




Depressive symptoms are prevalent in adolescence, but not all adolescents experience the same level or evolution of symptoms, suggesting the need to identify differences in trajectories of symptoms. We used Growth Mixture Modeling to analyze different trajectories of depressive symptoms in a sample of 1,072 Chilean adolescents (12-15 years old, 54% female). First, a baseline model was selected and then adolescent irritability, maternal warmth, demandingness and disrespect were introduced to the model as predictors of class membership. Four latent class trajectories of depressive symptoms were identified: high persistent (12%), low stable (56%), high decreasing (15%) and low increasing (17%). Low stable was the most prevalent class, and was characterized by higher maternal warmth and lower maternal disrespect and adolescent irritability while high persistent was characterized by the opposite maternal characteristics. Significant gender differences in class membership were observed. The results highlight the importance of identifying different trajectories of depressive symptoms and specific predictors of each trajectory. The association of parenting dimensions with trajectories of persistent depressive symptoms provides evidence that parenting can serve as both a protective and risk factor for adolescent adjustment.
La sintomatología depresiva es prevalente durante la adolescencia, pero no todos los adolescentes experimentan el mismo nivel y evolución de esta sintomatología, lo que sugiere la necesidad de identificar diferencias en las trayectorias de los síntomas. Usando Growth Mixture Modeling analizamos diferentes trayectorias de síntomas depresivos en 1.072 adolescentes chilenos (12-15 años, 54% mujeres). Primero, se seleccionó un modelo basal y luego se utilizó la irritabilidad del adolescente, la calidez, demanda y falta de respeto de la madre como predictores de la pertenencia a las clases. Se seleccionó un modelo con 4 clases latentes de síntomas depresivos: alta persistente (12%), baja estable (56%), alta decreciente (15%) y baja creciente (17%). La clase baja estable fue la más prevalente y se caracterizó por alto nivel de calidez maternal y bajo nivel de falta de respeto materna e irritabilidad del adolescente, en tanto que la clase alta persistente presentó características opuestas (baja calidez y alta demanda materna e irritabilidad del adolescente). Se observaron diferencias en la prevalencia de clases por sexo. Estos resultados resaltan la importancia de identificar diferentes trayectorias de síntomas depresivos y sus predictores. La asociación entre las dimensiones parentales y las trayectorias de síntomas depresivos persistentes provee evidencia de que los comportamientos parentales pueden servir, tanto como factores protectores como de riesgo.
Depressive symptoms in adolescence are of concern because of its association with long-term health outcomes (Costello, Swendsen, Rose, & Dierker, 2008; Keenan-Miller, Hammen, & Brennan, 2007; Ramiro, Teva, Bermúdez, & Buela-Casal, 2013), the emergence of major depressive disorders (Georgiades, Lewinsohn, Monroe, & Seeley, 2006), and their overall developmental significance. Poor mental health in adolescence impedes the development of social, cognitive, and psychological competencies that predict adaptation in young adulthood (Diamantopoulou, Verhulst, & Van der Ende, 2011; Zappitelli et al., 2013). Findings from studies in diverse samples (i.e., North American, European and South American) consistently reveal a high prevalence of depressive symptoms in adolescents (Abela & Hankin, 2011; Cumsille & Martínez, 1997; De la Barra, Vicente, Saldivia, & Melipillán, 2012; Roberts, Lewinsohn, & Seeley, 1995). In Chile, depression is a highly prevalent and disabling condition, ranked the second most common cause of disease burden (Vicente, Saldivia, de la Barra et al., 2012). Comparison of prevalence rates in adulthood suggested that depression is more common in Chile than in European or other South American countries, a finding usually attributed to rapid changes in socio-political context and lifestyles in Chile (Stapinski et al., 2013). However, it is not the presence of depressive symptoms at a single moment of time that is of concern but the persistence of symptoms over time. Cross-sectional analyses of depressive symptoms may capitalize on measurement error (lead to misinterpretations) as adolescent mood is both more volatile and shows more extreme high and lows than that of adults (Larson & Csikszentmihalyi, 1980). Because depressed mood may be transient in adolescence, it is important to distinguish between temporary highs and lows in mood from depressive symptoms that persist over time.
Early studies in adolescents examined subtypes of depression as states rather than as processes that unfold over time (Stoolmiller, Kim, & Capaldi, 2005). Timing of pubertal events (Angold & Costello, 2006; Hamilton, Hamlet, Stange, Abramson, & Alloy, 2014), changes in the brain system that regulates affect and behavior around puberty (Paus, 2005; Steinberg, 2005), and contextual factors associated to depressive mood in adolescence (Balluerka, Aritzeta, Gorostiaga, Gartzia, & Soroa, 2013) call for a dynamic analysis of variation of depressed mood symptoms over time. Findings based on cross-sectional analyses implicitly assume stability of symptoms. In contrast, designs with repeated assessments of the same adolescents are keen to model changes in patterns of depressive symptoms (Brendgen, Wanner, Morin, & Vitaro, 2005; Costello et al., 2008; Diamantopoulou et al., 2011; Wickrama, Wickrama, & Lott, 2009) and to examine how individual and contextual factors predict trajectories.
Preliminary evidence of heterogeneity in the course of depressive symptoms during adolescence comes from studies with U.S. adolescents. In a sample of 206 males ages 15-24 years, Stoolmiller et al. (2005) identified four classes of depressive symptoms (i.e., very low, moderate decreasing, high decreasing and high persistent). Membership in the high persistent class was predicted by low family income, low childhood academic achievement, high childhood depressive symptoms, high negative life events, and high number of changes in parental figures during childhood. Members of the high decreasing and high persistent classes displayed elevated rates of lifetime major depressive disorders in emerging adulthood when compared to members of the moderate and low classes.
Based on a sample of 11,500 youth (ages 12-19) from the National Longitudinal Study of American Adolescent Health, two separate studies examined trajectories of depression. Costello et al. (2008) modeled four distinct classes of depressed mood trajectories from 12 to 25 years, namely no depressed mood, stable low, early declining, and late escalating. Predictors of membership in any of the three trajectories of depressed mood included gender (female), ethnic minority status, delinquent behavior, and adolescent substance use. Higher socioeconomic status, residing in a two-parent household, higher perceived social connection (to parents, peers and school), and higher self-esteem were associated with a greater likelihood of belonging to the no depressed mood trajectory compared to the depressed mood trajectories (Costello et al., 2008). Similarly, Wickrama et al. (2009) modeled four depressive symptoms trajectories in adolescents from 13 to 23 years that they labeled chronically high, consistently low, increasing, and decreasing. Controlling for demographic characteristics, adolescents following different depressive mood trajectories differed in a number of risky behaviors such as multiple sex partner, drinking, and smoking.
Finally, in a sample of 719 adolescents, Yaroslavsky, Pettit, Lewinsohn, Seeley and Roberts (2013) examined latent trajectories of depressive symptoms from mid-adolescence through age 30. Their resulting three-class model included a high stable, a moderate decreasing and a low decreasing trajectory of depressive symptoms. Gender (female) and poor interpersonal functioning distinguished those adolescents who displayed a persistently elevated course of symptoms from those who displayed moderate symptoms in adolescence followed by a reduction in symptoms during early adulthood (Yaroslavsky et al., 2013).
Though differences in analytical methods (e.g., GMM vs. ProcTraj) and sample characteristics (e.g., age span) preclude direct comparisons across these studies, their findings consistently point to the role of demographic factors such as gender, socioeconomic and minority status, and family structure as predictors of the course of symptoms. Because studies are not comparable, the association of particular trajectories with adolescent characteristics such as history of problem behavior, substance use and self-esteem are not conclusive.
Parenting dimensions and the course of depressive symptoms?Little is known about how family processes and parenting specifically relates to the patterning of depressive symptoms over time. Though two studies have examined how indicators of family relationships relate to different trajectories of depressive symptoms (Wickrama et al., 2009; Yaroslavsky et al., 2013), their measures of family relationships have been combined with either peer and school (Wickrama et al., 2009) or relationship with siblings (Yaroslavsky et al., 2013) indicators. Given the composite nature of the measures, their findings regarding effects of family variables are uncertain.
Early to middle adolescence appears to be a sensitive period in the emergence and evolution of depressive symptoms. During early adolescence parents and adolescents negotiate autonomy related changes that realign parent-child relationships. Reorganization of regulatory systems of affect and behavior (Steinberg, 2005) as well as frequency or intensity of parent-adolescent conflict are two factors that may account for the frequency of depressive symptoms.
Findings from studies on parental socialization indicated that adolescents raised by authoritative parents (i.e., warm and reasonably demanding) showed advantages in psychosocial development and mental health over peers raised in non-authoritative homes (Steinberg, 2001). In several studies conducted among European American families, findings suggest that the way parents interact with their children is related to adolescent depressive symptoms. For example, Ge, Conger, Lorenz and Simons (1994) found that warm and involved parenting was negatively related to depressive symptoms and that parenting characterized by harshness and inconsistent discipline was positively related to adolescent depressive symptoms. In a subsequent study of 388 adolescents Ge, Best, Conger and Simons (1996) found that, after controlling for demographics and symptoms at the first time of measurement, parental warmth and skillful discipline decreased whereas hostility increased depressive symptoms. Conversely, studies have shown that adolescents whose parents treated them with disrespect were more likely to report depressive symptoms (Barber, Stolz, Olsen, & Collins, 2005; Barber, Xia, Olsen, McNeely, & Bose, 2012). Overall, these findings confirm that parental warmth protects children and adolescents from depression and other forms of internalized distress (Ge et al., 1996; Kim & Ge, 2000; Soenens, Park, Vansteenkiste, & Mouratidis, 2012).
These studies did not examine changes in the course of depressive symptoms, thus their findings do not inform about the association of parental dimensions with trajectories of depressive symptoms. Longitudinal evidence that negative relationships with parents increases the odds of an elevated trajectory of depressed mood is provided by Brendgen et al. (2005) findings. In a predominantly Caucasian sample of 550 Canadian adolescents, they found that the quality of adolescents’ relationship with parents (i.e., attachment, disclosure, communication) predicted trajectories of depressive symptoms.
Though parental characteristics create an emotional climate for behavioral exchanges between parents and adolescents (Darling & Steinberg, 1993), the contribution of adolescent characteristics to developmental outcomes should not be overlooked (Kerr, Stattin, & Burk, 2010). For example, temperamental dimensions may interact (Pérez & Cumsille, 2012) with parental characteristics or show independent effects on adolescent behavior. Relatedly, Brengden et al. (2005) found that negative emotionality during childhood increased the risk of a high depression trajectory in early adolescence.
One particular temperamental dimension that has been linked to depressive symptoms is irritability. Adolescent irritability has been associated with a wide range of youth psychiatric disorders in cross-sectional studies, and specifically with depressive and generalized anxiety disorders in longitudinal analysis (Stringaris, Cohen, Pine, & Leibenluft, 2009; Stringaris, Maughan, Copeland, & Costello, 2013; Stringaris, Zavos, Leibenluft, Maughan, & Eley, 2012). Stringaris et al. (2009) conducted a longitudinal community-based study of 631 US participants, whose parents were interviewed when participants were in early adolescence and participants were interviewed 20 years later. Findings indicated that adolescent irritability (i.e., the propensity to react with anger or grouchiness disproportionate to the situation reported by parent) increased the risk for developing depressive disorders and generalized anxiety disorder over a 20-year follow-up period. In a subsequent longitudinal study of 2,651 U.K. twin/sibling adolescents, Stringaris et al. (2012) estimated the genetic overlaps between the two components of oppositional behavior (i.e., irritability and headstrong/hurtful behaviors) and depression and delinquency. Using multivariate genetic analyses the authors found that irritability was more related with depression than with delinquency (Stringaris et al., 2012). Findings of these studies suggest that irritability is linked to depressive symptoms during adolescence and early adulthood.
Based on the previous antecedents, the main aims of this study were to:
- 1.
Identify different classes of trajectories of depressive symptoms in adolescents.
- 2.
Estimate the role of three parenting dimensions in predicting membership in different trajectories, particularly those of persistent depressive symptoms.
- 3.
Estimate the role of adolescent irritability in predicting membership in different trajectories, particularly those of persistent depressive symptoms.
The study used data from 1,072 adolescents who were between 12 and 15 years of age (M=14.1 years, SD=0.98, 54% female) at the time of first measurement. Students were in 7th to 10th grade, and most of them lived with both parents in the house (67%), only with the mother (21%) or the mother and a stepfather (7.5%). Forty-five percent of the fathers and thirty-eight percent of the mothers had university education, and 28% of the mothers and 24% of the fathers have not completed high school. Most of the participants (91%) had at least one sibling, and 30% percent of the participants were first born and 31% were second born. Adolescents were part of a prospective longitudinal study of parent adolescent-communication and were followed annually for 4 years. Participants were drawn from schools selected to represent the socioeconomic diversity of the Chilean educational system and included private (45%), private subsidized (20%), and municipal (35%) schools from the metropolitan area of Santiago. These schools broadly represent upper, middle and lower SES youth in the region. Self-report questionnaires were administered in schools each year from 2007 to 2010. Data were available for 1072, 788, 700 and 523 adolescents for the four waves of measurement. Because missing data was due to attrition, mostly because adolescents graduated from school, it was considered Missing at Random (Graham, Cumsille, & Shevock, 2013) and were handled in MPlus using Full Information Maximum Likelihood (FIML).
ProcedureSchool authorities were informed of the study goals and permission was requested to group-administer the questionnaires during classes. In accordance with Chilean ethical regulations at the time of the study, parental passive consent and adolescent active assent was requested. Fewer than 1% of the parents and/or adolescents refused to participate. Trained undergraduate psychology students administered questionnaires during homeroom classes and participating students received a snack and were entered into a raffle for movie tickets. The study protocol was approved by the ethics committee of Pontificia Universidad Católica de Chile and the funding agency, Fondo Nacional de Desarrollo Científico y Tecnológico (FONDECYT).
InstrumentsThe scale of depressive symptoms included 5 questions similar to the subscale of negative affect of the Center for Epidemiological Studies Depression Scale (Phillips et al., 2006). Adolescents were asked how often in the last 30 days they have felt down, tense, depressed, lonely and misunderstood. Response options included never (1), once (2), twice (3), three times (4), once a week (5) and almost daily (6). Confirmatory factor analysis (not reported) supported the longitudinal invariance of the measure. Internal consistency for this scale was estimated with Cronbach's alpha over .85 for each of the 4 measurement times.
Three measures of parenting behavior and one measure of temperamental disposition were computed at the time of the first and second measurement. Parental measures included parental disrespect (8 items, Cronbach's alpha=.84; sample item “[parents] try to make me feel guilty”) (Barber et al., 2012), parental warmth/responsiveness (4 items, Cronbach's alpha=.88, sample item “I can count on my mother's help if I need it”) and maternal expectations/demandingness (4 items, Cronbach's alpha=.83, sample item “My mother expects me to behave responsibly”). Confirmatory factor analysis supported the longitudinal invariance of the parental measures (Cumsille, Martínez, Rodríguez, & Darling, 2014). A measure of adolescent irritability (frustration tolerance) was computed using 5 items (Cronbach's alpha=.63, sample item “It really annoys me to have to wait in line”) (Pérez & Cumsille, 2012).
Analytic strategyWe modeled trajectories of depressive symptoms using Growth Mixture Modeling (GMM) in Mplus 7.1 (Modecki, Barber, & Eccles, 2014; Muthén & Muthén, 1998-2012). Unlike traditional Latent Growth Models where a single trajectory is estimated, through GMM it is possible to identify different classes of trajectories; that is, trajectories that may vary in the form of the growth or change over time (see Grimm & Ram, 2009, for an accessible review of the technique). First, a baseline model was selected with a specific number and shape of classes. Classes were selected according to criteria suggested in the literature (Grimm & Ram, 2009), including BIC (model with lowest BIC value), Vuong-Lo-Mendell-Rubin (VLMR) likelihood ratio test (select model with k-1 classes when p-value for model with k classes is >= .05), Lo-Mendell-Rubin (LMR) likelihood ratio test (same selection criteria as VLMR), Bootstrapping likelihood ratio test (BLRT, same selection criteria as VLMR), differentiation of the classes (entropy, models with values higher than .7) and classes sizes (no class should have fewer than 5% of the sample). Once classes were identified, we introduced the predictors of class membership and predictors of the level of depression within classes. Finally, using the output of the most likely class membership, we conducted an ANOVA with planned contrasts to identify differences between classes. As findings from several studies suggest gender differences in the prevalence of (i.e., higher for girls) (Dekker et al., 2007; Rawana & Morgan, 2014; Sallinen, Rönkä, Kinnun, & Kokko, 2007), level (Fernández & Kroner-Herwig, 2013), shape and timing (Dekker et al., 2007) of depressive symptoms, we examined the role of gender as a predictor of trajectory membership.
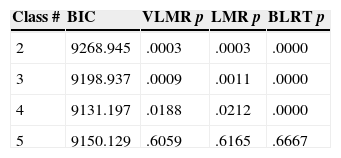
ResultsTable 1 presents the summary statistics for models with 2 to 5 classes. Given that BIC, VLMR, LMR and BLRT indices all favored the 4-class solution, and that none of the classes has fewer than 5% of the cases, this model was selected as the baseline. For model identification purposes, variances for the slope and the quadratic parameters were set to 0 for all the classes. The intercept was estimated as a random parameter.
Model Fit Comparisons for Models with 2 to 5 Classes N=1,072.
| Class # | BIC | VLMR p | LMR p | BLRT p |
|---|---|---|---|---|
| 2 | 9268.945 | .0003 | .0003 | .0000 |
| 3 | 9198.937 | .0009 | .0011 | .0000 |
| 4 | 9131.197 | .0188 | .0212 | .0000 |
| 5 | 9150.129 | .6059 | .6165 | .6667 |
BIC= Bayes Information Criteria; VLMR= Vuong-Lo-Mendell-Rubin likelihood ratio test;
LMR= Lo-Mendell-Rubin likelihood ratio test; BLTR= Bootstrapping likelihood ratio test.
The four-class solution included two flat and two curvilinear trajectories. As we can see in Figure 1, the two flat trajectories correspond to a low stable (56%) and a persistent high (12%) trajectory. The other two trajectories were named low increasing (17%) and high decreasing (15%) symptoms over time.

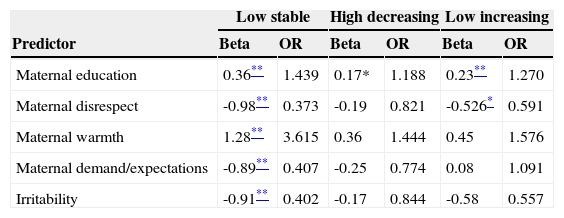
Predictors of class membership were introduced to the model. Table 2 presents the regression coefficients and Odd ratios comparing all the models to the high persistent class (reference group).
Regression coefficients and OR comparing each class to the High persistent class.
| Low stable | High decreasing | Low increasing | ||||
|---|---|---|---|---|---|---|
| Predictor | Beta | OR | Beta | OR | Beta | OR |
| Maternal education | 0.36** | 1.439 | 0.17* | 1.188 | 0.23** | 1.270 |
| Maternal disrespect | -0.98** | 0.373 | -0.19 | 0.821 | -0.526* | 0.591 |
| Maternal warmth | 1.28** | 3.615 | 0.36 | 1.444 | 0.45 | 1.576 |
| Maternal demand/expectations | -0.89** | 0.407 | -0.25 | 0.774 | 0.08 | 1.091 |
| Irritability | -0.91** | 0.402 | -0.17 | 0.844 | -0.58 | 0.557 |
Note. Reference class is High persistent.
Results from the multinomial regression suggest a clear pattern for the comparison of the low stable and the high persistent classes. Using the high persistent as the reference class, maternal warmth increased the odds of belonging to the low stable class. In contrast, maternal disrespect, maternal demand, and adolescent irritability decreased the odds of belonging to the low stable class. Maternal warmth was a particularly strong predictor of membership in the low stable class increasing the odds more than 3.5 times. Using the low stable as a reference class showed that it was clearly differentiated from the high decreasing class.
Sex was also a very powerful predictor of class membership. Being a girl increased the odds of belonging to the high persistent, compared to the low stable class, more than 29 times (p<.001).
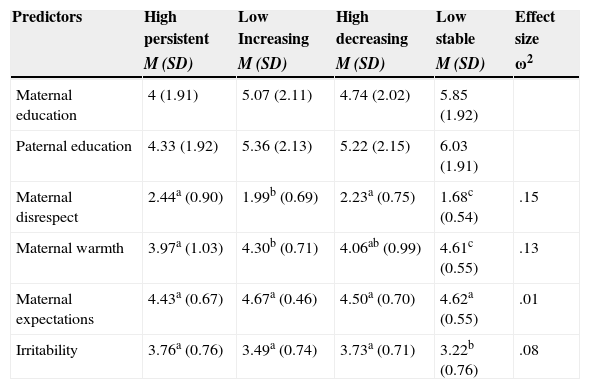
Using the posterior probabilities to classify adolescents in their most likely class, we conducted one way ANOVA's for the selected predictors. The means for each predictor by class are presented in Table 3. As expected, we found significant class differences for maternal disrespect (F[3,703]=41.75, p<.0001), maternal warmth (F[3,703]=37.41, p<.0001), maternal expectations (F[3,703]=4.32, p=.005), and adolescent irritability (F[3,703]=20.66, p<.0001). The low stable class is clearly distinguished from all other classes in terms of higher maternal warmth and lower maternal disrespect and adolescent irritability.
Means by class (n=707).
| Predictors | High persistent | Low Increasing | High decreasing | Low stable | Effect size |
|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | ω2 | |
| Maternal education | 4 (1.91) | 5.07 (2.11) | 4.74 (2.02) | 5.85 (1.92) | |
| Paternal education | 4.33 (1.92) | 5.36 (2.13) | 5.22 (2.15) | 6.03 (1.91) | |
| Maternal disrespect | 2.44a (0.90) | 1.99b (0.69) | 2.23a (0.75) | 1.68c (0.54) | .15 |
| Maternal warmth | 3.97a (1.03) | 4.30b (0.71) | 4.06ab (0.99) | 4.61c (0.55) | .13 |
| Maternal expectations | 4.43a (0.67) | 4.67a (0.46) | 4.50a (0.70) | 4.62a (0.55) | .01 |
| Irritability | 3.76a (0.76) | 3.49a (0.74) | 3.73a (0.71) | 3.22b (0.76) | .08 |
Note. Because of missing data in some of the predictor variables, data for this analysis was based on fewer cases. Means in rows with different letter are significantly different p<.01
Frequency analysis of class membership by gender showed that while 20% of the girls were classified in the high persistent class, only 3% of the boys were classified in the same class. Conversely, 69% of the boys, but only 39% of the girls, were classified in the low stable class.
Finally, introducing predictors of the level of the intercept within classes showed that for the low stable class, maternal warmth decreased the level of depressive symptoms, and maternal disrespect and adolescent irritability increased it. Maternal disrespect also increased the level of depressive symptoms in the high decreasing class. Interestingly, the predictors did not make a difference in the level of depression within the high persistent class.
DiscussionThe aim of this study was to identify different classes of trajectories of self-reported depressive symptoms during adolescence and to estimate whether parenting dimensions and adolescent temperament were related to class membership and to level of depressive symptoms. Four different trajectories–low stable, persistent high, high decreasing and low increasing–best captured the heterogeneity in the unfolding of symptoms during the four-year measurement period.
These findings are fairly consistent with those of previous longitudinal studies in both the number and shape of the trajectories identified (Brendgen et al., 2005; Costello et al., 2008; Fernández & Kroner-Herwig, 2013; Wickrama et al., 2009). Specifically, identified trajectories are similar in number and shape to those reported by Costello el al. (2008) and Wickrama and Wickrama (2010) using the Add Health data in the US. Though Costello et al's late escalating and early high declining depressed mood trajectories would suggest a different shape of trajectories compared to our findings, it is important to consider the different time frames of each study. Examination of Costello et al's trajectories within the age range of the current study (i.e., 12-18 years) reveals comparatively similar trajectories of symptoms within this age range. Thus, current findings add evidence to the patterning of depressive symptoms during adolescence in a different and understudied population. Considering the robustness of the trajectories identified it is possible to conclude that the majority of adolescents navigate adolescence with no or very low depressive symptoms (Brendgen et al., 2005; Costello et al., 2008; Wickrama & Wickrama, 2010), and those adolescents who do present depressive symptoms vary both in the level and course of their symptoms.
Our findings also confirm the effects of gender in predicting membership to different trajectories of depressive symptoms. Consistent with Costello et al. (2008) and Dekker et al. (2007), females in our sample have a higher probability of manifesting both high and persistent symptoms, and are underrepresented in the low stable trajectories.
Though several previous studies (Hamilton et al., 2014; Rawana & Morgan, 2014; Stringaris et al., 2013) report high prevalence of depressive symptoms in adolescent girls compared to boys, the current results indicate that symptoms should not be attributed to transient moods as they may configure patterns that persist over time. Further, given that gender differences are apparent not only in level but also in persistence of depressive symptoms over the adolescent years (Dekker et al., 2007), addressing gender differences by separate estimation of both number and shape of the latent trajectories, instead of using gender as a time-invariant covariate is most relevant. Future studies should also advance the examination of factors related to high depression risk among adolescent girls, modelling number and shape of trajectories by gender instead of treating gender as a time-invariant covariate. On applied grounds, identification of groups that differ in level and course of symptoms is central for intervention purposes.
In predicting membership to trajectories of depressive symptoms this study examined both parental (i.e., warmth, demandingness, disrespect) and adolescent (i.e., temperament) dimensions. Findings provide evidence for the association between warmth, disrespect and membership to different classes of trajectories of depressive symptoms highlighting the importance of parent characteristics in adolescents’ wellbeing. Maternal warmth not only predicted membership in the low stable trajectory group but was also associated with lower levels of symptoms within three of the classes. Alternatively, maternal disrespect not only decreased membership in the low stable trajectory but was associated to higher depressive symptoms within classes. Though Brendgen et al. (2005) found that parental characteristics predicted class membership, results in our sample point more specifically to the differential effects of parental warmth and disrespect in predicting trajectories of depressive symptoms.
Findings on the association between irritability as a temperamental characteristic and the evolution of depressive symptoms indicate that irritability decreases the odds of belonging to the low stable class. This finding is relevant both on theoretical and applied grounds. Theoretically, these results are in line with a trait thesis of depression whereby a highly reactive temperament serves as a vulnerability factor predisposing children to high levels of depressed mood independently of environmental stressors (e.g., Clark, Watson, & Mineka, 1994). On applied grounds, findings indicate the importance of early diagnosis and treatment to prevent or ameliorate the effects of irritability on depressive symptoms in adolescents.
Current findings provide additional evidence for the heterogeneity in the course of depressive symptoms for adolescents, by using adolescents of both genders and from a different cultural context. The implications of these findings extend beyond adolescence. Because depression interferes with other developmental tasks, it can be assumed that different trajectories of depressive symptoms in adolescence will have consequences for adjustment later in life (Rawana & Morgan, 2014; Wickrama et al., 2009; Yaroslavsky et al., 2013). Future studies should advance knowledge in three important ways. First, designs with longer follow-up are needed to address questions about the evolution of trajectories of depressive symptoms and examination of the developmental consequences of trajectories of depressive symptoms as adolescents move into young adulthood and beyond. This is particularly important for adolescents experiencing fluctuating patterns over time, as observed in the low increasing and high decreasing trajectories. Second, studies should advance the understanding of factors that are associated to the mechanisms that account for adolescents moving in and out of particular trajectories. Finally, because depressive symptoms may elicit the use of psychological control/disrespect by parents or may at least increase adolescents’ perceptions of parents as being controlling, future studies should include multi-source data to control for method variance.
Limitations of the current study include the use of self-report and one-source data in predictor and outcome variables, something that could increase reporter bias. Although, confirmatory factor analysis supported the longitudinal invariance of the depressive symptoms, parental measures (Cumsille et al., 2014) and adolescent irritability (Pérez & Cumsille, 2012) scales, it would have been ideal to incorporate multiple assessment strategies. Unfortunately, this is rarely feasible in large samples.
In spite of these limitations, current findings extend previous research on the course of depressive symptoms as well as on the contribution of parental characteristics and adolescent irritability to the course of depressive symptoms. First, it is the first study to model trajectories of depressive symptoms in a Latin American sample (Chilean), thus providing evidence for the relative universality of the depressive symptoms trajectories previously reported. Both for theoretical and applied purposes (e.g., prevention) it is important to advance knowledge on predictors of different trajectories of depressive symptoms, particularly in Chile where depression is a highly prevalent condition (Vicente, Saldivia, & Kohn, 2012). Second, modeling different trajectories of depressive symptoms can help to identify which adolescents are at risk for developing persistent or recurrent symptoms. Further, identifying groups that show different patterns of symptoms (e.g., chronic, persistent) may help predict the onset of major and minor depressive episodes (Lewinsohn, Clarke, Seeley, & Rohde, 1994), refine developmental theories about the etiology of depressive disorders during adolescence, identify predictors associated with different courses of symptoms, and guide the development of effective preventive or treatment interventions. Third, based on findings that suggest heterogeneity in depressive symptoms across adolescence, this study integrates variable-and person-centered approaches to analyze developmental trajectories (Costello et al., 2008; Von Eye & Bergman, 2003; Von Eye & Spiel, 2010). Fourth, its results provide evidence to ascertain similarities and differences across populations previously studied both in the shape of trajectories and in the contribution of parental dimensions to membership in different trajectories of depressive symptoms.
FundingFunding for this study was provided by Fondo de Desarrollo Científico y Tecnológico, Chile, Fondecyt #1120945.
