



Unwanted mental intrusions (UMIs) with contents related to Obsessive-Compulsive Disorder (OCD), Body Dysmorphic Disorder (BDD), Illness Anxiety Disorder (IAD), and Eating Disorders (EDs) are highly prevalent, independently of the cultural and/or social context. Cognitive-behavioral explanations for these disorders postulates that the escalation from common UMIs to clinically relevant symptoms depends on the maladaptive consequences (i.e., emotions, appraisals, and control strategies) of experiencing UMIs. This study examines, from a cross-cultural perspective, the cognitive-behavioral postulates of the maladaptive consequences of having UMIs.
MethodNon-clinical 1,473 participants from Europe, the Middle-East, and South America completed the Questionnaire of Unpleasant Intrusive Thoughts to assess the maladaptive consequences of experiencing highly disturbing OCD, BDD, IAD, and EDs-related UMIs.
ResultsFindings revealed main effects for both the country and the consequences associated with the four UMI contents. Interaction effects between the consequences of each UMI content and the sample location were also observed.
ConclusionsCognitive-Behavioral models for OCD, BDD, IAD, and EDs should be implemented along with socio-cultural variables that increase the understanding of the role of these variables in the phenomenology of UMIs and their associated consequences.
Las intrusiones mentales no deseadas (IM) de contenidos relacionados con el Trastorno Obsesivo-Compulsivo (TOC), el Trastorno Dismórfico Corporal (TDC), la Ansiedad por la Enfermedad (AE), y los Trastornos Alimentarios (TAs) son muy prevalentes, independientemente de la cultura y/o el contexto social. Las explicaciones cognitivo-conductuales de esos trastornos postulan que la escalada de IM normales a síntomas clínicamente relevantes depende de las consecuencias desadaptativas (i.e., emociones, valoraciones y estrategias de control) de las IM. Este estudio examina los planteamientos sobre dichas consecuencias desde una perspectiva transcultural.
Método1.473 participantes de Europa, Oriente Medio y Suramérica completaron el Inventario de Pensamientos Intrusos Desagradables para evaluar las consecuencias desadaptativas de experimentar IM muy molestas con contenidos de TOC, TDC, AE y TAs.
ResultadosSe obtuvieron efectos principales tanto para el país como para las consecuencias asociadas con los cuatro contenidos de IM, así como efectos de interacción entre las consecuencias de cada modalidad de IM y la localización de la muestra.
ConclusionesLos modelos cognitivo-conductuales sobre el TOC, el TDC, la AE y los TAs deben complementarse con variables socioculturales que aumenten la comprensión del papel de esas variables en la fenomenología de las IM y sus consecuencias asociadas.
Cognitive behavioral theories trace the origins of obsessions to commonly occurring unwanted mental intrusions (UMIs) that are universally experienced in the general population. Initially proposed by Rachman and De Silva (1978), this suggestion has been supported by several cross-cultural studies (i.e., Clark et al., 2014; Moulding et al., 2014; Pascual-Vera et al., 2019; Radomsky et al., 2014).
Most of the research on UMIs has typically focused on Obsessive-Compulsive Disorder (OCD) themes. Nevertheless, UMIs have been proposed as transdiagnostic variables operating across clinically different disorders (Pascual-Vera & Belloch, 2018a, 2018b; Pascual-Vera et al., 2017). For instance, UMIs have been described as normal variants of preoccupations about perceived appearance defects in Body Dysmorphic Disorder (BDD) (Giraldo-O'Meara & Belloch, 2018; Osman et al., 2004), images related to illnesses and death in Illness Anxiety Disorder (IAD) (Arnáez et al., 2017, 2021; Muse et al., 2010), and thoughts and impulses about eating and food in Eating Disorders (EDs; Belloch et al., 2016; Thaiposri & Reece, 2020).
Cognitive-behavioral approaches to OCD, BDD, IAD and EDs, posit that the critical point in transforming normal UMIs into clinically significant symptoms resides in the negative consequences of their disruption to the normal flow of thoughts. Among these consequences, the research highlights the dysfunctional appraisals of the significance of the intrusions, which are then followed by emotional distress, interference, and egodystonicity. All these consequences lead individuals to engage in maladaptive attempts to neutralize or control the unwanted mental intrusions. These assumptions have found considerable support, in both non-clinical and clinical samples, for OCD (i.e., García-Soriano et al., 2011), the BDD (Fang & Wilhelm, 2015; Giraldo-O'Meara & Belloch, 2017, 2018; Onden-Lim & Grisham, 2014; Senín-Calderón et al., 2020), the IAD (Arnáez et al., 2020, 2021; Fergus, 2013), and the EDs (Belloch et al., 2016).
Taken together, all of these studies suggest that the characteristics of BDD, IAD, and EDs parallel the symptoms of OCD: obsessions, compulsions, and the functional relationship between them. Recent support for this claim comes from a study by Pascual-Vera and Belloch (2018b) that examines the functional links between UMIs with OCD, BDD, IAD, and EDs-related contents in the same individual. The results showed similarities and differences in the maladaptive consequences linked to the four UMI contents. IAD-related intrusions caused the highest emotional distress, but not differences were observed among OCD, BDD and EDs-related intrusions. OCD-related intrusions were the most interfering, whereas EDs intrusions interfered less than all the other UMIs. The four UMIs were equally ego-dystonic, and they were similarly appraised by both men and women, except for the OCD-related intrusions, which were more dysfunctionally appraised by women. Finally, the four UMIs instigated the urge to “do something”, supporting the link between unwanted mental intrusions and behaviors to alleviate the discomfort they cause.
Nevertheless, the perceived negative consequences associated with the experience of UMIs, irrespectively of their content, could be modulated by cultural variables. Following Marsella and Yamada (2010): “Culture is shared learned behavior and meanings that are socially transmitted for purposes of adjustment and adaptation (…) It is represented internally (i.e., cognitively, emotionally) by values, attitudes, beliefs, epistemologies, (…) coded in verbally, imagistically, proprioceptively, viscerally, and emotionally, resulting in different experiential structures and processes” (p. 105). From this perspective, cultural variables influence how and when the emotional expression of the UMI is culturally suitable/acceptable, or to what extent the immediate appraisal of a given thought, feeling or impulse depends on the implicit beliefs and values ascribed to these thoughts, feelings and impulses (Inozu et al., 2012; Nicolini et al., 2017; Sica et al., 2002). These issues have partly been studied regarding OCD-related intrusive thoughts. Sica et al. (2006) compared the beliefs about obsessive UMIs in three groups of non-clinical individuals from Italy, Greece, and the US. Results indicated that beliefs were correlated with symptoms in all three groups. Significant, albeit modest, cross- cultural effects were found, because the relationship between beliefs and cleaning and checking compulsions tended to be low in Greek participants, compared to Italian and US counterparts. In a study of non-clinical samples from 13 countries across six continents, Moulding et al. (2014) showed that the relationships between the frequency of obsessive intrusions and their associated appraisals and control strategies were similar across countries. Pascual-Vera et al. (2019) conducted the largest study published to date on the cross-cultural differences in the expression of UMIs related to OCD, BDD, IAD, and EDs in 1,473 non-clinical adults from 10 cities in seven countries and three continents. They found that 64% of the total sample reported having experienced all four UMIs. EDs-related intrusions were the most frequently experienced, whereas IAD intrusions were the least frequent, but the most disturbing. All the UMIs were significantly related to each other in terms of frequency and disturbance, and all of them were associated with clinical measures of OCD, BDD, IAD, and EDs. In a study with university students Pascual-Vera and Belloch (2021b) found that up to 61.53% of the participants who experienced UMIs related to OCD, BDD, IAD, and EDs presented high risk to OCD and reported more negative consequences when they experienced UMIs, whatever it was their content. Similar results were also found in up to 71% individuals with OCD, who experienced UMIs with different contents not always related to typical obsessive themes (Pascual-Vera & Belloch, 2021).
The above-mentioned studies show the relevance of examining to what extent cultural differences might be associated with the experience of UMIs, and they suggest the need to conduct cross-cultural studies to improve our knowledge about how psychological phenomena might vary across cultural groups (Koç & Kafa, 2019; Sica et al., 2006). This was the main research question of current study, since it seeks to examine cross-cultural differences in the perceived maladaptive consequences of the four sets of UMIs: obsessive, dysmorphic, illness, and eating-disorders related. A within-subject perspective was adopted, with the aim of reducing the variability in the putative differential consequences of different UMI contents in the same individual. The cross-cultural expression of the four UMI contents was compared across participants from different countries and continents. We would expect that there will be differences in the emotional impact, interference, egodystonicity, and dysfunctional appraisals individuals attach to the UMIs, and in the thought control and/or neutralizing strategies used to manage them, depending on the participants’ country and culture, beyond differences between the four UMIs. Only participants who had experienced all four types of UMIs in the past three months were included in these analyses, which makes these intrusions closer to those experienced by individuals with the disorders related to their contents.
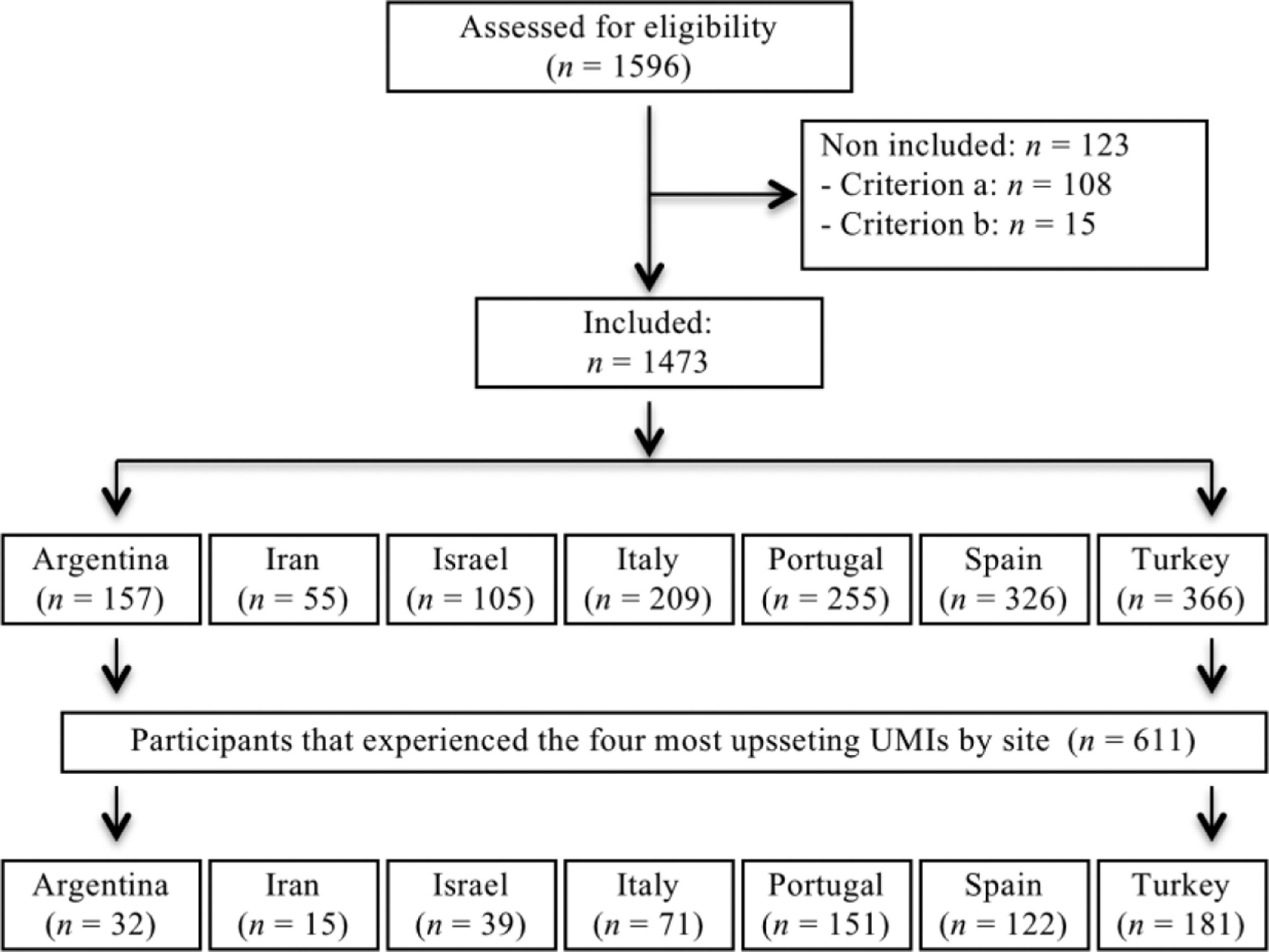
MethodParticipantsA sample of 1,473 participants in 10 cities in seven countries and three continents volunteered to participate in the current study. The sites were in the Middle East and Asia (Herzliya, Tel Aviv in Israel; Ankara in Turkey; and Tehran in Iran), Europe (Firenze and Padova in Italy; Algarve in Portugal; Valencia, Teruel, and Madrid in Spain), and South America (Buenos Aires in Argentina). Of the total sample, 74% of the participants (n = 1,086) were women, and 26% (n = 387) were men (χ2= 331.70, p < .0001). Their ages ranged from 18 to 64 years (M = 28.09, SD = 11.24 years). Most of the participants in all the countries (70.2%) had university studies. Having diagnosed mental health problems in the past six months, undergoing psychological or pharmacological treatment (criterion a), or not being in the 18-to-65 age range (criterion b) were non-inclusion criteria. A total of 123 individuals (criterion a, n = 108; criterion b, n = 15) were not included in the data analyses. From the initial sample, a total of 611 individuals (M = 25.88, SD = 9.78 years; 80% women) reported having experienced the four most upsetting UMI in the past three months. Consequently, this was the final sample included in the study. Figure 1 shows the participants flowchart. The demographic characteristics of participants by site are on Table 1.

Demographic characteristics of participants that experienced the four most upsetting UMIs by site.
Note. Values which share the same superscript letter were not significantly different from each other. Differing superscript letters indicate post-hoc between-groups differences (Dunnett and Bonferroni corrections for Mean (SD) and %, respectively).
Socio-demographic data sheet. The data required were the following: age, gender, years of education, marital status, and socio-economic level. Two additional questions about the participants’ current mental-health status were also included: (1) Do you have been diagnosed of a mental or behavioral disorder during the past six months, or are you currently receiving treatment for a mental or behavioral disorder? (2) If yes, could you write please the diagnosis and/or the treatment you are receiving for this mental or behavioral disorder?
Questionnaire of Unpleasant Intrusive Thoughts (QUIT; Pascual-Vera et al., 2019). This self-report explores unwanted mental intrusions related to obsessive, dysmorphic, hypochondriacal, and EDs-related themes and the functional links (emotions, appraisals, and control strategies) of each set of intrusions. After a detailed definition of UMIs and the different ways they can be experienced, four separate sets of intrusions are presented: OCD-related (12 items), BDD-related (9 items), IAD-related (10 items) and EDs-related (8 items). An additional set of relationship-related obsessive-compulsive phenomena (11 items) were also included, based on the work by Doron and colleagues (e.g., Doron et al., 2014). Respondents have to evaluate each UMI on its frequency (from 0 = never, to 6 = always) and the discomfort (from 0 = not at all, to 4 = extremely) it produces when it occurs.
After completing each set of intrusions, the respondent is asked to choose from the previous list the most upsetting intrusion s/he experienced in the past three months as much with a frequency ≥1 (Rarely, once or twice). Next, the consequences associated with the respondent's most upsetting intrusion are evaluated through 14 items (from 0 = never/not at all, to 4 = always/frequently) that assess the emotional distress experienced, the interference, the associated egodystonicity, the maladaptive meanings the individual attaches to the selected intrusion, and the control and/or neutralizing strategies the person uses to manage the intrusion. The current study focuses on the scores on these consequences. The Cronbach alpha values obtained in each site were from acceptable to satisfactory (Table 2).
ProcedureThe study of the cross-cultural expression and transdiagnostic nature of UMIs was proposed at the 3th and 4th meetings of the Research Consortium on Intrusive Fears (RCIF), to which all the authors pertain, which were held in Valencia, Spain and Ankara, Turkey in 2014 and 2016, respectively. Two former pilot studies of the QUIT were conducted in Spanish community samples (Pascual-Vera et al., 2017; Pascual-Vera & Belloch, 2018b). The Spanish version of the QUIT was first translated to English, and then back translated to Spanish by an accredited English-Spanish translator. The final English version of the QUIT was translated and back-translated into the various languages in which it should be applied (Hebrew, Italian, Persian, Portuguese, and Turkish), following a standardized translation/back- translation protocol adopted by all authors. This protocol produced translated versions of the QUIT in seven languages (English, Hebrew, Italian, Persian, Portuguese, Spanish, and Turkish). Participants were recruited by the authors in each site from January 2017 to January 2018 from several sources: undergraduate students who attended their lectures at the University, advertisements on the University Campus, and the web page of each research group, requesting voluntary participation in a study on values and beliefs about thoughts. Those who explicitly agreed to participate and provided informed written consent were scheduled to attend an assessment session. A common data template was created to enter the same labels and categories across sites. The research protocol was approved by the Research Ethics Committee of the University of Valencia, in Spain (number H1385632037445).
Data analysesThe consequences of experiencing the four UMI across the seven countries were examined using four different two-way mixed MANOVAs, once the homogeneity of variances (homoscedasticity) and muticollinearity were examined. The within-subjects factor was the content of the UMI (4 levels), and the between-groups factor was the site of the participants (7 levels, one per site), with the dependent variable being the scores on the consequences associated with each UMI (i.e., emotional impact, interference, egodystonicity, appraisals, and control strategies). Bonferroni adjustments for multiple post-hoc comparisons and effect sizes (η2) were calculated. These analyses were performed with the Huynh-Feldt correction because Mauchly's tests of sphericity were violated. Data were analyzed using IBM SPSS Statistics (version 22).
ResultsPreliminary dataAs shows Table 1, up to 41.4% (n = 611, Mage = 25.88, SD = 9.78; 80% women) of the sample reported having experienced the four most upsetting UMI in the past three months. The percentage rates of participants who experienced the four UMI modalities differed across countries (χ2 = 200.84, p < .0001). Between-group comparisons showed that the highest percentages of participants who experienced all the UMIs were Turkish (n = 181; 29.67%), Portuguese (n = 151; 24.75%), and Spanish (n = 122; 20%), and the lowest percentages were for Iranian (n = 15; 2.45%), Argentinian (n = 32; 5.24%), Israelis (n = 39; 6.39%), and Italian (n = 71; 11.63%) participants.
The mean frequency and discomfort caused by these UMI were moderate (Table 3). Participants reported that the last time they experienced OCD-related and IAD-related intrusions was typically in the last month (OCD) and 3 months (IAD) before the time of the survey, whereas BDD and EDs intrusions were experienced daily. In all the participating countries, the most upsetting OCD-related intrusion was having doubts about leaving something on (e.g., kitchen stove, gas), the most upsetting BDD-related intrusion was about noticing an appearance defect, the most upsetting IAD-related intrusion was about a loved one having a serious disease, and, lastly, the most upsetting EDs-related intrusion was about being fat.
Frequency and disturbance of the four mental intrusions that participants selected as most upsetting.
| Unwanted mental intrusions | Frequency | Disturbance |
|---|---|---|
| OCD-related | 3.23 (1.35) | 2.60 (1.05) |
| BBD-related | 3.05 (1.37) | 2.31 (1.12) |
| IAD-related | 2.49 (1.26) | 2.64 (1.12) |
| EDs-related | 3.38 (1.46) | 2.22 (1.17) |
Note. Data are Mean (SD).
The age was negatively associated with the emotional impact caused by the BDD, IAD, and EDs related intrusions, respectively (r = -.18, r = -.16, r = -.13; all p’s ≤.01) and with the interference (r = -.12, r = -.11, for BDD, and EDs related intrusions, respectively; all p's ≤ .05). Nonetheless, the correlation coefficients were small, with R2 ranging from .006 to .03.
Differences in the consequences of the most upsetting OCD, BDD, IAD, and EDs-related mental intrusions between the participants from the different countriesThe MANOVA results showed significant main effects for the between-country differences in the emotional impact of the UMIs (F(6, 587)= 9.42; p ≤ .01; η2 =.08), the interference in daily activities (F (6, 581) = 5.27; p ≤ .01; η2 =.05), the egodystonicity they caused (F (6, 584) = 6.67; p ≤ .01; η2=.64), the dysfunctional appraisals attached to them (F (6, 576) = 10.21; p ≤ .01; η2=.09), and the strategies used to control them (F (6, 566) = 10.05; p ≤ .01; η2=.09). In all cases, the effect size was medium. Given the significance of the overall tests, the univariate effects were examined. Post-hoc analyses indicated that Iranian, Portuguese, Spanish, and Turkish participants reported the highest emotional impact of the four UMI contents, whereas Israelis and Italians reported the lowest (Table 4).
Differences in the emotional impact caused by unwanted mental intrusions across countries and among four contents of intrusions
Note. Data are Mean (SD). Values which share the same superscript were not significantly different from each other. Superscripts a, b, c indicates post-hoc within-group (UMIs content) differences. Superscripts 1, 2, 3 indicate post-hoc between-groups differences (countries). Same superscript means no differences.
Regarding the interference caused by the four UMI contents, post-hoc analyses revealed that OCD intrusions were more interfering for Portuguese, Spanish, and Turkish participants, whereas they interfered less in the Italian participants. By contrast, in every site, the BDD and EDs-related intrusions caused a similar degree of interference, except in the Turkish individuals, who reported higher rates of interference by the BDD intrusions than Italian, and in the Iranian participants, who reported higher interference of EDs-related intrusions than Italian participants. In the case of IAD intrusions, Turkish and Portuguese reported the most interference, and Italian and Argentinian participants reported the least (Table 5).
Differences in the interference caused by unwanted mental intrusions across countries and among four contents of intrusions.
Note. Data are Mean (SD). Values which share the same superscript were not significantly different from each other. Superscripts a, b, c indicates post-hoc within-group (UMIs content) differences. Superscripts 1, 2, 3 indicate post-hoc between-groups differences (countries). Same superscript means no differences.
As for egodystonicity, in every site, OCD, BDD, and EDs intrusions were assessed similarly, except for Spanish, who experienced both BDD and EDs-related intrusions as more egodystonic, compared to both Italian and Turkish participants. Regarding IAD intrusions, two subgroupings emerged: Israeli, Portuguese, and Spanish participants experienced the IAD-related intrusions as more egodystonic than Argentinian, Italian, and Turkish participants (Table 6).
Differences in the egodystonicity caused by unwanted mental intrusions across countries and among four contents of intrusions.
Note. Data are Mean (SD). Values which share the same superscript were not significantly different from each other. Superscripts a, b, c indicates post-hoc within-group (UMIs content) differences. Superscripts 1, 2, 3 indicate post-hoc between-groups differences (countries). Same superscript means no differences.
Overall, the four UMI modalities were more dysfunctionally appraised by Iranian, Israeli, Portuguese, and Spanish than by Italian participants (Table 7). Taken together, Italians used the strategies to control all four intrusions less, but Turkish and Iranian used these strategies more (Table 8).
Differences in the dysfunctional appraisals about unwanted mental intrusions across countries and among four contents of intrusions
Note. Data are Mean (SD). Values which share the same superscript were not significantly different from each other. Superscripts a, b, c indicates post-hoc within-group (UMIs content) differences. Superscripts 1, 2, 3 indicate post-hoc between-groups differences (countries). Same superscript means no differences.
Differences in the control strategies used to manage unwanted mental intrusions across countries and among four contents of intrusions.
Note. Data are Mean (SD). Values which share the same superscript were not significantly different from each other. Superscripts a, b, c indicates post-hoc within-group (UMIs content) differences. Superscripts 1, 2, 3 indicate post-hoc between-groups differences (countries). Same superscript means no differences.
In the within-group comparisons (i.e., UMI content), significant differences were also observed, although with small size effects, in the emotional consequences of each UMI (F(2.858, 1677) = 18.35; p ≤ .01; η2= .03), the interference it caused (F(2.949, 1713) = 20.92; p ≤ .01; η2=.03), the dysfunctional appraisals (F (2.981, 1717) = 14.40; p ≤ .01; η2=.02), and the control strategies (F (2.940, 1664) = 10.15; p ≤ .01; η2= .01). However, there were no significant differences in the egodystonicity caused by each UMI (F(2.868, 1675) = 2.32). Post-hoc analyses indicated that IAD intrusions provoked the highest emotional impact in all the participants from Europe and Turkey, whereas Iranians, Israelis, and Argentinians assigned the same emotional impact to the four UMIs (Table 4). OCD-related intrusions were the most interfering for Spanish, Italian, Argentinian, Portuguese, and Turkish participants, although in the last two groups these intrusions were just as interfering as the IAD-related intrusions. Overall, the EDs intrusions were the least interfering for the participants from every country, except the Iranians, for whom these intrusions were the most interfering (Table 5). The egodystonicity caused by the four UMI contents was assessed equally by all participants (Table 6), but the dysfunctional appraisals attached to the UMI contents were different depending on the specific location of the sample (Table 7). Thus, Spanish and Italian assessed the four UMIs equally, the OCD-related were more dysfunctionally appraised by the Portuguese, the Iranian and Israelis assessed the IAD intrusions more dysfunctionally, and the Turkish assessed both the OCD and IAD intrusions more dysfunctionally. On the whole, participants in all countries made the least dysfunctional appraisals of the BBD and the EDs-related intrusions.
The use of control strategies to manage the four UMIs differed across the countries (Table 8). Thus, the Spanish, Portuguese, and Israeli participants used more control strategies when experiencing IAD intrusions than when experiencing EDs intrusions. In the middle were the OCD and BDD intrusions, which instigated similar control strategies. Similarly, Turkish participants used more strategies to control OCD, BDD, and IAD intrusions, compared to their low use to manage EDs-related intrusions. By contrast, Iranians, Italians, and Argentinians used similar strategies to keep all four UMIs under control, regardless of their content.
Finally, interaction effects were found between the consequences of each UMI content and the sample location on the emotional impact (F (17.146, 1677) = 2.15; p ≤ .05; η2=.022), interference (F(17.69, 1713) = 2.76; p ≤ .01; η2=.02), egodystonicity (F (17.21, 1675) = 3.52; p ≤ .01; η2=.03), dysfunctional appraisals (F (17.88, 1717) = 2.79; p ≤ .01; η2 = .02), and control strategies (F (17.64, 1664) = 2.45; p ≤ .01; η2=.02), although in all cases with small effect sizes.
DiscussionThe current study aimed to examine the maladaptive consequences of obsessive, dysmorphic, illness, and eating-disorders related UMIs in individuals from different countries and socio-cultural contexts. Up to 41% of the participants experienced the four most upsetting UMIs in the past three months, supporting the universality of normal unwanted mental intrusions with contents typically related to OCD, BDD, IAD, and EDs. According to cognitive-behavioral models, in all the locations the disturbing UMIs had negative consequences. They caused emotional distress and were interfering, egodystonic, and dysfunctionally appraised, and individuals deployed a variety of strategies to control them. These results coincide with previous studies of OCD intrusions (e.g., Clark et al., 2014; Moulding et al., 2014), suggesting that the general mechanisms and/or processes posited by the current cognitive-behavioral models about the critical role of UIMs in explaining the genesis of OCD, BDD, IAD, and EDs are not dependent on cultural diversity, as shown cross-cultural similarities on OCD symptom presentations, like contamination fears that results in washing compulsions (Williams et al., 2017).
Nevertheless, as expected, our data also reveal subtle differences across countries, suggesting that the cultural background influences the way individuals react to and interpret the different UMI contents. Overall, Spanish and Portuguese participants experienced the most maladaptive consequences when they had UMIs, whereas Italian reported the least. At the midpoint were Turkish and Iranian, although they were closer to the Spanish and Portuguese, whereas Israelis and Argentinians were closer to the Italian participants. The fact that individuals from each country did not experience the same rate of the four UMIs suggest that the tendency to experience more disturbing UMIs, as it occurred in Turkish, Portuguese, and Spanish participants, are due to the worst way (i.e., emotions, appraisals, etc.) in which individuals from these countries respond to their UMIs. This general pattern is consistent with the one reported by Pascual-Vera et al. (2019) when examining the general frequency and disturbance caused by OCD, BDD, IAD, and EDs-related intrusions. The authors found that Iranian and Turkish participants reported the highest frequency of UMIs, and Spanish and Portuguese experienced the highest discomfort, whereas Israelis, Italians and Argentinians reported the lowest rates of both frequency and discomfort. The similarities found among participants from different countries might be influenced by different factors, such as sharing cultural and historical factors related to geographical location (i.e., Spain and Portugal), the rather strict observance of religion and values (Christian Catholicism in Spain and Portugal, and Islam in Iran and Turkey), and the role of migration movements of Italians and Israelis to Argentina, which were specially relevant at the end of the 19th century for Italians (Sergi, 1983) and across the first four decades of the 20th century for Jewish people. Nonetheless, the low rates of UMIs endorsed by Italian participants compared with both Spanish and Portuguese individuals were an unexpected result, because the three mentioned countries share Catholic religion and traditions. The age of Italian participants, who were youngest than Spanish and Portuguese, could explain these results. The fact that Turkish participants use strategies to neutralize or control UMIs more is consistent with the differences observed between Canadian and Turkish students in terms of the greater use of control efforts by Turkish to manage OCD-related intrusions (Yorulmaz et al., 2010). In sum, our results suggest that, although cognitive models of disorders in which UMIs play a substantive role can be relatively independent of the socio-cultural background, identifying cultural factors (e.g., religious- and migration-related), might be important in implementing more accurate assessments and treatments that consider these factors.
Regarding the contents of the intrusions, the IAD-related caused the highest emotional impact, the OCD-related were the most interfering, and these two intrusive contents were the most dysfunctionally appraised, whereas the BDD and EDs-related intrusions interfered less and were appraised less dysfunctionally. Additionally, participants used thought-control strategies less when they experienced EDs-related intrusions. The findings are similar to the ones reported by Pascual-Vera and Belloch (2018b), and they suggest that having intrusions related to "fear for one's/others’ safety", as in obsession-like and health and death-related intrusions, are more easily interpreted as personally threatening, regardless of the cultural background, than intrusions related to physical appearance. The fact that EDs intrusions were the least interfering and instigated fewer control and/or neutralizing behaviors could indicate that both Western and non-Western societies have normalized the experience of having disturbing thoughts and images related to appearance, thinness, or dieting. Cultural beliefs and attitudes related to the idealization of a particular body type and a thin physical appearance, and the subsequent dissatisfaction with one's figure, have been identified as a factor leading to the development of EDs (e.g., Eli, 2018; Miller & Pumariega, 2001). However, these results might be modulated by the characteristics of our study sample: up to 80% of the participants were young women with university studies. The influence of a culture of thinness in patriarchal societies is probably predominant in all the countries in this study (Hesse-Biber et al., 2006). To further investigate this possibility, future studies may benefit from integrating feminist and transcultural theories when examining the occurrence of culture-based syndromes, such as are at least in part the EDs (Miller & Pumariega, 2001).
The present study has several limitations that could affect the interpretation of the results. First, our samples were dissimilar in size and small in the case of Iran, Israel, and Argentina. Although we collected a large representative sample, in this study we only included participants who had recently experienced the four most upsetting UMIs. Nonetheless, it is important to note that our findings are related to UMIs about each content individuals selected as the most disturbing one experienced recently, which makes these intrusions closer to those clinically significant experienced by individuals with OCD, BDD, IAD, and EDs. The age variability across countries and the fact that participants were mainly women with university studies is another limitation. Further studies are needed to guarantee the representativeness of the results. Another limitation was the possible bias associated with the use of a retrospective self-report questionnaire that might over- or underestimate the UMIs experience because UMIs can be difficult to distinguish from other cognitive products, such as ruminations, automatic thoughts, or worries (Inozu, Haciömeroglu, Keser, Akin-Sari, & Özmenler, 2021). We tried to control these difficulties by designing the QUIT on the basis of previously validated self-report measures.
In conclusion, the occurrence of UMIs typically related to OCD, BDD, IAD, and EDs is not restricted to a specific culture or socio-cultural context, although these intrusions differ in their expressive phenomenology (i.e., contents, prevalence, frequency, and discomfort rates) and in the maladaptive consequences linked to them (Pascual-Vera et al. (in press) Our findings suggest that cognitive models of disorders such as OCD, BDD, IAD, and EDs, although seem to be relatively free of cultural influences, should incorporate social and culturally-relevant constructs that would allow to make culturally-specific predictions to increase the understanding of the role of culture and associated values and beliefs in the expression of UMIs and their associated consequences. The role of cultural factors, such as migration movements, religion or gender values, might be behind these cultural variations, but we cannot rule out the influence of more specific variables, as the age is, in our findings. Future studies should examine the weight of social context-based factors to increase the understanding of the role of culture and associated values and beliefs in the expression of UMIs and their associated consequences, as well as the influence that the specific emotional and/or affective state of respondent has on the results.
