





Background/Objective Person centered care is a novel approach which aims to improve care quality in services for older people requiring care. The aim of this work is the adaptation and validation of the Staff Assessment Person-directed Care (PDC) in a Spanish population. Method The PDC was applied to a sample of 1,339 direct care professionals from 56 elderly care homes. The psychometric properties were analyzed within the framework of Classical Test Theory and Item Response Theory models. Results The measure showed a high reliability provided by Cronbach's alpha (α = .96), the test-retest reliability (r = .88), and also an adequate Information Function (highest scores between theta values -2 and +2). The factorial structure of PDC is essentially unidimensional, and confirms the existence of two large dimensions which are in turn expressed in eight highly correlated factors. Especially notable in terms of validity evidence based on relations to others variables are the correlations of PDC with the The Person-centered Care Assessment Tool (r= .68), organizational climate (r = .67), emotional exhaustion (r= -.41) and personal accomplishment (r = .45). Conclusions The Spanish version of the PDC demonstrates adequate psychometric properties for its use in the evaluation of elderly care facilities, both for professional and research purposes.
Antecedentes/Objetivos La atención centrada en la persona es un enfoque innovador que busca mejorar la calidad asistencial de los servicios para personas mayores que precisan cuidados. Ante el creciente interés hacia este enfoque es necesario contar con instrumentos de medida que permitan evaluar en qué grado los servicios gerontológicos llevan a cabo una atención centrada en la persona. El objetivo de este trabajo es la adaptación y validación del Staff Assessment Person-directed Care (PDC) en población española. Método Se llevó a cabo la traducción y adaptación del PDC al español y se aplicó a una muestra de 1.339 profesionales de atención directa, pertenecientes a 56 residencias para personas mayores. El estudio de las propiedades psicométricas se realizó desde el marco de la Teoría Clásica de los Tests y los modelos de Teoría de Respuesta a los Ítems. Resultados El coeficiente alfa de Cronbach fue de 0,97 y el coeficiente de fiabilidad test-retest de 0,89. La Función de Información indica que la prueba mide de forma precisa para un amplio rango de puntuaciones (valores θ entre -2 y + 2). La estructura factorial del PDC es esencialmente unidimensional, confirmándose la existencia de dos grandes dimensiones que se articulan a su vez en ocho factores muy correlacionados. En cuanto a la validez predictiva destacan las correlaciones del PDC con el The Person-centered Care Assessment Tool (r= 0,68), con el clima organizacional (r = 0,67) y con los factores del burnout, agotamiento emocional (r= -0,41) y realización personal (r = 0,46). Conclusiones La versión española del PDC confirma los resultados encontrados en otras poblaciones, presentando unas excelentes propiedades psicométricas para su uso en la evaluación de residencias de personas mayores, tanto con fines profesionales como de investigación.
Modern societies are experiencing rapid and increasing ageing all over the world. Consequently, in more developed countries we are seeing a significant development of various professional care services for older people in need of care (Kinsella & Phipillips, 2005; United Nations, 2013). These circumstances have motivated both public and private administrations to control quality, and service providers to put into place processes to improve the care given to this group of people (Dewar & Nolan, 2013). In the process of expanding services traditional facilities have been the object of criticisms such as organizational rigidity, uniformity of care practices and the lack of personalization of care. These factors have a negative impact on a person's wellbeing by limiting their capacity to make decisions, follow their own life plans or live according to their own habits and preferences (Koren, 2010; Misiorski & Kahn, 2005).
The Person-Centered Care (PCC) approach arose out of this context some decades ago. It aims to integrate evidence-based practices with authentic personalization of care and support so that people can retain control over their day to day lives and decisions. In recent years the PCC approach has become established as one of the pillars of quality in elderly care services (Edvardsson, Fetherstonhaugh, & Gibson, 2010; Nolan, Davies, Brown, Keady, & Nolan, 2004). Furthermore, this approach has become a benchmark to guide the transformation of culture in elderly care facilities (Brownie & Nancarrow, 2013; Koren, 2010; Misiorski & Kahn, 2005). Historically, the origin of the PCC approach is usually attributed to Rogers (1961), however, this concept has been widely developed in various areas and services, including in relation to older people needing care, especially in the field of dementia (Brooker, 2007; Edvardsson, Winblad, & Sandman, 2008; Kitwood, 1997). Despite there being no unified definition of or consensus about this approach, most authors highlight its complexity and multidimensionality (McCormack, 2004; Nolan et al., 2004). First amongst its most often cited components are those directly related to personalized care, that is, the acknowledgement that each person is a valued individual (Brooker, 2007; Kitwood, 1997; White, Newton-Curtis, & Lyons, 2008), the awareness of the life history and lifestyle of the people being cared for (Chappell, Reid, & Gish, 2007; Edvardsson, Fetherstonhaugh et al., 2010; Edvardsson, Koch, & Nay, 2010; White et al., 2008), the promotion of personal autonomy (Chappell et al., 2007; Edvardsson, Fetherstonhaugh et al., 2010; Edvardsson, Koch et al., 2010; White el al., 2008), and organizing day to day life with meaning and significance for the subject (Kitwood, 1997; Sancho & Yanguas, 2014). In addition, dimensions have also been identified which are related to supportive surroundings, such as individualized care (Brooker, 2007; Edvardsson, Fetherstonhaugh et al., 2010; Edvardsson, Koch et al., 2010; Kitwood, 1997), the design of the physical space (Edvardsson, Fetherstonhaugh et al., 2010; Edvardsson, Koch et al., 2010; White et al., 2008), and various organizational variables (Chappell et al., 2007; Edvardsson, Fetherstonhaugh et al., 2010; Edvardsson, Koch et al., 2010; White et al., 2008). In Spain, care homes for older people are still a long way from the PCC approach (Díaz-Veiga & Sancho, 2013; Martínez, 2011, 2013; Rodríguez, 2012), nonetheless, in recent years there has been a growing interest in these models, highlighting an awareness of the need to change current services. In order to achieve this progress, rigorous evaluation of care homes will be needed in order to understand the level of person centered care provided and the support available. This will allow improvements and achievements to be reported once these models are applied. However, the development of valid tests to achieve this aim in a Spanish speaking population is very recent, and so far there are few tools which allow rigorous evaluation of how well the PCC approach is being applied (Martínez, Suárez-Álvarez, Yanguas, & Muñiz, 2015).
Various approaches to evaluate elderly care services have been suggested from the context of PCC. Amongst these are: Direct observation of care given, interviews aimed at gathering opinions from professionals, recipients of care and their families, and external evaluation of objective progress indicators (De Silva, 2014). The specialist literature recommends using a combination of these strategies and tools (De Silva, 2014; Edwardsson & Innes, 2010). Although the professional's opinions should not be the only factor to be considered in overall objective quality evaluations of care services, they are extremely important as they are the people who provide direct care and who are involved in changes that many facilities require in order to apply a PCC oriented model.
Internationally, various tools have been developed to discover the opinions of professionals who work in elderly care facilities (Edvardsson & Innes, 2010). They include: The Person-centered Care Assessment Tool (P-CAT; Edvardsson, Fetherstonhaugh et al., 2010; Edvardsson, Koch et al., 2010), The Staff Assessment Person Directed Care (PDC; White et al., 2008), The Individualizad Care (Chappell et al., 2007), and The English language Person-centered Climate Questionnaire: Staff version (Edvardsson, Koch et al., 2010). One of the most used tools internationally, which is available in various languages, including Spanish, is the P-CAT (Martínez et al., 2015). This tool evaluates three components: Personalizing Care, Organizational Support and Environmental Accessibility. The PCAT is doubtless a useful tool, but its brevity, occasionally seen as one of its strengths, becomes a weakness when the aim is to make comprehensive changes in facilities and to guide improvement processes (Rokstad, Engedal, Edwardsson, & Selbaek, 2012). For such an aim, the PDC (White et al., 2008) seems a more appropriate tool. This is because, in addition to having demonstrated appropriate psychometric properties in previous studies (Choi & Lee, 2013; Sullivan et al., 2012; White et al., 2008), its 50 items articulated in two large dimensions, which in turn are organized into eight sub-factors, are extremely useful for detailed evaluation of the homes in terms of level and type of care given, which facilitates subsequent guidance towards service improvement. The first dimension of the PDC (Person-Directed Care) includes the sub-factors of Autonomy, Personhood, Knowing the Person, Comfort Care and Support Relations, while the second (Environmental Support for Person-Directed Care) comprises the sub-factors Work with Residents, Personal Environment for Residents, and Management/Structure.
Within this context, the aim of this present work is the translation, adaptation and validation of the Spanish version of the Staff Assessment Person-Directed Care (PDC), currently one of the most used tools for the detailed evaluation of person centered care. Spanish is the third most spoken language in the world, so there is great interest in having a Spanish version of this test, which would be useful both for research and professional practice. With appropriate cultural adaptations (Muñiz, Elosua, & Hambleton, 2013), the new version of the PDC could also be used in the rest of the Spanish speaking world, where interest is growing in the field of elderly care and the provision of long term care. Moreover, previous psychometric research on the PDC has been done within the framework of Classical Test Theory (CTT), whereas our study includes recent psychometric developments within the framework if Item Response Theory (IRT), which allows a more comprehensive understanding of the psychometric functioning of the PDC.
MethodParticipantsA total of 1,339 front-line care staff (staff directly involved in care) in 56 residential care homes for the elderly agreed to participate in the study and completed the requested information. A stratified sampling method was used according to type of home (66.1% urban; 33.9% non-urban), size of facility (32.1% less than 50 residents, 30.4% between 50 and 100, 37.5% more than 100), and ownership (46.4% public, 53.6% private). In addition, given the different modes of management which exist in public residential care homes, the three most common were included: 23.2% direct management (all of the professionals are public sector employees); 23.2% indirect management (professionals subcontracted through private companies); 53.6% mixed management (professionals of both types). Care assistants made up 70.6% of the respondents, 29.4% were professionals from a range of disciplines. Some 91.5% were women and 8.5% were men. The mean age was 39.41 (SD = 10.54) ranging between 19 and 65. The average time previously spent caring for the elderly was 76.97 months (SD = 57.45) ranging from 1 to 372 months.
The criteria for including the participating centers were: a) it appears in the authorized register of residential centers in the corresponding autonomous community, b) it is a dedicated long stay center for care-dependent residents, and c) commitment to participate in the study following the conditions stipulated in the protocol. Criteria for exclusion were: a) centers exclusively for people with a high level of independence and autonomy, b) palliative care units, acute care or convalescence centers, and c) short stay units. The sample may be considered representative of the residential sector in Spain, since 14 of the 17 autonomous communities in Spain are represented in the sample.
ProcedureAfter obtaining agreement to collaborate in the study from the 56 selected centers, 1,700 questionnaires were sent by mail of which 1,339 were returned completed, a response rate of 78.76%. In each center a member of staff was designated to coordinate the administration of the measuring instruments. A protocol was produced and sent in writing to each center manager and each staff coordinator in order to communicate and standardize the test application process. This protocol included indications about which professionals should be invited, elderly care specialists and members of technical teams (i.e. medical, nursing, occupational therapy, physiotherapy, psychology, social work, social education and support), information about how to encourage maximum participation, how to organize the sessions for the professionals to be able to complete the questionnaires individually and confidentially, information about the data collection period, instructions to be read by the coordinators and also the procedure for the receipt, storage and return of the questionnaires. In addition to the evaluation tools used, sociodemographic data was also collected about the participating professionals. Individual contact was maintained with each coordinator to resolve any issues. Participation by the professionals was anonymous, voluntary and completely confidential. No compensation of any kind was offered or received for their participation. The entire process was approved and supervised by the Matia Fundazioa / Fundación Hurkoa Care Ethics Committee.
Instruments- -
The Staff Assessment Person-Directed Care (PDC). The PDC (White et al., 2008), is a tool comprising a total of 50 Likert-type items with 5 answer categories. The tool was designed to evaluate the level to which person centered care is provided in a facility as assessed by professionals directly involved in care. The tool evaluates two main dimensions: Person-Directed Care and Environmental Support for Person-Directed Care. The first dimension includes five factors, Autonomy, Personhood, Knowing the Person, Comfort Care and Support Relations; the second, Work with Residents, Personal Environment for Residents and Management/Structure. The questionnaire allows scores to be obtained in each of the main dimensions and the subscales, as well as a total score. International Test Commission guidelines for translation and adaptation of tests (Hambleton, Merenda, & Spielberger, 2005; Muñiz et al., 2013) were followed when carrying out the translation, adaptation and validation of the PDC for the Spanish population. Firstly, two independent translations of the test were obtained from two experienced translators. Once these translations were done, they were themselves checked by a group of experts who produced a first draft of the test by consensus. Following the production of this first draft in Spanish, a different experienced translator produced a back-translation into English. Then, a total of 9 experts, with experience of translating psychometric tests, evaluated the level of semantic correspondence between the original version of the test and the back-translation on a scale of 0 to 10. The average of the scores was calculated for each item and any which scored less than 7 points were revised. Following this criterion, four items were slightly modified and a second draft of the test was produced. This second draft was the subject of a pilot study by 8 participants whose main objective was to check whether they understood each item. As part of the pilot study process, some modifications were made to make the test easier to understand correctly. Finally a second pilot study was carried out, using the new version with a group of 13 professionals in an elderly care facility to ensure that the test could be applied without difficulties.
- -
The Person-centered Care Assessment Tool (P-CAT). The P-CAT is a questionnaire which contains 13 items that measure the level of development of person centered care delivered by a facility according to the personnel directly involved in care (Edvardsson, Fetherstonhaugh et al., 2010; Edvardsson, Koch et al., 2010). The items have a Likert-type format, with five answer categories where 1 means “Completely disagree” and 5 “Completely Agree”. The Spanish version of the tool has appropriate psychometric properties: The internal consistency of the scale was .88; the test-retest reliability coefficient was .79; the first factor explains 38% of the variance and appropriate evidence of validity in relation to other variables has been demonstrated (Martínez et al., 2015).
- -
Organizational Climate Scale (CLIOR). The short version of the CLIOR scale was used to evaluate the organizational climate in the care homes (Muñiz et al., 2014; Peña, Muñiz, Campillo, Fonseca, & García-Cueto, 2013). It is made up of 15 Likert-type items with five answer categories where 1 means “Completely disagree” and 5 “Completely Agree”. The instrument has appropriate psychometric properties (α=.94; the first factor explains 52.32% of the variance) and allows the evaluation of the organizational climate as perceived by the workers.
- -
Maslach Burnout Inventory (MBI). With the aim of being able to measure the level of burnout in the sample of professionals who took part in the study, the Spanish version (Seisdedos, 1997) of the MBI questionnaire (Maslach & Jackson, 1986) was used. This tool measures burnout experienced by professionals with a 22 item Likert-type scale with 7 answer categories. It distinguishes three components emotional exhaustion (α = .88; 9 items), depersonalization (α = .56; 5 items), and personal accomplishment (α=.75; 8 items). High scores in the first two components and low scores in the third define burnout syndrome. According to results published in the meta-analysis by Aguayo, Vargas, de la Fuente, and Lozano (2011), the reliability coefficients found in previous studies have a mean alpha coefficient of .88, .71 and .78 for each dimension respectively.
Firstly, a Confirmatory Factor Analysis (CFA) was carried out within the framework of Structural Equation Modelling in order to study the factorial structure of the instrument. A robust weighted least squares estimator (WLSMV) was used, indicated for categorically ordered data (Muthén & Muthén, 2010). The goodness of fit of the data to the model was evaluated using the χ2, the Comparative Fit Index (CFI), the Tucker Lewis Index (TLI), and the Root Mean Square Error of Approximation (RMSEA). The literature suggests that the fit is adequate when the χ2/df < 5, CFI>.90, TLI>.90, and the RMSEA<.08 (Kline, 2011).
After defining the factorial structure that best represents the data, the differential item functioning (DIF) of the items on the basis of gender was examined, using the logistical regression method (Gómez-Benito, Hidalgo, & Zumbo, 2013). The reliability coefficient was estimated using the Cronbach alpha coefficient for ordinal data (Elosua & Zumbo, 2008) and the test-retest reliability using a subsample of 118 professionals working in adult day care centers. Samejima's Graded Response Model within the Item Response Theory (IRT) framework was used to calculate the Information Function of the PDC. In order to examine the evidence of validity in relation to other variables, the Spearman correlation coefficients between the PDC, the Person-centered Assessment Tool (P-CAT), burnout (MBI) and organizational climate (CLIOR) were calculated. Given the small number of missing values (less than 5%), those cases were eliminated in order to perform the analysis, as their influence on the results is considered irrelevant (Cuesta & Fonseca, 2014; Fernández-Alonso, Suárez-Álvarez, & Muñiz, 2012). The data was analyzed using the statistical software packages SPSS 19, MULTILOG 7, and MPLUS 6.
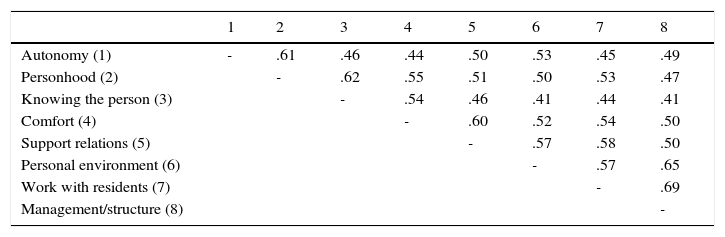
ResultsDimensionalityThe factorial structure of the PDC is initially made up of two dimensions and eight more specific facets (Figure 1). The Confirmatory Factor Analysis fit indexes give χ2 = 5786.84 (df = 1166; p < .001; χ2/df = 4.96), a CFI = .915, a TLI = .911, and a RMSEA = .057 (90% IC = .056 - .059). These results indicate that the fit of the data to the model is adequate (Kline, 2011) and confirms the factorial structure of the original version in the Spanish population (White et al., 2008). The correlation between the Person-Directed Care and Environment dimensions was .82. The high correlation found between both dimensions as well as the high covariation between the eight factors (Table 1) allows the Spanish version of the PDC to be interpreted as an essentially unidimensional structure, and as such, it is appropriate to use a total score from the scale. Furthermore, carrying out a Factorial Analysis with the 50 test items together gives a GFI = .95 and an RMSR = .087.

Spearman correlations between the eight dimensions of the Person-directed Care questionnaire (PDC).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| Autonomy (1) | - | .61 | .46 | .44 | .50 | .53 | .45 | .49 |
| Personhood (2) | - | .62 | .55 | .51 | .50 | .53 | .47 | |
| Knowing the person (3) | - | .54 | .46 | .41 | .44 | .41 | ||
| Comfort (4) | - | .60 | .52 | .54 | .50 | |||
| Support relations (5) | - | .57 | .58 | .50 | ||||
| Personal environment (6) | - | .57 | .65 | |||||
| Work with residents (7) | - | .69 | ||||||
| Management/structure (8) | - |
Note. All correlations are statistically significant at p < .001
The study of Differential Item Functioning by gender was performed using the logistical regression method on all of the items making up the PDC questionnaire. In order to reduce type I errors the statistical test (p<.01) was used together with the effect size (R2>.035). No items demonstrated differential functioning in terms of the respondent's gender.
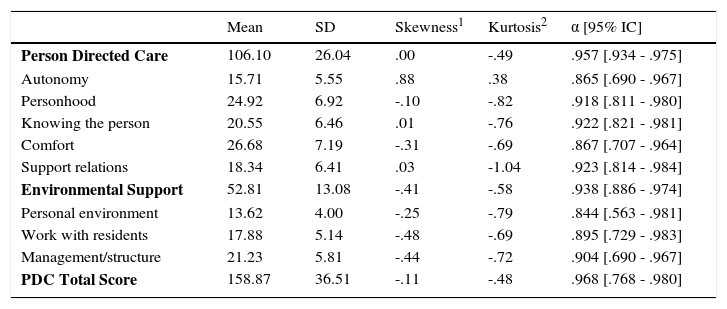
ReliabilityThe ordinal Cronbach's alpha for PDC total scores was .96, for the Person Directed Care dimension it was .95 and for Environmental Support it was .93. As can be seen in Table 2, the internal consistency of the subscales varied between .85 (Personal Environment) and .93 (Support Relations). A group of 118 professionals from 14 day care centers were used to evaluate test-retest reliability. The PDC questionnaire was given twice to this group with a minimum of one week between tests. The test-retest reliability coefficient was .88. Regarding the P-CAT, the reliability coefficient for the sample used in this study was .96 and the first factor explains 55.74% of the variance.
Descriptive statistics and internal consistency of the PDC dimensions.
| Mean | SD | Skewness1 | Kurtosis2 | α [95% IC] | |
|---|---|---|---|---|---|
| Person Directed Care | 106.10 | 26.04 | .00 | -.49 | .957 [.934 - .975] |
| Autonomy | 15.71 | 5.55 | .88 | .38 | .865 [.690 - .967] |
| Personhood | 24.92 | 6.92 | -.10 | -.82 | .918 [.811 - .980] |
| Knowing the person | 20.55 | 6.46 | .01 | -.76 | .922 [.821 - .981] |
| Comfort | 26.68 | 7.19 | -.31 | -.69 | .867 [.707 - .964] |
| Support relations | 18.34 | 6.41 | .03 | -1.04 | .923 [.814 - .984] |
| Environmental Support | 52.81 | 13.08 | -.41 | -.58 | .938 [.886 - .974] |
| Personal environment | 13.62 | 4.00 | -.25 | -.79 | .844 [.563 - .981] |
| Work with residents | 17.88 | 5.14 | -.48 | -.69 | .895 [.729 - .983] |
| Management/structure | 21.23 | 5.81 | -.44 | -.72 | .904 [.690 - .967] |
| PDC Total Score | 158.87 | 36.51 | -.11 | -.48 | .968 [.768 - .980] |
Note. SD = Standard deviation; α = Ordinal Cronbach's Alpha; 1 Standard Error = .07; 2Standard Error = .14
Table 2 also shows the descriptive statistics of all of the subscales in the PDC. The mean total in the PDC was 158.87 (SD = 36.51). Given that the theoretical range of scores is between 50 and 250 it should be noted that the respondents tended to score the items above the theoretical mean (150). In addition, the distribution of the total scores does not show any significant asymmetry although it does show issues of kurtosis. Dimensions which are notable for being especially asymmetrical include Autonomy (positive skew), Work with residents (negative skew), and Management/Structure (negative skew), and the Personhood and Support relations dimension for their negative kurtosis. The indices of discrimination for the items calculated through item-test correlation varied between .27 and .70 with a mean of .55.
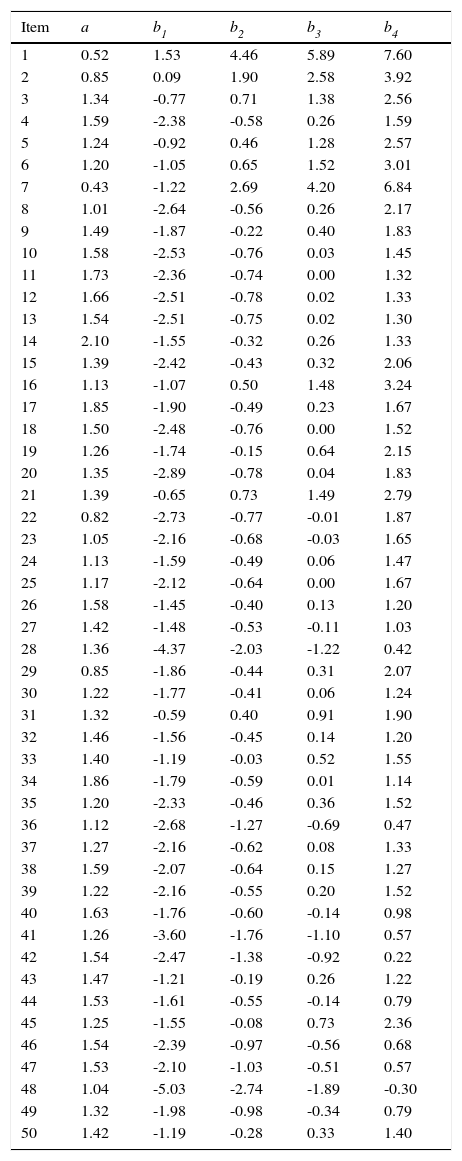
Item Response Theory AnalysisTable 3 shows the parameters of discrimination (a) and difficulty (b1-b4) for the 50 items of the PDC. In general, the items showed moderate levels of discrimination (Baker, 2001). The difficulty parameters presented in Table 3 indicate that the items are measuring appropriately for low and medium ability levels of the different personality traits.
Item Response Theory parameter estimates for the PDC.
| Item | a | b1 | b2 | b3 | b4 |
|---|---|---|---|---|---|
| 1 | 0.52 | 1.53 | 4.46 | 5.89 | 7.60 |
| 2 | 0.85 | 0.09 | 1.90 | 2.58 | 3.92 |
| 3 | 1.34 | -0.77 | 0.71 | 1.38 | 2.56 |
| 4 | 1.59 | -2.38 | -0.58 | 0.26 | 1.59 |
| 5 | 1.24 | -0.92 | 0.46 | 1.28 | 2.57 |
| 6 | 1.20 | -1.05 | 0.65 | 1.52 | 3.01 |
| 7 | 0.43 | -1.22 | 2.69 | 4.20 | 6.84 |
| 8 | 1.01 | -2.64 | -0.56 | 0.26 | 2.17 |
| 9 | 1.49 | -1.87 | -0.22 | 0.40 | 1.83 |
| 10 | 1.58 | -2.53 | -0.76 | 0.03 | 1.45 |
| 11 | 1.73 | -2.36 | -0.74 | 0.00 | 1.32 |
| 12 | 1.66 | -2.51 | -0.78 | 0.02 | 1.33 |
| 13 | 1.54 | -2.51 | -0.75 | 0.02 | 1.30 |
| 14 | 2.10 | -1.55 | -0.32 | 0.26 | 1.33 |
| 15 | 1.39 | -2.42 | -0.43 | 0.32 | 2.06 |
| 16 | 1.13 | -1.07 | 0.50 | 1.48 | 3.24 |
| 17 | 1.85 | -1.90 | -0.49 | 0.23 | 1.67 |
| 18 | 1.50 | -2.48 | -0.76 | 0.00 | 1.52 |
| 19 | 1.26 | -1.74 | -0.15 | 0.64 | 2.15 |
| 20 | 1.35 | -2.89 | -0.78 | 0.04 | 1.83 |
| 21 | 1.39 | -0.65 | 0.73 | 1.49 | 2.79 |
| 22 | 0.82 | -2.73 | -0.77 | -0.01 | 1.87 |
| 23 | 1.05 | -2.16 | -0.68 | -0.03 | 1.65 |
| 24 | 1.13 | -1.59 | -0.49 | 0.06 | 1.47 |
| 25 | 1.17 | -2.12 | -0.64 | 0.00 | 1.67 |
| 26 | 1.58 | -1.45 | -0.40 | 0.13 | 1.20 |
| 27 | 1.42 | -1.48 | -0.53 | -0.11 | 1.03 |
| 28 | 1.36 | -4.37 | -2.03 | -1.22 | 0.42 |
| 29 | 0.85 | -1.86 | -0.44 | 0.31 | 2.07 |
| 30 | 1.22 | -1.77 | -0.41 | 0.06 | 1.24 |
| 31 | 1.32 | -0.59 | 0.40 | 0.91 | 1.90 |
| 32 | 1.46 | -1.56 | -0.45 | 0.14 | 1.20 |
| 33 | 1.40 | -1.19 | -0.03 | 0.52 | 1.55 |
| 34 | 1.86 | -1.79 | -0.59 | 0.01 | 1.14 |
| 35 | 1.20 | -2.33 | -0.46 | 0.36 | 1.52 |
| 36 | 1.12 | -2.68 | -1.27 | -0.69 | 0.47 |
| 37 | 1.27 | -2.16 | -0.62 | 0.08 | 1.33 |
| 38 | 1.59 | -2.07 | -0.64 | 0.15 | 1.27 |
| 39 | 1.22 | -2.16 | -0.55 | 0.20 | 1.52 |
| 40 | 1.63 | -1.76 | -0.60 | -0.14 | 0.98 |
| 41 | 1.26 | -3.60 | -1.76 | -1.10 | 0.57 |
| 42 | 1.54 | -2.47 | -1.38 | -0.92 | 0.22 |
| 43 | 1.47 | -1.21 | -0.19 | 0.26 | 1.22 |
| 44 | 1.53 | -1.61 | -0.55 | -0.14 | 0.79 |
| 45 | 1.25 | -1.55 | -0.08 | 0.73 | 2.36 |
| 46 | 1.54 | -2.39 | -0.97 | -0.56 | 0.68 |
| 47 | 1.53 | -2.10 | -1.03 | -0.51 | 0.57 |
| 48 | 1.04 | -5.03 | -2.74 | -1.89 | -0.30 |
| 49 | 1.32 | -1.98 | -0.98 | -0.34 | 0.79 |
| 50 | 1.42 | -1.19 | -0.28 | 0.33 | 1.40 |
Note. a = IRT discrimination parameters; b1, b2, b3, b4 = IRT difficulty parameters.
The Information Function was estimated to evaluate the precision of the PDC for different levels of the measured variable (θ), and so to complement the more overall information provided by the alpha coefficient. In Figure 2 the solid line represents the information provided by the test and the dotted line represents the Standard Error. As can be seen, the PDC gives the best precision for values of theta (θ) between -2 and +2.
Validity evidence based on relations to other variables
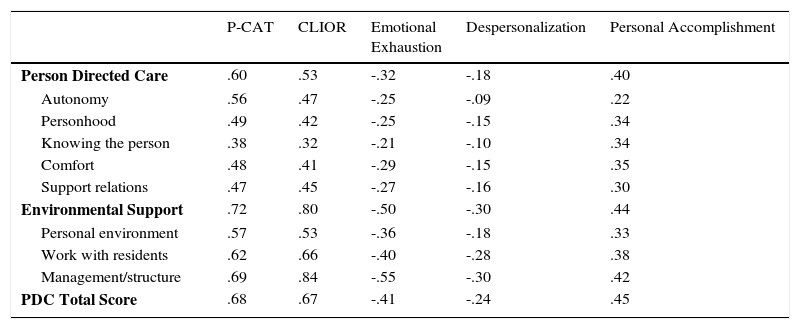
Table 4 shows the Spearman correlations between PDC scores and those obtained in the Person-centered Care Assessment Tool (P-CAT), organizational climate (CLIOR), and the three Burnout dimensions (emotional exhaustion, depersonalization, and personal accomplishment). The results show that the scores converge in the expected direction, highlighting the clear correlation between the PDC and the P-CAT (r = .68), and between the PDC and organizational climate (r = .67). The percentage of associated variance between the total PDC and the P-CAT as well as between the total PDC and organizational climate was found to be around 50%. This data would indicate an elevated effect size. However, the percentage of associated variance between the total PDC and the burnout dimensions show a smaller effect size, in the region of 20%, and is especially low in depersonalization (lower than 10%).
Spearman correlations between the dimensions of Person-Directed Care questionnaire (PDC), the Person-centered Care Assessment Tool (P-CAT), the Organizational Climate scale (CLIOR), and three subscales of Burnout (MBI).
| P-CAT | CLIOR | Emotional Exhaustion | Despersonalization | Personal Accomplishment | |
|---|---|---|---|---|---|
| Person Directed Care | .60 | .53 | -.32 | -.18 | .40 |
| Autonomy | .56 | .47 | -.25 | -.09 | .22 |
| Personhood | .49 | .42 | -.25 | -.15 | .34 |
| Knowing the person | .38 | .32 | -.21 | -.10 | .34 |
| Comfort | .48 | .41 | -.29 | -.15 | .35 |
| Support relations | .47 | .45 | -.27 | -.16 | .30 |
| Environmental Support | .72 | .80 | -.50 | -.30 | .44 |
| Personal environment | .57 | .53 | -.36 | -.18 | .33 |
| Work with residents | .62 | .66 | -.40 | -.28 | .38 |
| Management/structure | .69 | .84 | -.55 | -.30 | .42 |
| PDC Total Score | .68 | .67 | -.41 | -.24 | .45 |
Note. All correlations are statistically significant at p < .001
The Staff Assessment Person Directed Care (PDC) developed by White et al. (2008) is one of the most commonly used tools internationally for the evaluation of care in elderly care homes focusing on the person centered care (PCC) approach. In general assessment, the PDC tool has been shown to have appropriate psychometric properties both in the North American population (Sullivan et al., 2012; White et al., 2008) and in its South Korean adaptation (Choi & Lee, 2013). The original version of the tool (White et al., 2008) identified a structure composed of two main dimensions expressed in eight factors assessed in a sample of 420 direct-care professionals from seven care homes and one home care service. The five factors which make up the first dimension explain 61% of the variance and their Cronbach alpha coefficients varied between .86 (Autonomy; Personhood) and .91 (Knowing the person; Support relations). The three remaining factors which make up the second dimension explain 60% of the variance and their Cronbach alpha coefficients ranged from .74 (Personal environment) to .86 (Management). A second study, carried out by Sullivan et al. (2012), also in a population of North American care homes, confirmed the discriminant and convergent validity of the 50 proposed items in the original as well as the 8 factor factorial structure. The Cronbach alpha coefficients in this study ranged between .84 (Personal environment) and .91 (Support relations; Personhood; Knowing the person). A third study by Choi and Lee (2012) was carried out in a South Korean population following translation and cultural adaptation of the original items, although in this case it was the director or manager of the center who answered the questionnaire. These authors ended by proposing a reduced version of the PDC, adapted for the population of residential care homes in South Korea. The Korean version of the PDC is composed of a total of 30 items which are grouped in seven factors, eliminating the Personal Environment factor that the original scale had in the Environment Support dimension, a decision that the authors based on the existence of cultural differences in the concept of this component. The Cronbach alpha coefficients of this version were between .70 (Autonomy) and .84 (Organization).
In the case of the Spanish version of the PDC, the results have confirmed the original structure of eight factors suggested by White et al. (2008). The reliability coefficients of the factors are in line with those found in previous studies with the Autonomy dimension having the lowest Cronbach alpha coefficient and Support relations having the highest (Choi & Lee, 2013; White et al., 2008). Given the high covariation between the dimensions as well as between the eight factors it seems reasonable to conclude that the structure which best represents the data is essentially unidimensional. In fact, carrying out a Factorial Analysis with the 50 test items together gives a GFI = .95 and an RMSR = .087, which supports the idea of unidimensionality. Furthermore the high internal consistency of the scale (α =.98) must be emphasized, as well as the high temporal stability coefficient (test-retest reliability = .88). This raises the possibility of obtaining a total score of person-centered care in addition to scores for each of the two dimensions and eight factors. In addition, the psychometric properties of the items in the Spanish version of the PDC were appropriate. No items demonstrated differential functioning in terms of gender and all items had acceptable discriminative power, both within Classical Test Theory and Item Response Theory frameworks. The Spanish version of the PDC maintains the composition of the 50 items proposed in the original. With regard to the evidence of validity in relation to other variables, the Spanish version of the PDC demonstrated adequate convergent validity with the tests used. It is especially important to highlight the clear relation found between the PDC and the PCAT (r = .68). This is not a surprising result as both tools evaluate person-centered care (Martínez et al., 2015). Likewise, the clear correlation between the PDC and organizational climate (r = .67) is worthy of note. While bearing in mind that correlational techniques do not allow causality to be established, it seems reasonable to think that the organizational climate can work in both directions, on the one hand as a facilitating precondition of PCC, given the high involvement that the application of this approach requires from professionals, and a the same time as a positive effect of this care approach. These data are in line with those found in various research, which link care models oriented towards PCC with better satisfaction on the part of the professionals with their work and a significant reduction in stress (Dilley & Geboy, 2010; Edvardsson, Sandman, & Borell, 2014; McCormack et al., 2010; Passalacqua & Harwood, 2012; Van del Pol-Grevelink, Jukema, & Smits, 2012). The practical implication of these results will doubtless be of interest for managing change and implementation of PCC models in existing centers.
With respect to Burnout, the PDC has negative correlation with the emotional exhaustion (r = -.41) and depersonalization (r = -.24) factors, and a slight positive correlation with the personal accomplishment factor (r = .45). These results are in line with expectations as PCC requires motivated professionals and, at the same time, drives towards work which is distinguished by more autonomy and responsibility on the part of the elderly care workers, and by closer, more humane treatment of service users, characteristics which can act as preventative factors in burnout (De la Fuente et al., 2015; Hayajneh & Shehadeh, 2014; Passalacqua & Harwood, 2012; Schrijnemaekers et al., 2003; Van del Pol-Grevelink et al., 2012; Vargas, Cañadas, Aguayo, Fernández, & De la Fuente, 2014).
In summary, the results confirm that the Spanish version of the PDC demonstrates adequate psychometric properties according to the standards established in the specialist literature (Evers et al., 2013). Furthermore, the tool provides precise measurement over a wide range of scores (ϴ values between -2 and + 2), within which one would expect to find the majority of people if the scores are normally distributed. Therefore the PDC can be considered of great use in the evaluation of person-centered care in elderly care homes. This test, as opposed to other, shorter tests such as the P-CAT, may be especially useful for reviewing services and establishing care priorities to direct change as well as to analyze more deeply the effects of interventions in distinct parts of PCC models or the relationship between them. The results must be interpreted in light of some limitations. The first, and most significant, is that the data obtained through the PDC questionnaire come from the opinions of the professionals providing care to the residents. While they are very important opinions, they should be complemented in the future by the addition of other data from other sources in order to achieve a more complete view of the activity in the centers. In addition, it must be borne in mind that the control of test administration was through the coordinators working in that same center. While no behavior was detected which might suggest malpractice and which would put data quality in doubt thanks to the sample size and the direct contact maintained with each test coordinator in each center, in future it would be beneficial to have better control over test administration. Secondly, the data was collected at a specific period in time, it would be useful to carry out some kind of longitudinal study to be able to evaluate change over time.
This research was funded by the Spanish Ministry of Economy and Competitiveness. References: PSI2014-56114-P, BES2012-053488, and IB-05-02. We would like to express our utmost gratitude to the following public and private institutions, without whose collaboration this research would not have been possible: Consejería de Bienestar Social y Vivienda del Principado de Asturias, Ayuntamiento de Madrid, Instituto de Atención Social y Sociosanitaria de Canarias, Instituto Mallorquín de Asuntos Sociales, Consejería de Trabajo y Bienestar de la Xunta de Galicia, Instituto Foral de Bienestar Social de Vitoria, Consorci d’Accio Social de Catalunya, Gerencia de Servicios Sociales de Castilla y León, LARES Federación, NOVAIRE, EULEN SOCIOSANITARIOS, INTRESS, Asociación Madrileña de Atención a la Dependencia (AMADE), ASISPA, L’ONADA, Fundación MATÍA, SARAIVA, IDEA, Fundación Vallparadís-Mutua Terrassa, Residencia Sierra Cuera (Asturias), Residencia El Olivaret (Barcelona), Residencia La Quintana (Asturias), Residencia Torrezuri (País Vasco) y Residencia Santa Agueda (País Vasco).
