



Given the negative consequences of weight bias, including internalized weight stigma, on health outcomes, two instruments—the Weight Self-Stigma Questionnaire (WSSQ) and Weight Bias Internalization Scale (WBIS)—have been developed. However, their psychometric properties are yet to be tested for Asian pediatric populations. Method:Participants aged 8 to 12 years (N=287; 153 boys) completed the WSSQ and the WBIS, and they were classified into either a group with overweight or a group without overweight based on self-reported weight and height. Results:Both WSSQ and WBIS had their factor structures supported by confirmatory factor analyses (CFAs). The measurement invariance of two-factor structure was further supported for WSSQ across gender and weight status. The measurement invariance of single-factor structure was supported for WBIS across gender but not across weight status. Conclusions:WSSQ and WBIS were both valid to assess the internalization of weight bias. However, the two instruments demonstrated different properties and should be applied in different situations.
Dadas las consecuencias negativas del sesgo de peso, incluyendo el estigma de peso internalizado, sobre los resultados de salud, se han desarrollado dos instrumentos -el Weight Self-Stigma Questionnaire (WSSQ) y la Weight Bias Internalization Scale (WBIS)-. Método:Los participantes de 8 a 12 años de edad (N=287; 153 varones) completaron el WSSQ y la WBIS, y fueron clasificados en un grupo con sobrepeso o un grupo sin sobrepeso basado en el peso y la altura autoinformados. Resultados:Tanto en el WSSQ como en la WBIS se confirmaron sus estructuras factoriales mediante análisis factoriales confirmatorios (CFAs). La invarianza de la medida de la estructura de dos factores fue más apoyada para el WSSQ a través del género y del estado del peso. La invarianza de la medida de la estructura unifactorial fue apoyada para la WBIS a través de género, pero no a través de estado del peso. Conclusiones:WSSQ y WBIS son instrumentos válidos para evaluar la internalización del sesgo de peso. Sin embargo, los dos instrumentos demostraron diferentes propiedades y deben aplicarse en diferentes situaciones.
Being overweight and obese are considered to be most important multifaceted public health problems associated with multiple health impairments, including psychological problems, elevated blood pressure, type 2 diabetes, asthma, hepatic steatosis, cardiovascular disease and high cholesterol (C. -T. Lee et al., 2018; Y. -C. Lin, Latner, Fung, & Lin, 2018). Moreover, childhood obesity is a very common, increasing problem worldwide. For example, the prevalence of overweight and obesity has increased to 18.7% among primary students in Hong Kong (Wong et al., 2018). In addition to the physical health of children, childhood overweight and obesity are associated with their mental and social health. Children with obesity and overweight may experience negative social attitudes, stigma and prejudice, and are exposed to weight stigmatization in all domains of life, including education, treatment adherence, physical activity, personal relationships and even healthcare utilization (Puhl & King, 2013). Unfortunately, children with overweight or obesity are perceived as unattractive playmates who were stigmatized; that is, their peers describe them as “ugly,” “lazy,” and “stupid” (Puhl & King, 2013). Experiencing overweight and obesity among children significantly impairs their quality of life even worse than their age-matched counterparts with cancer (Schwimmer, Burwinkle, & Varni, 2003).
Stigma is a multidimensional concept and can be described as the degrees to which individuals with overweight or obesity are exposed to discrimination, prejudice, and stereotypes (C. -Y. Lin, 2019; C. -Y. Lin et al., 2019; Wong et al., 2018). Enacted stigma refers to the actual experiences of discrimination in social life by a child with overweight or obesity. Despite growing number of studies in the literature demonstrating the medical outcomes of overweight and obesity among children, studies investigating stigma, bias, and discrimination as a result of overweight and obesity are still scarce, especially in East Asia. These problems can result in psychological, social, and behavioral impairments including low self-esteem, anxiety, depression, body dissatisfaction, unsatisfactory academic performance, poor peer relationship, and eating disorders (Harriger & Thompson, 2012; Lucena-Santos, Carvalho, Oliveria, & Pinto-Gouveia, 2017). Furthermore, weight stigma and teasing by peers are prevalent not only among those with overweight and obesity, but also across different weight categories (M. Y. Cheng et al., 2018; Jendrzyca & Warschburger, 2016). Both weight bias and anti-fat attitudes could be negatively internalized in children with overweight or obesity; this increases the risk of social marginalization (Durso & Latner, 2008; Ratcliffe & Ellison, 2015).
Internalization of weight bias is a different construct from anti-fat attitudes. Specifically, anti-fat attitude is a negative evaluation given by others; internalization of weight bias is a negative evaluation by one's self (O. Y. Cheng et al., 2019). Therefore, the source of evaluation is different in these measures. This distinction is very important for predicting negative psychological outcomes among children with overweight and obesity; thus, those with internalized weight bias would report more concerns on body image, depression, anxiety, stress and self-esteem as well as eating disturbances (Durso & Latner, 2008). The sources of weight bias and stigma are peers, friends, parents and other family members, teachers, healthcare professionals, and social media (Puhl & Heuer, 2009). Therefore, children are at risk of stigmatization for overweight and obesity in several settings: home, neighborhoods, schools and clinical settings. The possible mechanisms of the effects of weight stigma on children's outcomes could be explained by some mediators. In a theoretical framework, Tylka et al. (2014) found that weight stigma leads to internalized weight stigma, and that internalized weight stigma further shapes body shame, and finally that body shame deteriorates psychological well-being. Internalized weight stigma can be maintained by several factors including negative self-judgments about the meaning of being a child with obesity, attention and mood shifts, and avoidance and safety behaviors as well as eating and weight management behaviors (Ratcliffe & Ellison, 2015).
Two self-reported measures have been developed to assess internalized weight stigma: the Weight Self-Stigma Questionnaire (WSSQ; Lillis, Luoma, Levin, & Hayes, 2010) and the Weight Bias Internalization Scale (WBIS; Durso & Latner, 2008). The WSSQ was originally developed for assessing self-devaluation and fear of enacted stigma among adults with overweight and obesity. Several studies have confirmed the psychometric characteristics of the WSSQ among Turkish, German and Chinese adults with overweight and obesity (Hain et al., 2015; K. P. Lin & Lee, 2017; Sevincer, Kaya, Bozkurt, Akin, & Kose, 2017). In a study, the French version of the WSSQ was also assessed and confirmed in adolescents with overweight and obesity (Maïano, Aimé, Lepage, ASPQ Team, & Morin, 2017). On the other hand, WBIS was developed to assess self-devaluation of being overweight and obese. The WBIS has shown good psychometric properties among different populations including adolescents and adults (Hilbert et al., 2014). There is still a lack of evidence regarding the applicability of both WSSQ and WBIS among children. Although WSSQ and WBIS have been validated in adolescents, some key differences between children and adolescents affect their impetrations of weight stigma. The transition from child to adolescent is evidenced by several important changes including biological, psychological, and social (C. -T. Lee, Tsai, Lin, & Strong, 2017). Therefore, the results of studying adolescents may not be generalizable for children. To the best of our knowledge, only one other paper describes the validation of WBIS among children (Zuba & Warschburger, 2018). However, measurement invariance of the WBIS across gender and weight status has yet to be investigated. Assessing measurement invariance can help to ensure that the subpopulations (e.g., boys and girls in the present study) have equivalent meaning (Strong, Lin, Tsai, & Lin, 2017).
In addition, we found no studies examining the psychometric properties of the WSSQ among children. Therefore, the psychometric comparisons between WBIS and WSSQ are unclear among pediatric populations. The aim of the current study was to evaluate and compare factor structure and measurement invariance between the WBIS and WSSQ among a sample of children in Hong Kong. We hypothesized that both WBIS and WSSQ strongly correlated each other and were significantly associated with psychological outcomes (e.g., quality of life) (Hübner et al., 2016).
MethodParticipants and ProcedureThe study proposal was approved by the Human Subjects Ethic Review Board of The Hong Kong Polytechnic University before data collection. We contacted several primary schools and non-governmental organizations (NGOs) in Hong Kong to explain the study purpose to them. Two schools and two NGOs expressed interest in assisting us to recruit participants. The school teachers and NGO staff helped us provide study information to the potential participants and their parents. If both participants and parents were interested in this study, they were invited to sign a written informed consent to ensure their willingness to participate. The children were also asked to complete a series of questionnaires under the supervision of school teachers or research assistants.
The inclusion criteria for the participating children included: (1) between 8 and 12 years of age; (2) had the ability to understand traditional Chinese characters; (3) studying in a primary school in Hong Kong; (4) children and their parents voluntarily agreed to participate in this study. The exclusion criteria included: (1) children who were diagnosed with cognitive impairment or neurological diseases, such as autism spectrum disorder, attention-deficit/hyperactivity disorder, and intellectual disability; (2) children who had any physical disability, such as amputation or crippled legs. Moreover, all the children were classified as with overweight or without overweight (i.e., non-overweight) based on Hong Kong norms (So et al., 2008).
InstrumentsWeight Self-Stigma Questionnaire (WSSQ). The WSSQ is a 12-item questionnaire that measures weight-related self-stigma. The scale asks participants to rate how much they agree with each statement as it applies to them on a 5-point Likert-type scale and provides scores in two domains (self-devaluation and fear of enacted domains). Both self-devaluation and fear of enacted domains (e.g., “I caused my weight problems”) have six item each, and have satisfactory internal consistency (α=.81 and .87) (Lillis et al., 2010). A higher score in the WSSQ indicates a higher level of weight-related self-stigma.
Weight Bias Internalization Scale (WBIS). The WBIS is an 11-item questionnaire that measures weight-related self-stigma. The scale asks participants to rate how much they agree with each statement as it applies to them on a 5-point Likert-type scale and provides scores in only one domain (e.g., “I hate myself for being overweight”). The WBIS has satisfactory internal consistency (α=.90; Durso & Latner, 2008). However, as suggested by the developer, the translated WBIS used “weight” to replace “overweight” in its Chinese version. For example, the aforementioned sample item is “I hate myself because of my weight” in the Chinese WBIS. A higher score in the WBIS indicates a higher level of weight-related self-stigma.
Perceived Weight Discrimination (PWD). The PWD is a 10-item questionnaire that measures perceived weight discrimination (or experienced weight stigma) using dichotomous items (yes scores 1 and no scores 0). The questionnaire was adapted from the studies of Schafer and Ferraro (2011) and Williams, Yu, Jackson, and Anderson (1997). We summed up the scores of the 10 items; a higher score indicated a higher level of perceived weight discrimination.
Kid-KINDL. The Kid-KINDL is a 24-item questionnaire that measures generic quality of life (QoL) for children between 8 and 12 years of age. The scale asks participants to rate how much they agree with each statement as it applies to them on a 5-point Likert-type scale, and the score is usually converted into a 0-100 scale; a higher score indicates a better QoL (C. -T. Lee, Lin, Tsai, Strong, & Lin, 2016; Ravens-Sieberer & Bullinger, 1998). The 24 items are distributed into the six domains each with four items: physical well-being, emotional well-being, self-esteem, Friends, family, and school (Pakpour et al., 2019). P. L. Chan, Ng, and Chan (2014) and Y. Chan et al. (2017) confirmed the adequacy of the internal consistency (α=.77 to .85).
Sizing Me Up. The Sizing Me Up is a 22-item questionnaire that measures weight-related QoL for children using the stem sentence of “…because of your weight/shape/size.” The scale asks participants to rate how much they agree with each statement as it applies to them on a 4-point Likert-type scale, and the score is usually converted into a 0-100 scale; a higher score indicates a better QoL (Pakpour et al., 2019; Zeller & Modi, 2009). The 22 items are distributed into the domains of Emotion (4 items), Physical (5 items), Teasing/marginalization (2 items), Positive attributes (6 items), and Social avoidance (5 items). Zeller and Modi (2009) and Strong et al. (2017) confirmed the adequacy of the internal consistency (α=.62 to .88).
Translation procedure for the WSSQ and WBISAfter obtaining permission from the developers to translate WSSQ (from Dr. Lillis) and WBIS (from Prof. Latner), we adopted a standard translation procedure to ensure their linguistic validity including forward translation, back translation, and reconciliation (Y. -C. Lin, Strong, Tsai, Lin, & Fung, 2018). In the first stage, two Hong Kong Chinese translators who were fluent in English and with a bachelor's degree in psychology independently translated two forward versions. The corresponding author then worked with a research assistant with a bachelor's degree in psychology to reconcile the two forward translations. A mainland Chinese translator who had been living in the U.S. in an immersion program for one year back-translated the reconciled translation. The developer of WBIS, Prof. Latner, provided additional comments on revision after comparing the back-translation to the original version. The final translated versions of the WSSQ and WBIS were circulated among a panel consisting of a psychometrician, a pediatrician, and an assistant professor in public health to ensure their readability. Afterward, five children aged between 8 and 12 (two males and three females) read the translated WSSQ and WBIS, and all indicated that they could fully understand all the items. In addition, the wordings of “overweight” were revised to “weight” throughout the WBIS as recommended by Prof. Latner during the translation process; a sample item is provided in the Weight Bias Internalization Scale section.
Data analysisWe used mean and standard deviation (SD) to present the descriptive statistics for age, self-stigma, and QoL for all participants, and to present the frequency and percentage for gender and perceived weight discrimination. In terms of psychometric testing, we first conducted two confirmatory factor analyses (CFAs) to test the factor structures of WSSQ (two-factor structure) and WBIS (one-factor structure). Because the skewness and kurtosis values of the WSSQ and WBIS items scores were not extreme (skewness in WSSQ items: 0.52 to 1.53; kurtosis in WSSQ items: -0.92 to 1.97; skewness in WBIS items: -0.70 to 1.35; kurtosis in WBIS items: -1.22 to 1.10), we applied robust maximum likelihood in the CFA. In addition, a comparative fit index (CFI), Tucker-Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR) were adopted to determine the data-model fit: CFI and TLI>.90 together with RMSEA and SRMR<.08 indicate satisfactory fit (C. -C. Chang, Su, & Lin, 2016; C. -Y. Lin, Updegraff, & Pakpour, 2016; C. -Y. Lin, Wang, Pai, & Ku, 2017; Su, Yang, & Lin, 2017).
After verifying the factor structures, we applied multigroup CFA (MGCFA) to examine the measurement invariance for both WSSQ and WBIS across gender (boys vs. girls) and weight status (overweight vs. non-overweight). The MGCFA contained three models: configural model, which simply separated the sample into two subgroups (boys and girls, or overweight and non-overweight) and did not constrain any coefficients between subgroups; metric invariance model, which constrained the factor loadings being equal across subgroups; scalar invariance model, which constrained both factor loadings and item intercepts being equal across subgroups (C. -Y. Lin, Strong, Tsai, & Lee, 2017). We further compared three fit indices (CFI, RMSEA, and SRMR) between the models (Bagheri, Jafari, Tashakor, Kouhpayeh, & Riazi, 2014) to determine whether the measurement invariance was supported: ΔCFI>-.01, ΔRMSEA<.015, and ΔSRMR<.01 (C. -Y. Lin, Ku, & Pakpour, 2017). However, if the fit indices were not fully satisfied, we apply partial invariance to relax the constraint in the loading or intercept invariance one at a time to assess partial invariance (Byrne, Shavelson, & Muthén, 1989).
The correlations between WSSQ, WBIS, PWD, and QoL instruments were computed using Pearson's correlations. Because WSSQ and WBIS share the same concept of self-stigma, we hypothesized that the correlation between WSSQ and WBIS was the strongest. As for other correlations, we hypothesized them in moderate correlations (r between .30 and .50). In addition, we tested the differences between the correlations (r of WSSQ and other instruments vs. WBIS and other instruments) using a test on two dependent correlations with one variable in common (I. A. Lee & Preacher, 2013). The descriptive statistics were done using SPSS 23.0 (IBM Corp., Chicago, IL), and the CFAs (including MGCFAs) were done using lavaan package in R software (lavaan.ugent.be).
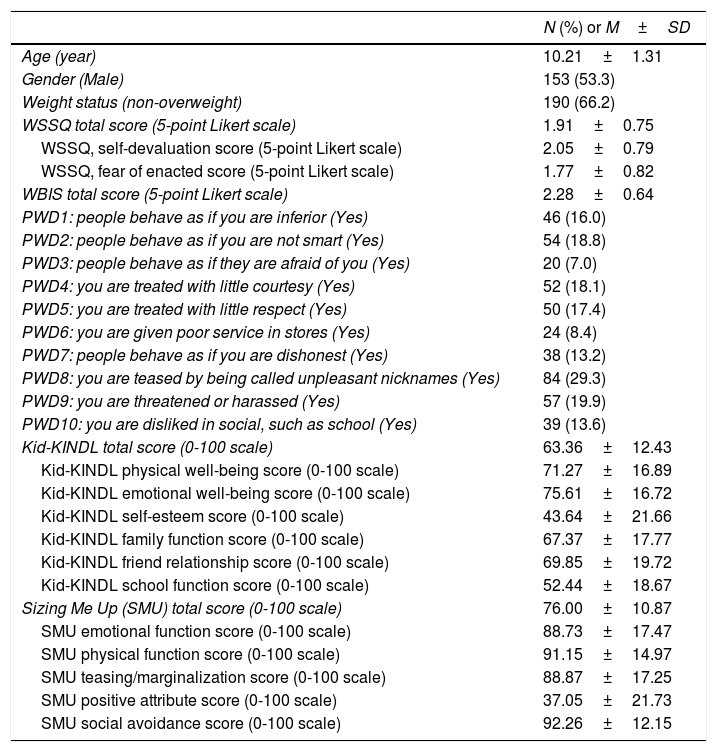
ResultsThe mean (SD) age of the children was 10.21 (1.31) years; slightly more than half of them were boys (n=153, 53.3%). Nearly two thirds of the participants were non-overweight (n=190, 66.2%); Table 1 shows their scores in self-stigma and QoL.
Participant characteristics.
| N (%) or M±SD | |
|---|---|
| Age (year) | 10.21±1.31 |
| Gender (Male) | 153 (53.3) |
| Weight status (non-overweight) | 190 (66.2) |
| WSSQ total score (5-point Likert scale) | 1.91±0.75 |
| WSSQ, self-devaluation score (5-point Likert scale) | 2.05±0.79 |
| WSSQ, fear of enacted score (5-point Likert scale) | 1.77±0.82 |
| WBIS total score (5-point Likert scale) | 2.28±0.64 |
| PWD1: people behave as if you are inferior (Yes) | 46 (16.0) |
| PWD2: people behave as if you are not smart (Yes) | 54 (18.8) |
| PWD3: people behave as if they are afraid of you (Yes) | 20 (7.0) |
| PWD4: you are treated with little courtesy (Yes) | 52 (18.1) |
| PWD5: you are treated with little respect (Yes) | 50 (17.4) |
| PWD6: you are given poor service in stores (Yes) | 24 (8.4) |
| PWD7: people behave as if you are dishonest (Yes) | 38 (13.2) |
| PWD8: you are teased by being called unpleasant nicknames (Yes) | 84 (29.3) |
| PWD9: you are threatened or harassed (Yes) | 57 (19.9) |
| PWD10: you are disliked in social, such as school (Yes) | 39 (13.6) |
| Kid-KINDL total score (0-100 scale) | 63.36±12.43 |
| Kid-KINDL physical well-being score (0-100 scale) | 71.27±16.89 |
| Kid-KINDL emotional well-being score (0-100 scale) | 75.61±16.72 |
| Kid-KINDL self-esteem score (0-100 scale) | 43.64±21.66 |
| Kid-KINDL family function score (0-100 scale) | 67.37±17.77 |
| Kid-KINDL friend relationship score (0-100 scale) | 69.85±19.72 |
| Kid-KINDL school function score (0-100 scale) | 52.44±18.67 |
| Sizing Me Up (SMU) total score (0-100 scale) | 76.00±10.87 |
| SMU emotional function score (0-100 scale) | 88.73±17.47 |
| SMU physical function score (0-100 scale) | 91.15±14.97 |
| SMU teasing/marginalization score (0-100 scale) | 88.87±17.25 |
| SMU positive attribute score (0-100 scale) | 37.05±21.73 |
| SMU social avoidance score (0-100 scale) | 92.26±12.15 |
Note. WSSQ=Weight Self-Stigma Questionnaire. WBIS=Weight Bias Internalization Scale. PWD=perceived weight discrimination; adapted from Schafer and Ferraro (2011).
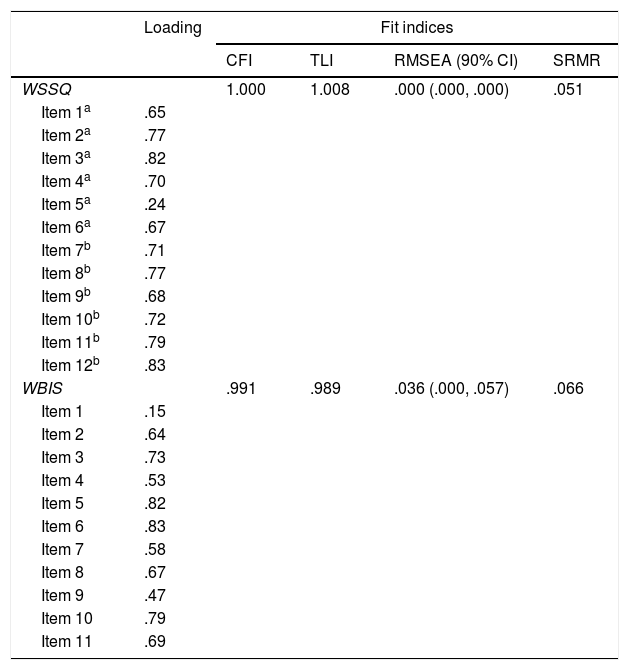
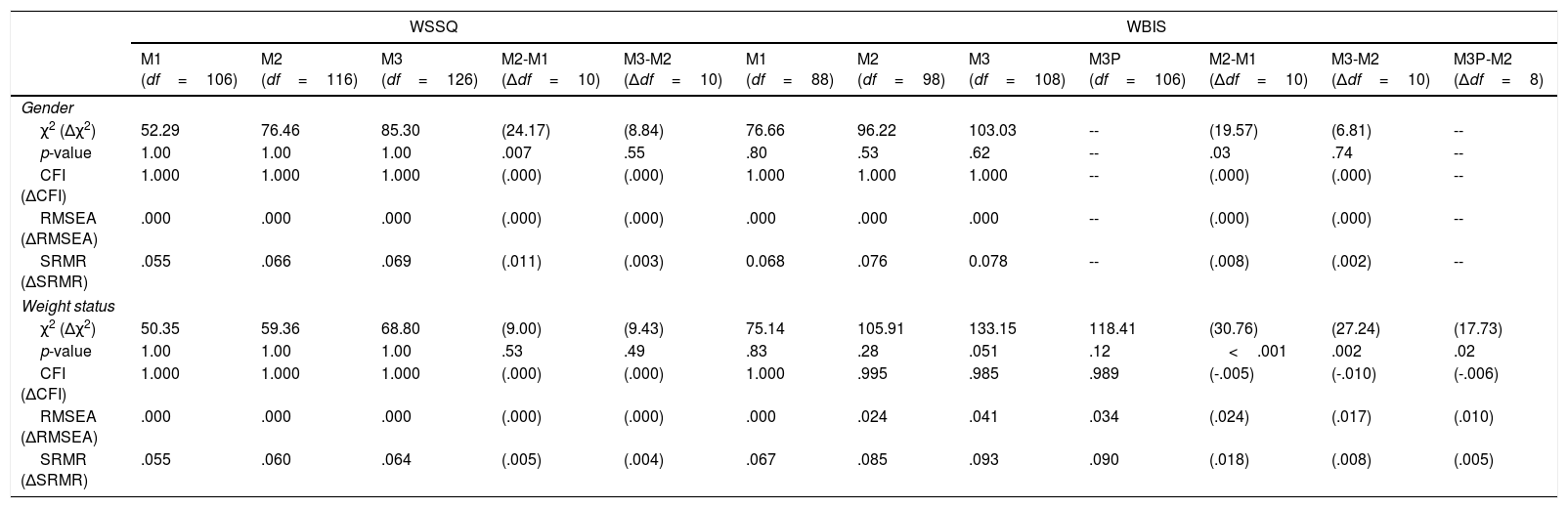
Table 2 illustrates the data-model fit for the two-correlated-factor model in WSSQ and the unidimensional model in WBIS; both questionnaires had satisfactory structures: (CFI=1.000, TLI=1.008, RMSEA=.000, and SRMR=.051 for WSSQ; CFI=.991, TLI=.989, RMSEA=.036, and SRMR=.066 for WBIS). All the factor loadings were strong—.65 to .83 in WSSQ; .47 to .83 in WBIS—except for item 5 in the WSSQ (.24) and item 1 in the WBIS (.15). Given the satisfactory fit in both questionnaires, we did not adjust their factor structures used for the process of assessing measurement invariance. The MGCFAs showed that the measurement invariance of WSSQ was supported across gender and weight status. The measurement invariance of WBIS was supported across gender but not across weight status. However, after relaxing the constraints for two item intercepts (i.e., items 1 and 9), the partial invariance was supported (Table 3). Additionally, the completely standardized latent mean differences between genders were -.144 for WSSQ self-devaluation domain; -.132 for WSSQ fear of enacted domain; and -.036 for WBIS. The completely standardized latent mean differences between weight statuses were -.467 for WSSQ self-devaluation domain; -.367 for WSSQ fear of enacted domain; -.103 for WBIS with all item intercepts constrained; and -.095 for WBIS with relaxed item intercepts.
Confirmatory factor analysis for Weight Self-Stigma Questionnaire (WSSQ) and Weight Bias Internalization Scale (WBIS).
| Loading | Fit indices | ||||
|---|---|---|---|---|---|
| CFI | TLI | RMSEA (90% CI) | SRMR | ||
| WSSQ | 1.000 | 1.008 | .000 (.000, .000) | .051 | |
| Item 1a | .65 | ||||
| Item 2a | .77 | ||||
| Item 3a | .82 | ||||
| Item 4a | .70 | ||||
| Item 5a | .24 | ||||
| Item 6a | .67 | ||||
| Item 7b | .71 | ||||
| Item 8b | .77 | ||||
| Item 9b | .68 | ||||
| Item 10b | .72 | ||||
| Item 11b | .79 | ||||
| Item 12b | .83 | ||||
| WBIS | .991 | .989 | .036 (.000, .057) | .066 | |
| Item 1 | .15 | ||||
| Item 2 | .64 | ||||
| Item 3 | .73 | ||||
| Item 4 | .53 | ||||
| Item 5 | .82 | ||||
| Item 6 | .83 | ||||
| Item 7 | .58 | ||||
| Item 8 | .67 | ||||
| Item 9 | .47 | ||||
| Item 10 | .79 | ||||
| Item 11 | .69 | ||||
Note. aEmbedded in self-devaluation domain. bEmbedded in fear of enacted domain. CFI=comparative fit index; TLI=Tucker-Lewis index; RMSEA=root mean square error of approximation; SRMR=standardized root mean square residual.
Measurement invariance of Weight Self-Stigma Questionnaire (WSSQ) and Weight Bias Internalization Scale (WBIS) across gender (boy vs. girl) and across weight status (overweight vs. non-overweight).
| WSSQ | WBIS | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 (df=106) | M2 (df=116) | M3 (df=126) | M2-M1 (Δdf=10) | M3-M2 (Δdf=10) | M1 (df=88) | M2 (df=98) | M3 (df=108) | M3P (df=106) | M2-M1 (Δdf=10) | M3-M2 (Δdf=10) | M3P-M2 (Δdf=8) | |
| Gender | ||||||||||||
| χ2 (Δχ2) | 52.29 | 76.46 | 85.30 | (24.17) | (8.84) | 76.66 | 96.22 | 103.03 | -- | (19.57) | (6.81) | -- |
| p-value | 1.00 | 1.00 | 1.00 | .007 | .55 | .80 | .53 | .62 | -- | .03 | .74 | -- |
| CFI (ΔCFI) | 1.000 | 1.000 | 1.000 | (.000) | (.000) | 1.000 | 1.000 | 1.000 | -- | (.000) | (.000) | -- |
| RMSEA (ΔRMSEA) | .000 | .000 | .000 | (.000) | (.000) | .000 | .000 | .000 | -- | (.000) | (.000) | -- |
| SRMR (ΔSRMR) | .055 | .066 | .069 | (.011) | (.003) | 0.068 | .076 | 0.078 | -- | (.008) | (.002) | -- |
| Weight status | ||||||||||||
| χ2 (Δχ2) | 50.35 | 59.36 | 68.80 | (9.00) | (9.43) | 75.14 | 105.91 | 133.15 | 118.41 | (30.76) | (27.24) | (17.73) |
| p-value | 1.00 | 1.00 | 1.00 | .53 | .49 | .83 | .28 | .051 | .12 | <.001 | .002 | .02 |
| CFI (ΔCFI) | 1.000 | 1.000 | 1.000 | (.000) | (.000) | 1.000 | .995 | .985 | .989 | (-.005) | (-.010) | (-.006) |
| RMSEA (ΔRMSEA) | .000 | .000 | .000 | (.000) | (.000) | .000 | .024 | .041 | .034 | (.024) | (.017) | (.010) |
| SRMR (ΔSRMR) | .055 | .060 | .064 | (.005) | (.004) | .067 | .085 | .093 | .090 | (.018) | (.008) | (.005) |
Note. M1=configural model. M2=model that constraints all factor loadings being equal across group (either in gender or weight status). M3=model that constraints all factor loadings and all item intercepts being equal across group (either in gender or weight status). CFI=comparative fit index; RMSEA=root mean square error of approximation; SRMR=standardized root mean square residual.
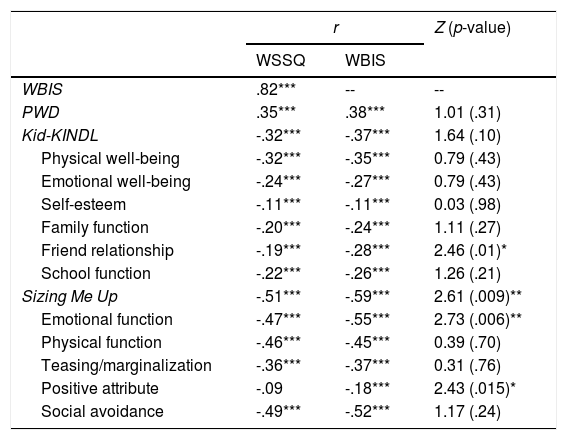
The correlation between WSSQ and WBIS was quite strong (r=.82). In addition, WSSQ was moderately correlated to PWD (r=.35), Kid-KINDL (r=-.32), and Sizing Me Up (r=-.51). WBIS showed a similar pattern to WSSQ (r=.38 with PWD; -.37 with Kid-KINDL; -.59 with Sizing Me Up). Moreover, as compared with WSSQ, WBIS had stronger correlations to the Friend relationship domain in Kid-KINDL, Sizing Me Up total score, emotional function, and positive attribute domains in Sizing Me Up (Table 4). However, if we take the multiple comparisons of the correlation coefficients into consideration and apply corrections for the multiple comparisons, the stronger coefficients in the WBIS were not significantly different from the slightly weaker coefficients in the WSSQ.
Correlation comparisons between the Weight Self-Stigma Questionnaire (WSSQ) and Weight Bias Internalization Scale (WBIS).
| r | Z (p-value) | ||
|---|---|---|---|
| WSSQ | WBIS | ||
| WBIS | .82*** | -- | -- |
| PWD | .35*** | .38*** | 1.01 (.31) |
| Kid-KINDL | -.32*** | -.37*** | 1.64 (.10) |
| Physical well-being | -.32*** | -.35*** | 0.79 (.43) |
| Emotional well-being | -.24*** | -.27*** | 0.79 (.43) |
| Self-esteem | -.11*** | -.11*** | 0.03 (.98) |
| Family function | -.20*** | -.24*** | 1.11 (.27) |
| Friend relationship | -.19*** | -.28*** | 2.46 (.01)* |
| School function | -.22*** | -.26*** | 1.26 (.21) |
| Sizing Me Up | -.51*** | -.59*** | 2.61 (.009)** |
| Emotional function | -.47*** | -.55*** | 2.73 (.006)** |
| Physical function | -.46*** | -.45*** | 0.39 (.70) |
| Teasing/marginalization | -.36*** | -.37*** | 0.31 (.76) |
| Positive attribute | -.09 | -.18*** | 2.43 (.015)* |
| Social avoidance | -.49*** | -.52*** | 1.17 (.24) |
Note. *p<.05; **p<.01; ***p<.001. PWD=perceived weight discrimination; Kid-KINDL is a generic quality of life measure; Sizing Me Up is a weight-related quality of life measure.
To our knowledge, this is the first study that has compared psychometric characteristics of the WSSQ and WBIS among children with overweight and obesity as well as their counterparts with normal weight. Our study showed that both self-reported measures on internalized weight stigma (i.e., WSSQ and WBIS) had an acceptable factor structure. Furthermore, our results were unique in providing evidence of factorial invariance across gender and weight status groups among children. In addition, both WSSQ and WBIS measures were mutually correlated and associated with other measures, including PWD, Kid-KINDL and Sizing Me Up.
The original two-factor structure of the WSSQ fit well with the data and suggested that children perceive weight self-stigma in a multidimensional perspectives (i.e., domains of self-devaluation and fear of enacted stigma), which was consistent with the study of French adolescents (Maïano et al., 2017). All the item loadings in our results, except for item 5, were in anticipation and were comparable to those obtained from Maïano et al.’s study (2017). Given that item 5 (“I would never have any problems with weight if I were stronger”) had a relatively low factor loading in our results, which indicated that item 5 had a low level of contribution to the self-devaluation subscale in our sample. A potential reason is that most of the children had normal weight (∼ two thirds) and the content of the item was not fully connected with children without overweight. Nevertheless, other studies on adults have also demonstrated that weight self-stigma could be measured using the aforementioned two latent variables (Hain et al., 2015; Lillis et al., 2010; K. P. Lin & Lee, 2017). Hence, we are confident that the WSSQ has satisfactory factorial validity.
The unidimensional structure of the WBIS was supported in this study and this finding is in accordance with other studies on adolescents (Roberto et al., 2012) and adults (Durso & Latner, 2008; Hilbert et al., 2014). Similar to previous studies on both children and adult populations (Durso & Latner, 2008; Hilbert et al., 2014; M. S. Lee & Dedrick, 2016; Roberto et al., 2012) item 1 (“No matter how much I weigh, I can do just as much as everyone else”) was found to have poor factor loading. Moreover, Zuba and Warschburger (2018) showed that removing item 1 can increase all psychometric statistics including model fit among primary school children. A possible reason for this may lie in the fact that children or even their parents underestimate the child's body weight (Pakpour, Yekaninejad, & Chen 2011). Therefore, they cannot identify themselves as having a weight problem (Yao & Hillemeier, 2012), and cannot link up the association between their weight and their capabilities.
Regarding measurement invariance, our findings demonstrated that boys and girls who completed the WSSQ and WBIS had a similar model structure. To the best of our knowledge, the factorial invariance on gender had only been conducted in one study on WBIS among primary school children (Zuba & Warschburger, 2018), and our factorial invariance findings agreed with that study's results. The invariance findings had an important implication on future studies that measure gender differences in self-reported weight-related stigma when using WSSQ and WBIS. For example, girls were reported to score higher weight-related stigma than boys because of the girls experiencing more weight-based stigmatization (Zuba & Warschburger, 2018). Therefore, girls felt more social pressure to lose weight and diet than boys, and girls would report more scores on both WSSQ and WBIS measures. In other words, the invariance evidence across gender in Zuba and Warschburger's (2018) study and our findings helped in detecting real differences on weight-related stigma across gender rather than observing differences in interpretations for WSSQ and WBIS item contents between genders.
Regarding factorial invariance across weight status, our results showed that both group with overweight and group without overweight had similar interpretations of the WSSQ items, regardless of weight status. However, some WBIS items were not invariant across the weight status groups. Therefore, caution should be noted when using WBIS to assess weight status differences on weight-related self-stigma, especially because there is growing interest in comparing weight-related self-stigma between samples with and without overweight (Zuba & Warschburger, 2018). Future research should further examine which items in the WBIS should be revised for reaching measurement invariance for children across weight status.
Finally, our results indicated that both WSSQ and WBIS correlated significantly with perceived weight discrimination and with generic and weight-related QoL measures. Our results were in line with previous reports suggesting that internalized weight stigma was associated with poor mental health and deteriorated QoL (Durso & Latner, 2008; Hilbert et al., 2014; Zuba & Warschburger, 2018). Specifically, when we compared both measures (WSSQ and WBIS), WBIS had slightly stronger correlations with the Friend relationship domain in the Kid-KINDL, Sizing Me Up total score, emotional function, and positive attribute domains in Sizing Me Up. Therefore, our results suggested that the WBIS was slightly more sensitive to the levels of weigh-related QoL than the WSSQ. Based on the psychometric findings from the WSSQ and WBIS, we would recommend that healthcare providers and researchers consider the following: (1) If a person is interested in comparing weight-related self-stigma between weight status groups, using WSSQ may be a better choice than using WBIS; (2) if a person is interested in understanding the relationship between weight-related self-stigma and QoL for children, using WBIS may have slightly more benefits than using WSSQ. For example, WBIS can be used to understand the effectiveness of stigma reduction programs on QoL for children with overweight.
There are some limitations in this study. First, because of the convenience sampling method, our sample was not representative of the entire population of Hong Kong children. Second, we did not obtain the weight and height using objective measure; such information could be biased in our self-reported measure because of the social desirability and recall bias. Third, although having neurological diseases was one of our exclusion criteria, we were unable to fully identify whether a participant had such disease because it was self-reported.
In conclusion, both WSSQ and WBIS measures were valid scales to assess the internalization of weight bias. Despite considerable correlation between WSSQ and WBIS, our results suggest that these measures have specific psychometric properties and are not recommended to be used interchangeably.
FundingThis research was supported in part by (received funding from) the startup fund in the Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong.
This research was supported in part by (received funding from) the startup fund in the Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong. We thank the assistance from the following organizations: HKTA Wun Tsuen Ng Lai Wo Memorial School, Buddhist Wong Cheuk Um Primary School, Hong Kong Playground Association, Hin Keng Children & Youth Centre of Hong Kong Playground Association.
