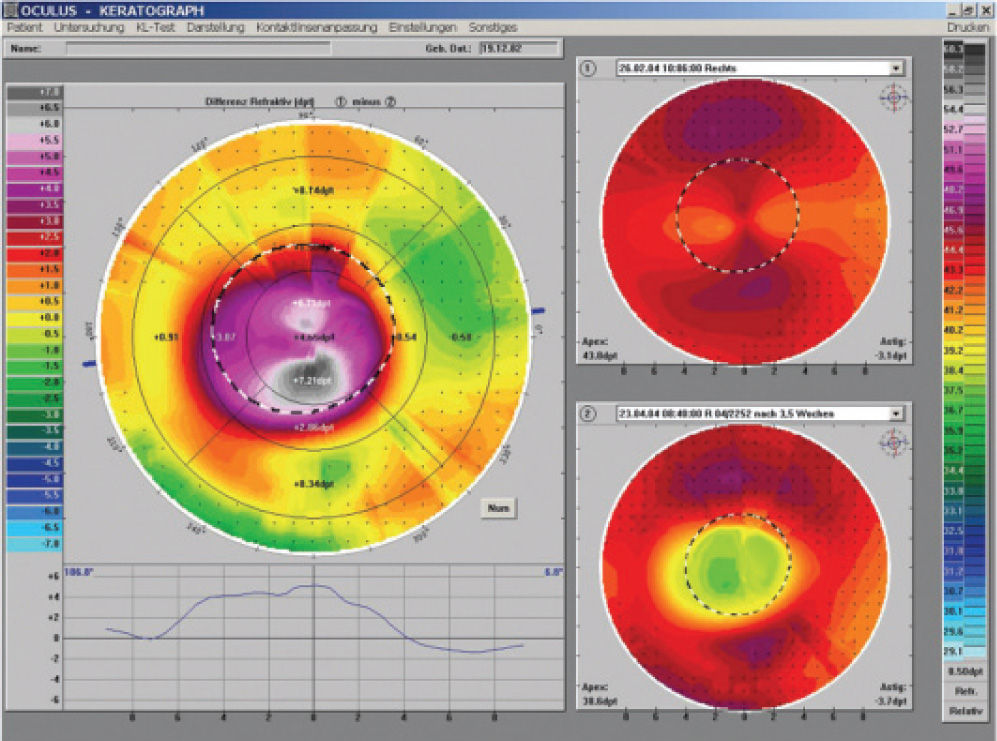
The manufacturer's calculation software was used to determine the FOKX lens to be fitted (Base Curve: 8.95 mm, Power +1.0D, Total diameter: 10.60 mm, Material: Boston XO Red). At the last fitting appointment, after two month, the patient presented a satisfactory topography pattern. All corneal astigmatism was successfully corrected. The treatment zone is perfectly centered and the cornea was corrected horizontally by 4.50D whereas the vertical meridian showed a change of about 7.00D (Figure 3).

The subjective correction post treatment showed plano −0.50D × 8°. Uncorrected visual acuity increased up to 20/20 without notice of halos or other disturbing phenomena. Conversely, the optical zone remained relative small. Follow-up was scheduled for every 6 month.
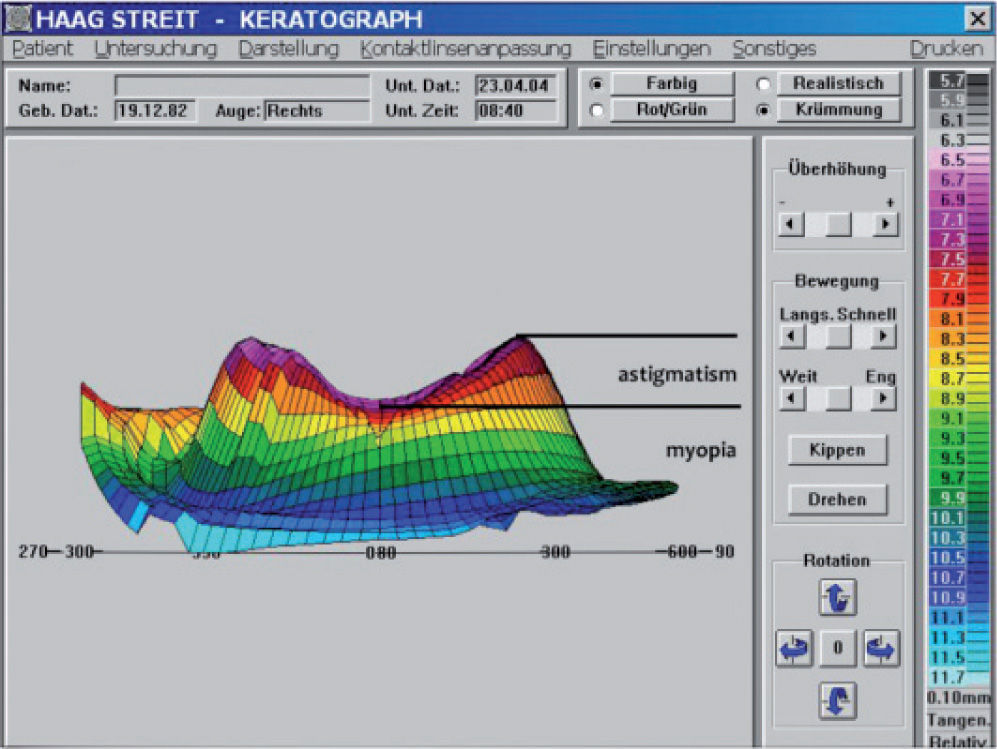
DiscussionIf we take a look at the 3D image, provided by the topographer in horizontal view, the different amount of myopia in each meridian corrected is clearly visible. There's something like a “valley” in the middle and two elevations. The margins of the valley in the direction of the lower elevation, shows the change of the corneal curvature due to amount of myopia corrected. Instead, whereas the direction of both peaks to the side of the treatment zone represent the combined correction of myopia and astigmatism, which must show up in a higher difference in corneal curvature, due to the higher amount of total myopia in this meridian (Figure 4).

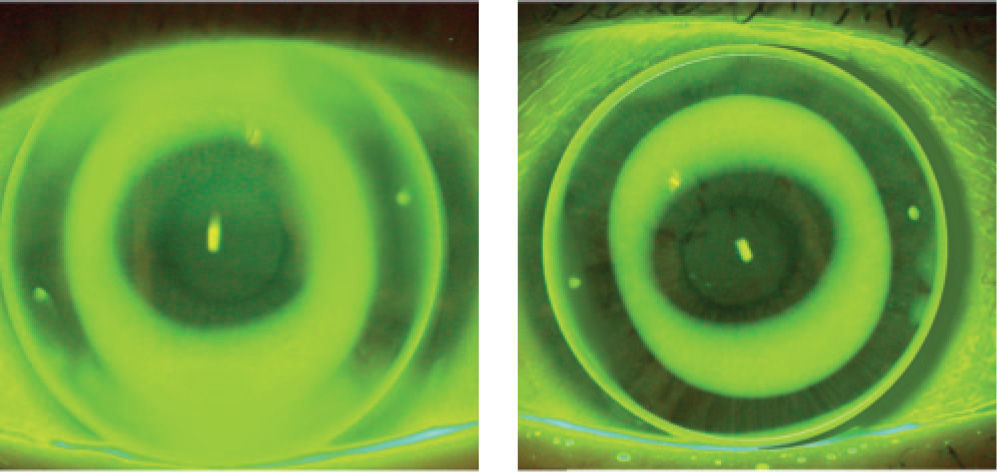
While a simple toric or peripheral toric landing-zone provide stabilisation, doesn’t correct significant amounts of astigmatism. Correction of corneal astigmatism needs a perfectly closed reverse-zone in every meridian and that's only possible to achieve with a toric reverse-zone to modulate the hydrodynamic forces driving corneal flattening in each corneal meridian separately. If we take a look on our case with a traditional or even periphertoric orthokeratology lens design on that cornea, the fluorescein pattern look like the left image (Figure 5).

It is observed that reverse-zone doesn’t close up tight enough along the vertical meridian and the lens can’t build up enough power in that meridian to correct the full amount of corneal astigmatism. If we compare the fluorescein pattern of the FOKX design, the reverse-zone does really close up in all meridians and additionally present clear distinguished edges. While observing the reverse-zone carefully, the toric design is visually recognisable, due to the changing width of the fluorescein band in the reverse-zone. Likewise the toric landing-zone shows perfect alignment with the toric periphery of the cornea and make sure that the contact lens will fit in t on the eye.
In summary, while orthokeratology has demonstrated to be a safe and predictable procedure to temporary correct myopia, the new orthokeratology contact lens design FOKX provide successful outcomes in treatment of high amounts of astigmatism. The Falco calculation software was helpful in reducing the chair time and the amount of contact lenses needed for fitting to just one pair in this case. Correcting astigmatism with orthokeratology offers a new perspective for all patients suffering from astigmatism.
Conflict of interestsThe authors do not have any financial interest on any noted company or product in this article.





