



Infecciones de transmisión sexual (ITS) y embarazos no deseados suponen una preocupación actual del sistema de salud pública. Entender los factores (ej. conocimiento, actitudes y habilidades) que influyen la conducta sexual de estudiantes universitarios es crucial para el desarrollo de intervenciones hechas a medida y enfocadas a reducir los riesgos de esta vulnerable población. Los objetivos de este estudio fueron: describir conductas sexuales y analizar diferencias entre géneros en cuanto a conductas sexuales; identificar si existen diferencias entre géneros y grupos de edad en relación con el conocimiento, actitudes y habilidades relacionadas con métodos anticonceptivos e ITS; evaluar la relación del conocimiento con actitudes y habilidades con la conducta sexual de estudiantes universitarios en Portugal. La muestra incluyó 3.278 estudiantes. Los resultados demuestran que la mayoría fue sexualmente activa y usaba condones y anticonceptivos orales. En general los estudiantes universitarios tienen un conocimiento elevado, actitudes positivas y habilidades sobre anticoncepción e ITS. Análisis de género indicaron que las mujeres tenían mayor conocimiento, actitudes más favorables y mejores habilidades. Los estudiantes universitarios, en particular, se enfrentan a nuevos retos en la salud sexual y podrían beneficiarse de una educación más comprensiva destinada a promocionar la toma de decisiones saludables sobre la planificación familiar y prevención de ITS.
Sexually transmitted infections and (STIs) unintended pregnancies are contemporary public health concerns. Understanding factors (e.g. knowledge, attitudes and skills) influencing sexual behaviours of university students are critical to develop targeted and tailored risk-reduction interventions for this vulnerable population. Thus, the goals of this study were to describe sexual behaviours and analyze differences between genders for sexual behaviours; to identify whether differences exist between genders and age groups regarding knowledge, attitudes and skills concerning contraceptive methods and STIs, and to evaluate the association of knowledge with attitudes and skills with sexual behaviour among university students in Portugal. The sample included 3278 students. Results show that the majority were sexually active and use condoms and oral contraceptives. In general, university students have high knowledge, positive attitudes and skills about contraception and STIs. Gender analyses indicated that women had greater knowledge, and more favourable attitudes, and higher skills toward contraceptive and STI preventive behaviour College students, in particular, face new challenges in sexual health and would benefit from more comprehensive education aimed at promoting healthy decision-making about family planning and STI prevention.
Pagina nueva 1
The rates of sexually transmitted infections (STIs) among young people are a major public health concern. Globally, over 100 million STIs occur each year in people under the age of 25 years old (UNAIDS, 2009). According to World Health Organization (2011), at the end of 2010 there were about 34 million people living with HIV infection in the world and 42% of the newly HIV/AIDS infected occur in young people aged between 15 and 24 years old. In Portugal, according to the latest available report from the national monitoring center of sexually transmitted diseases (Centro de Vigilância das Doenças Sexualmente Transmissíveis, 2011), there was a proportional increase in the number of cases of heterosexual transmission among the 20-49 year old cohort, which means that some were infected during adolescence or early adulthood.
In addition to STIs, unintended pregnancies and abortions are also public health concerns for young people (World Health Organization, 2010). According to the World Health Organization, globally, approximately 15 million adolescents are mothers annually (World Health Organization, 2010) and 21.6 million abortions occurred in 2008 in women aged 15 to 44 years old (World Health Organization, 2011). In Portugal, in 2010, 4052 teenagers between 13 and 19 years old were mothers (Instituto Nacional de Estatística, 2011) and in 2010, there were 19,151 abortions in women aged 15 to 44 years but most occurred in young people between 15 and 29 years old (55%) (Direcção Geral de Saúde, 2011)
It is a fact that unprotected sex is one of the main routes of transmission of sexually transmitted infections (e.g. HIV/ AIDS) and unintended pregnancies (Castro & Bermúdez, 2011; Reis, Ramiro, Matos, Diniz, & Simões, 2011). Consequently knowledge, attitudes and behavioural skills concerning contraceptive methods and STIs are crucial factors that influence healthy sexual behaviour (e.g. consistent condom use) (Bermúdez et al., 2012; Ganczak et al., 2007; Reis & Matos, 2007; Reis et al., 2009). According to the empirical literature, possessing correct knowledge and positive attitudes in relation to sexuality or contraception may be sufficient to ensure that young people change their attitudes and their behaviours and therefore use condoms (Reis, Ramiro, Matos, Diniz, & Simões, 2011). It is essential that young people are willing to learn about sexuality, STIs and contraception, to discuss the usage and the election of a contraceptive with their partner and to plan to acquire the chosen contraceptive method; thus increasing their capacity of contraceptive self-efficacy.
Therefore, skill facility in communicating about sex, the capacity to negotiate, self-efficacy to demand use of condoms, as well as positive attitudes towards use of contraceptive methods are important factors predicting their use (Bermúdez et al., 2012; Robinson, Scheltema, & Cherry, 2005).
Furthermore, effective strategies of behavioural change in individuals who engage in sexual activity are needed. Explanatory models of risky sexual behaviour include multiple psychosocial variables. For example according to the model of information-motivation behavioural skills (IMB) - to improve a safer sexual behaviour, the first goal must be to improve knowledge, and then foster motivation (that includes attitudes, behavioural intentions and subjective norms - perceived social support to perform these actions) and behavioural skills (Fisher & Fisher, 1992). The IMB model has been studied in a variety of populations (Bermúdez, Herencia-Leiva, & Uribe Rodríguez, 2009; Fisher, Fisher, Bryan, & Misovich, 2002; Kalichman et al., 2002), including college students (Bazargan, Kelly, Stein, Husaini, & Bazargan, 2000; Fisher, Fisher, Williams, & Malloy, 1994), regarding safe sex. Information and motivation were found to be independent factors, each related to behavioural skills, and behavioural skills were related to preventive behaviours (e.g., condom use discussions, condom accessibility, condom use during sexual intercourse, and HIV antibody testing). Specifically, the model states that information and motivation work through prevention behavioural skills to influence risk reduction behaviours. Moreover, information and motivation are independent constructs, since some people are well informed but may not be motivated to perform preventive behaviours while other people are motivated to perform preventive behaviours but may not be well informed. Information and motivation, however, may relate to behavioural skills which are relevant to risk behaviour changes, such as condom use (Fisher & Fisher, 1992, 1993).
Regarding safe sexual behaviour, several studies consider young people to be a priority group for intervention due to the inconsistent use of contraceptive methods and condoms, the existence of occasional partners and the influence of alcohol and/or drugs in sexual intercourse (Nodin, 2001; Reis & Matos, 2007; Reis et al., 2009). Condoms and birth control pills are the most commonly used contraceptive (American College Health Association , 2009; Matos, Simoes et al., 2011). But for nearly half of unintended pregnancies, contraceptive methods had been used (Finer & Henshaw,
2006), which suggests incorrect or inconsistent use of contraception. To decrease the rates of STIs and unintended pregnancies, it is crucial that sexually active individuals use appropriate contraceptive methods both correctly and consistently. Regarding condoms, it is also important to consider that they are the only birth control method that simultaneously reduce the risk of STIs, including HIV (Reis, Ramiro, Matos, Diniz, & Simoes, 2011).
One study that assessed condom use among university students reported that 83.1% had engaged in unprotected sex at sometime during the past, with women having a higher rate of unprotected sex than men. This study also showed that more than one-third of sexually active students never used condoms in the last three months (Bontempi, Mugno, Bulmer, Danvers, & Vancour, 2009). In Portugal and according to the broadest national study - the HBSC (Health behaviour in school-aged children) - there is an increase in condom and oral contraceptive use from 2002 to 2010 (92.6%, 40% in 2002, 94.1%, 47.1% in 2006, and 95.2%, 53.5% in 2010; respectively) during last sexual intercourse among 8th and 10th grade students; nevertheless, not all adolescents practice sexual preventive behaviours, yet. Males reported higher rates of sexual activity and lower rates of contraception (Matos, Simoes et al., 2011). Another survey among 1402 Portuguese youth between 18 and 25 years old showed that the condom (73.8%) and oral contraceptive (44.2%) were the most commonly used contraceptive methods and a third of young people mentioned having had occasional partners and sexual intercourse under the influence of alcohol or drugs in the last year (Nodin, 2001). Similar findings were also reported in another survey among 436 youth between 18 and 24 years old, which demonstrated that the condom (71.4%) and oral contraceptive (63.2%) were the most commonly used contraceptive methods, 17% mentioned having had occasional partners and 31.4% having had sexual intercourse under the influence of alcohol or drugs in the last year (Reis et al., 2009). Both surveys also demonstrated that men mentioned a higher use of the condom, more occasional partners and sexual intercourse under the influence of alcohol or drugs than women (Nodin, 2001; Reis et al., 2009). Nevertheless none of these Portuguese studies analyzed the difference between age groups.
Concerning knowledge, attitudes and skills in relation to STIs or contraception there is still a need to deepen the study of these variables in order to understand the current needs of young people and then draw up intervention strategies (Bermúdez et al., 2012; Reis & Matos, 2007; Reis et al., 2009; Weinstein, Walsh, & Ward, 2008).
A study assessing knowledge regarding sexually transmitted infections in young people found that around 75% believed they were reasonably well informed regarding STIs, but many underestimated they were at risk for being infected with HIV and/or STIs. Moreover, although almost all participants knew STIs were transmitted via sexual contact, they were unaware of the consequences for untreated STIs (Kaiser Family Foundation, Hoff, Greene, & Davis, 2003). As for gender differences, females were more likely to be familiar with knowledge regarding risk, transmission and long term health implications concerning sexual health (Weinstein et al., 2008).
Reis, Ramiro, Matos, Diniz, & Simões (2011) conducted a study in Portugal in which 7093 young people participated.
They assessed knowledge of preventive sexual behaviour in Portuguese adolescents, including knowledge and attitudes towards HIV/AIDS, and whether they changed from 2002 to 2006. They concluded that there was a reduction of knowledge about how to protect themselves from becoming infected and an increase in the doubts regarding HIV/AIDS. Another survey on knowledge and attitudes about contraception and STIs among university students in Portugal showed that women demonstrated better knowledge and more preventive attitudes to risk-taking, while men demonstrated bigger risk acceptance (Reis & Matos, 2007; Reis et al., 2009).
However Portuguese studies have never analyzed behavioural skills of adolescents and young people nor age differences, which our study aimed to analyse. This is particularly important to study, especially in university context, where they spend a significant part of their lives at a time they are particularly active sexually and consequently when their behavioural skills may be so relevant. A study among university students showed that those who reported having had sex education in previous years had engaged in less risky behaviours than those who didn't (Reis, Ramiro, Matos, & Diniz, 2011), thus suggesting that sex education may have a significant role in prevention.
Behavioural surveillance surveys consist of repeated cross-sectional surveys conducted systematically to monitor changes in HIV, STI and risk behaviours. Besides monitoring, it is also an evaluation tool designed to track trends related to knowledge, attitudes and behaviours in subpopulations that may be prone to infection (Centro de Vigilância das Doenças Sexualmente Transmissíveis, 2011; UNAIDS, 2009, 2011).
This study was developed by using a recent, nationally representative survey. The main objective of the survey was to assess sexual behaviours, knowledge, attitudes and skills concerning contraceptive methods and STIs among students aged 18 to 35 years old. Thus, the goals of this study were a) to describe sexual behaviours and analyze differences between genders for sexual behaviours; b) to identify whether differences exist between genders and age groups regarding knowledge, attitudes and skills concerning contraceptive methods and STIs, and c) to evaluate the association of knowledge with attitudes and skills with sexual behaviour among university students in Portugal.
According to literature we hope to show that: a) condom and oral contraceptives are the most used contraceptive methods, b) men more often than women report engaging in sexual risk behaviours, c) women and younger students have better knowledge, behavioural skills and more positive attitudes concerning contraceptive methods and STIs and d) there is an association between knowledge, attitudes and behavioural skills concerning contraceptive methods and STIs.
Method
Participants
The sample consists of 3278 randomly selected university students in Portugal, between the ages of 18 and 35. It provides national representative data from those attending university during the academic year 2009/2010. Data were collected through a self-administered questionnaire. The sample included 69.7% women and 30.3% men. This percentage is consistent with the gender distribution in the Portuguese university population (Direcção-Geral do Ensino Superior/Ministério da Ciência, Tecnologia e Ensino Superior 2011). The mean age was 21 years old (standard deviation 3). The majority of students were of Portuguese nationality (97.3%), single (95.5%), catholic (71.9%) and heterosexual (96.4%).
Measures
Socio-demographic characteristics were assessed through the following items - gender (male/female), age (included as a continuous variable), nationality (Portuguese, European countries, Brazilian, African countries, other), marital status (single, married, unmarried cohabitation, divorced, widower), religion (Catholic, Protestant, Buddhist, Orthodox, None, other) and sexual orientation (Heterosexual, Homosexual, Bisexual).
Sexual behaviour was assessed through the following behaviours - three questions about first sexual intercourse: age of onset, use of contraceptive method (Yes/No) and which contraceptive method was used; one question about the contraceptive method usually used; and the degree of sexual risk behaviour, which was measured through six behaviours - occasional partners (Yes/No), having had sexual intercourse with alcohol and drugs (Yes/No) and having had an STI, an unintended pregnancy and having made a voluntary interruption of pregnancy (Yes/No). These questions were developed for the purpose of the HBSC research (from which this study derives) and which aimed at studying health and risk behaviours in adolescence (Currie, Samdal, Boyce, & Smith, 2001). The Portuguese version of the scale was used (Matos, Simoes et al., 2011).
Knowledge concerning contraceptive methods was assessed through answers to 14 items developed by the authors and based on literature documenting the importance of knowledge of contraceptive methods (Reis & Matos, 2007). Young people were asked to respond to fourteen questions about contraceptive methods:
1. "The main function of the oral contraceptive is...?"
2. "The oral contraceptive is a contraceptive method with 99% efficiency for...?"
3. "What should a woman do when she forgets to take the oral contraceptive?"
4. "What happens if a woman has diarrhea or vomits and uses the oral contraceptive?"
5. "The main function of the contraceptive adhesive and vaginal ring is...?"
6. "How does a woman use the contraceptive patch properly?"
7. "How does a woman use the vaginal ring correctly?"
8. "What happens if a woman has diarrhea or vomits and uses the contraceptive patch or the vaginal ring?"
9. "What can reduce the effect of the oral contraceptive, the contraceptive patch and the vaginal ring?"
10. "Contraception emergency pill or the morning after pill can be taken..."
11. "The condom is the only method..."
12. "The less effective contraceptive method is..."
13. "Which of the following situations should cause a woman to take contraception emergency pills or the morning after pill?"
14. "In Portugal it is legally possible to make a voluntary abortion at the request of a woman ...?"
Each item has four or five optional answers, but only one is correct. Results vary between 0 and 14, with the highest score being an indicator of higher knowledge regarding contraceptive methods. For this measure Cronbach's alpha was .79.
Knowledge concerning sexual transmitted infections was assessed through the use of 21 items developed by the authors and based on literature documenting the importance of knowledge of STIs (Reis & Matos, 2007). Young people were asked to respond to twenty one questions about STIs:
1. "Is gonorrhoea curable?"
2. "Is syphilis curable?"
3. "Is chlamydia curable?"
4. "The treatment of STIs is more effective if..."
5. "Which of the following statement is false with regard to the treatment of STIs?"
6. "Which of the following symptoms is false to indicate an STI?"
7. "Is there a vaccine for Hepatitis?"
8. "Is there is a vaccine for human papilloma virus?"
9. "Please tick the potentials ways of transmission of HIV:
a) saliva, b) blood, c) urine, d) toilet, e) swimming pools, f) syringes, g) sperm, h) kisses, i) hugs, j) mosquito bite"
10. "During heterosexual intercourse, who has got higher chances of getting infected with HIV (if the partner is infected)?"
11. "Which of the following is true to prevent STIs?"
12. "Which of the statements listed below is false with regard to the transmission of STIs?"
Each item has two, four or five optional answers, but only one is correct. Results vary between 0 and 21, with the highest score being an indicator of higher knowledge regarding STIs. This scale has an acceptable level of internal consistency (alpha= .81).
Attitudes towards contraceptive methods were assessed through use of 11 items selected from the Contraceptive Attitudes Scale (Reis & Matos, 2007). Young people were asked to state their opinion regarding eleven statements about attitudes towards contraceptive methods:
1. "The contraceptive methods increase sexual desire"
2. "The contraceptive methods make sex seem more romantic"
3. I feel I would be comfortable talking about contraception with my friends"
4. "People should use contraceptives regardless of knowing their sexual partner for a longer or shorter time"
5 "The contraceptive methods can really make intercourse more pleasurable"
6. "There is no difficulty in the use of contraceptive methods"
7. "Using contraceptives makes a relationship seem too permanent"
8. "Sex is nice if you use a contraceptive method"
9. " It pays to use contraceptives even though the monetary costs are high"
10. "Contraceptive methods make sex seem too planned"
11. "I feel better about myself when using contraceptive methods"
Students were asked to indicate their level of agreement with the statements using a five-point response format (1= Strongly disagree to 5= Strongly agree). Results can vary between 11 and 55, with the highest score indicating more positive attitudes for contraception use. For this measure, Cronbach's alpha was .83.
Attitudes towards STIs were assessed through use of 27 items selected from the STD Attitudes Scale (Reis & Matos, 2007). Young people were asked to respond to twenty seven statements about attitudes towards STIs:
1. "The way each person lives his/her sexuality is related to how concerned he/she is about contracting an STI"
2. "It's easy to use contraceptive methods that reduce the chances of getting an STI"
3. "Responsible sex is one of the best ways to reduce the risk of an STIs"
4. "Going to the doctor is the best way to prevent the damaging effects an STIs"
5. "Choosing the right sexual partner is important to reduce the risk of getting an STI"
6. "A high rate of STIs should be of public interest"
7. "All people with an STI have an obligation to take their partner to the doctor"
8. "The best way to convince one's sexual partner to join the treatment of an STI is to go to the doctor with him/ her"
9. "When one knows he/she has an STI is it necessary to change one's sexual habits"
10. "It would be very pleasant for me to do a treatment of an STI"
11. "Thinking you can acquire an STI and being sexually active makes you feel nervous"
12. "I do not feel it is insulting to suggest to my sexual partner to use condoms to avoid an STI"
13. "I feel the urge to talk about STIs with my partner"
14. "If I thought I had an STI, I would go to the doctor"
15. "If I thought I had an STI, I would immediately take my partner to make medical examinations me"
16. "It would be comfortable for me to talk about my STI with my partner if sexually active"
17. "Having sex with more than one person and thinking that I can acquire an STI distresses me"
18. "I believe that sexual abstinence is the best way to prevent STIs"
19. "If I had an STI, I would cooperate with people from public health to find ways of preventing STIs"
20. "If I had an STI, I would avoid exposing myself during treatment"
21. "If I had sex with more than one person often, I would do tests quite regularly"
22. "Before you decide to have sex with someone, you must observe all warning signs of a possible STI"
23. "To decrease the possibility of acquiring an STI, the best option is to have a steady sexual partner"
24. "If I suspect that I have an STI, I will avoid having any sexual contact"
25. "The thought of having an STI makes me avoid having sex"
26. "If I could I would support community efforts to control STIs"
27. "I would be willing to work with others on prevention of STIs"
Students were asked to indicate their level of agreement with the statements using a five-point response format (1= Strongly disagree to 5= Strongly agree). Results vary between 27 and 135, the highest score being an indicator of more positive/preventive attitudes towards STIs. This scale has an acceptable level of internal consistency (alpha= .80).
Self-efficacy skills related to safer sexual behaviour were assessed through the use of nine items selected from the Sexual Risk Behaviour Beliefs and Self-efficacy Scales. This scale assessed the degree of self-efficacy for refusing sexual intercourse, self-efficacy for communicating about safer sex and self-efficacy for buying and using condoms (Basen-Engquist et al., 1998). The Portuguese version of the scale was used (Matos, Reis, Ramiro, & Equipa Aventura Social, 2011). Young people were asked to respond to nine statements about self-efficacy for safe sex:
1. "Imagine that you met someone at a party. He or she wants to have sex with you. Even though you are very attracted to each other, you are not ready to have sex. How sure are you that you could keep from having sex?"
2. Imagine that you and your boyfriend or girlfriend have been going together, but you have not had sex. He or she really wants to have sex. Still, you do not feel ready. How sure are you that you could keep from having sex until you feel ready?"
3. Imagine that you and your boyfriend or girlfriend decide to have sex, but he or she will not use a condom (rubber). You do not want to have sex without a condom (rubber). How sure are you that you could keep from having sex, until your partner agrees it is OK to use a condom (rubber)?"
4. Imagine that you and your boyfriend or girlfriend have been having sex but have not used condoms (rubbers). You really want to start using condoms (rubbers). How sure are you that you could tell your partner you want to start using condoms (rubbers)?"
5. "Imagine that you are having sex with someone you just met. You feel it is important to use condoms (rubbers). How sure are you that you could tell that person that you want to use condoms (rubbers)?"
6. "Imagine that you or partner use birth control pills to prevent pregnancy. You want to use condoms (rubbers) to keep from getting STI or HIV. How sure are you that you could convince your partner that you also need to use condoms (rubbers)?"
7. "How sure are you that you could use a condom (rubber) correctly or explain to your partner how to use a condom (rubber) correctly?"
8. If you wanted to get a condom (rubber), how sure are you that you could go to the store and buy one?"
9. "If you decide to have sex, how sure are you that you could have a condom (rubber) with you when you needed it?"
Students were asked to indicate their level of self-efficacy using a five-point response format (1= Strongly unsafe; 5= Strongly safe). Summing items yields a total score ranging from 9 to 45. Students who score high on this scale believe they can effectively practice safer sex behaviours. This scale has an acceptable level of internal consistency (alpha= .86).
All scales were subjected to validation by an expert panel. Prior to carrying out the research, a pilot test was conducted.
Procedure
The national survey "Sexual and Reproductive Health in University Students" (HBSC / SRHUS) - is an extension of the Health Behaviour in School-aged Children (HBSC) study for university students. The HBSC study is a collaborative WHO research, undertaken in 43 countries with the aim to study school-aged behaviour regarding health and risk behaviours in adolescence. Portugal is part of this group of countries since 1996 (Currie et al., 2001).
This cross-sectional study was carried between March and June 2010 with an evaluation protocol that was administered to university students. The 19 universities in the sample were randomly selected from the 144 official national list of universities. The sample was stratified by region: five universities in the North, four in the Centre, five in Lisbon and Tagus Valley, two in Alentejo and three in the Algarve. We established previous contact with the selected universities to have authorization for our research. The sampling unit used in these surveys was the class. In each university, classes were randomly selected to meet the required number of students for each grade in a total of 124 classes. After having received authorization, we solicited voluntary participants to fill out the questionnaires and explained the study's aim. There were no refusals. To protect participants and their anonymity, no information regarding identity requested on the questionnaire. Participants were sitting in individual desks, at a reasonable distance from other participants, thus guaranteeing confidentiality. This study had the approval of a scientific committee, the National Ethics Committee and the National Commission for Data Protection and strictly followed the guidelines for human rights protection.
Data analysis
The data were analyzed using the Statistical Package for Social Sciences (SPSS), version 19 for Windows. Descriptive statistics including frequencies, means and standard deviations were performed to give general descriptions of the data. Sexual behaviour was compared between genders using Chi-square (c2) tests. The analysis of differences between genders and age groups, in terms of knowledge, attitudes and skills on contraceptives and STIs, was evaluated using ANOVA for independent groups. The Pearson correlation coefficient was used to determine the associations between dimensions of knowledge, attitudes and skills. The level for statistical significance was set at p < .05. Only significant results are discussed.
Results
Sexual behaviour
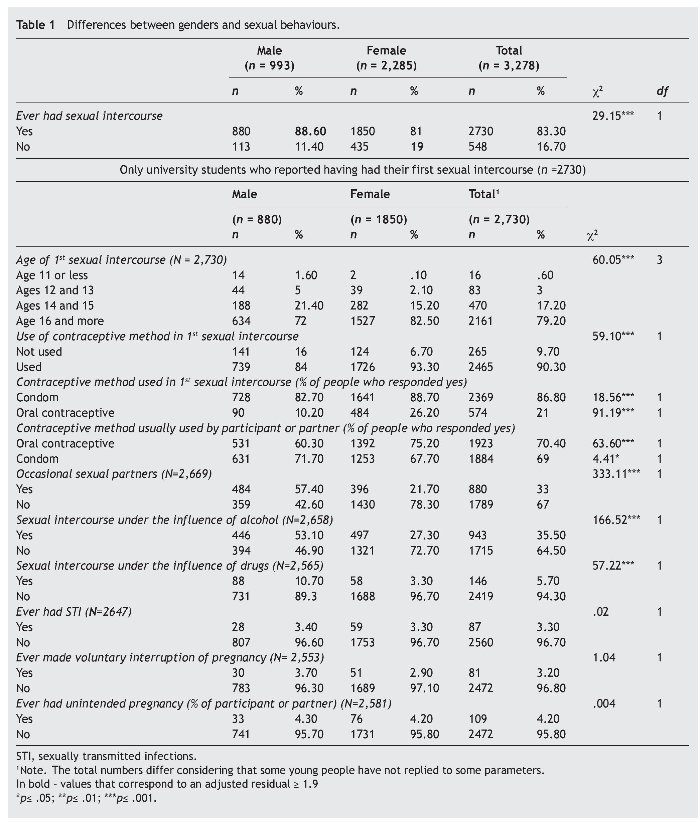
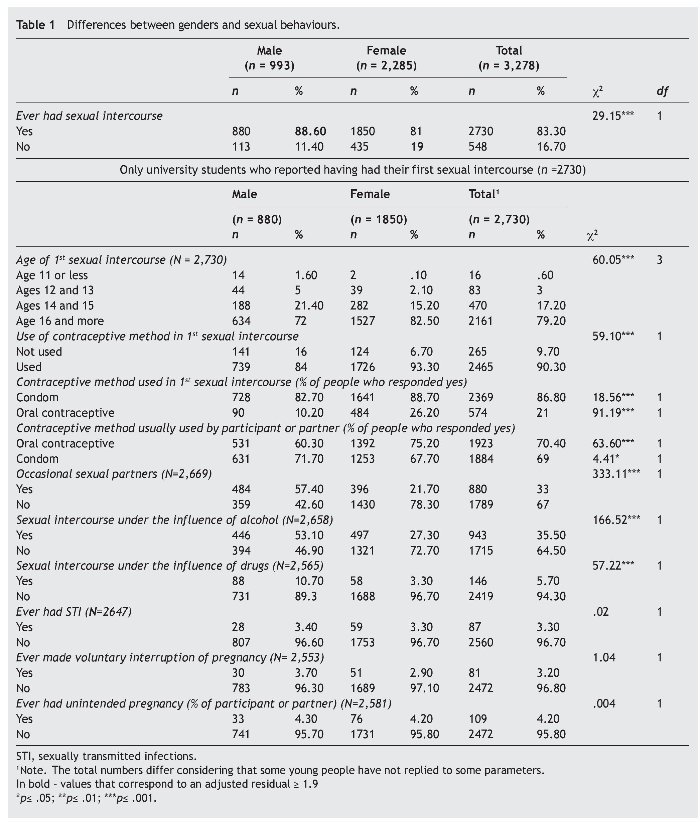
Structured self-reported questionnaires were completed by 3,278 participants, between the ages of 18 and 35. In this sample 83.3% of young people reported a history of sex. Men (88.6%) were more likely to report being sexually experienced than women (81%) (p = .000). Of the students who were sexually experienced, 79.2% reported first sexual intercourse at the age of 16 or later and 90.3% used contraception in their first sexual intercourse, primarily condoms (86.8%). Results showed that, although both the majority of men (72%) and women (82.5%) had their first sexual intercourse at the age of 16 or later, men more often claim to have started sex at a younger age. As for use of a contraceptive method at first sexual intercourse (used by the own or by the partner), a high proportion of men (84%) and women (93.3%) reported contraceptive use, with men (16%) mores than women (6.7%) not using contraception. Regarding the choice of the contraceptive method at first intercourse (used by the own or by the partner), women (88.7%; 26.2%) more often than men (82.7%; 10.2%) report having chosen condoms and the oral contraceptive.
As for usual contraceptive methods (used by the own or by the partner) oral contraceptives (70.4%) and condoms (69%) are the most frequently reported. Significant variation was observed between genders in relation to both oral contraceptive and condom use (p = .036, respectively): women (75.2%) reported using oral contraceptives more often than men (60.3%), while men refer the condom (71.7%) more often than women (67.7%).
Results showed that the majority of men have occasional sexual partners (57.4%) and sexual intercourse under the effect of alcohol (53.1%) (p = .000). Though the rates of sexual intercourse under the influence of drugs is not as high (10.7%) (p = .000) as the other risky sexual behaviours mentioned previously, they still represent a major concern in men's sexual behaviours. And they have all these risky behaviours more frequently than women. Regarding STIs, abortions and unintended pregnancies, 3.3%, 3.2% and 4.2% reported having an STI, abortion and unintended pregnancy. (Table 1).
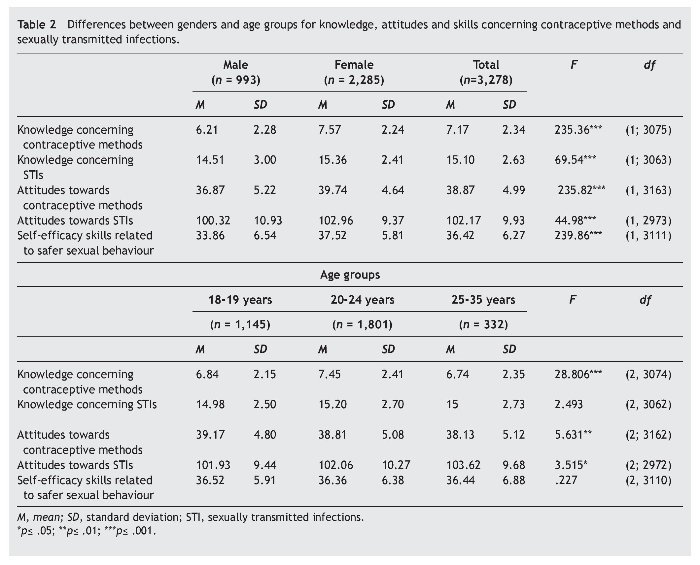
Differences between genders and age groups for knowledge, attitudes and skills concerning contraceptive methods and sexually transmitted infections
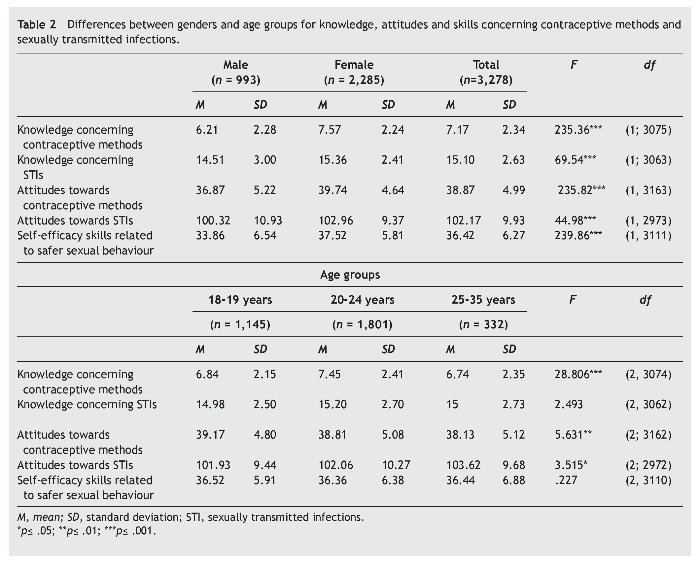
The mean total score in relation to knowledge concerning contraceptive methods and STIs was 7.17 (SD = 2.34) and 15.10 (SD = 2.63), respectively; with men showing significantly less knowledge (M = 6.21, SD = 2.28; M = 14.51, SD = 3, respectively) than women - (M = 7.57, SD = 2.24; M = 15.36, SD = 2.41) (F1, 3075 = 235.36, p = .000; F1, 3063 = 69.54, p = .000)].
The mean total score in relation to attitudes towards contraceptive methods and STIs was 38.87 (SD = 4.99) and 102.17 (SD = 9.93), respectively; with men showing significantly more negative attitudes (M = 36.87, SD = 5.22; M = 100.32, SD = 10.93, respectively) than women - (M = 39.74, SD = 4.64; M = 102.96, SD = 9.37 (F1, 3163 = 235.82, p= .000; F 1, 2973 = 44.98, p = .000).
The level of self-efficacy skills related to safer sexual behaviour among young people was high, as indicated by a total mean score of 36.42 out of 45 points, with females (M = 37.52, SD = 5.81) showing significantly more self-efficacy skills related to safer sexual behaviour than males - (M = 33.86, SD = 6.54 (F1, 3111 = 239.86, p = .000).
Statistically significant differences were found between age groups for knowledge concerning contraceptive methods (F 2, 3074 = 28.806, p = .000) and attitudes towards contraceptive methods and STIs (F 2; 3162 = 5.631, p < .004; F 2; 2972 = 3.515, p = .030). The Post-hoc comparisons by the Games-Howell method indicated that young people aged between 20 - 24 reported having more knowledge about contraceptive methods (M = 7.45, SD = 2.41) when compared with the other two age groups (18-19 years old: M = 6.84, SD = 2.15; 25-35 years old: M = 6.74, SD = 2.35, respectively). Young people aged 18 - 19 years showed significantly more positive attitudes towards contraceptive methods (M = 39.17, SD = 4.80) when compared with older students e (25-35 years old: M = 38.13, SD = 5.12). And young people aged 25-35 years showed significantly more positive/preventive attitudes towards STIs (M = 103.62, SD = 9.68) when compared with the other two age groups (18-19 years old: M = 101.93, SD = 9.44; 20-24 years old: M = 102.06, SD = 10.27, respectively). (table 2).
Bivariate correlations
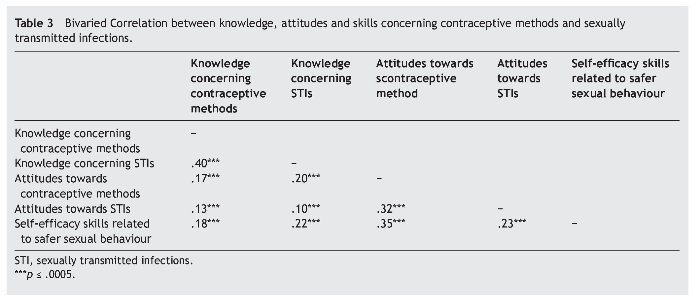
Associations among the variables under study were analyzed through Pearson's correlation. As observed in Table 3, knowledge concerning contraceptive methods was associated in a positive, moderate and statistically significant way with knowledge concerning STIs (r = .40; p = .0005) and in a positive, weak and statistically significant way with attitudes towards contraceptive methods (r = .18; p = .0005), attitudes towards STIs (r = .13; p = .0005) and self-efficacy skills related to safer sexual behaviour (r = .19; p = .0005).
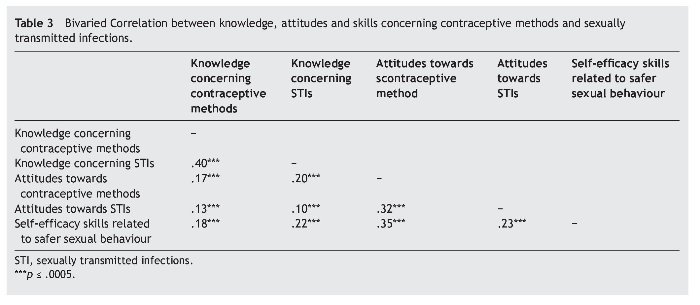
Knowledge concerning STIs was statistically significant, positive and weak in terms of attitudes towards contraceptive methods (r = .20; p = .0005), attitudes towards STIs (r = .11; p = .0005) and self-efficacy skills related to safer sexual behaviour (r = .23; p = .0005).
Attitudes towards contraceptive methods were associated in a positive, moderate and statistically significant way with attitudes towards STIs (r = .32; p = .0005) and self-efficacy skills related to safer sexual behaviour (r = .36; p = .0005).
There was a positive, weak and statistically significant correlation between attitudes towards STIs and self-efficacy skills related to safer sexual behaviour (r = .23; p = .0005).
Discussion
The main aim of the current study was to describe the sexual behaviours of university students in Portugal and assess differences between genders and age groups for knowledge, attitudes and skills concerning contraceptive methods and STIs, and evaluate the association between knowledge, attitudes and skills.
Results showed the majority is sexually active, had their first sexual intercourse at the age of 16 or later, used condom as their first contraceptive method and usually used the oral contraceptive and condom. There also seems to be a general tendency for females to report more use of oral contraceptive than males, which may be explained by the fact that men may not always know if their partner uses the oral contraceptive. As for condom use, in general, men are more likely to report it, possibly as they feel less embarrassed buying and/or carrying them (World Health Organization, 2009). Therefore, these results confirm our first hypothesis and have also been found in other studies (American College Health Association, 2010; Matos, Simoes et al., 2011).
Regarding risk behaviours, it was found that men reported more risk behaviour because they have had more occasional partners and more sex associated with alcohol and drug use. These results confirm our second hypothesis and are corroborated by other researches (Nodin, 2001; Reis et al., 2009).
Concerning STIs, unintended pregnancies and abortions, it was found that a minority of students reported having had at least one of them. Therefore, we have a minority, but worthy of concern, students at risk and this suggests that protective behaviours are not consistent or they are abandoned over time.
Most young people have reasonable knowledge about contraception and STIs, especially women and young people aged between 20- 24 years. They also show positive attitudes and skills towards contraception and STIs. The comparative analysis showed significant variation between genders, where women had more knowledge, attitudes, skills, concerns and preventive behaviours towards risk and men had higher risk acceptance, confirming our third hypothesis in what difference between genders are concerned. Regarding the differences between age groups our hypothesis was not confirmed, because younger people (aged 18 to 19 years) did not produce the best results. It was the group of older youth (aged 25 to 35 years) who had less knowledge, attitudes and behavioural skills in relation to contraception and STIs compared to the other two groups, thus demonstrating that the older university students need interventions on sexual health, possibly because they did not benefit from sex education in middle and high school.
Knowledge of contraceptive methods was positively associated with knowledge of STIs, attitudes and skills, i.e., knowledge, attitudes and skills are fundamental factors to diminish risk behaviour. These results support similar findings by Reis, Ramiro, Matos, Diniz, & Simões (2011) and Synovitz, Herbert, Kelley, and Carlson (2002) and confirm our fourth hypothesis.
Results indicate that young people who are well informed and have more positive attitudes and skills tend to not accept risks, while those who possess less knowledge, less positive attitudes and less skills will more readily accept risks, which is in agreement with the model of information-motivated behavioural skills (IMB) (Fisher & Fisher, 1992; 1993). Knowledge alone about contraception and STIs does not grant a protective effect in relation to preventive sexual behaviour. This means that being well informed about contraception and prevention of STIs does not guarantee that individuals will not perform behaviours that may put them at risk of becoming infected. Motivation and behavioural skills to perform preventive sexual behaviours have significant effects; consequently interventions that promote prevention of sexual behaviour should give emphasis on changing attitudes, perceptions of social support, intentions and skills acquisition.
The increase in knowledge, attitudes and skills is positive in that it suggests that more students are aware of their future options. Substantial proportions of students, however, still do not have correct information, positive attitudes and self-efficacy skills. Furthermore, gender and age group differences in knowledge, attitudes and skills may suggest that education is not reaching the college population equally. In terms of prevention, a continuing emphasis on teaching correct condom use and encouraging regular testing for HIV and other STIs is crucial for the promotion of healthy sexual behaviour.
This study has some limitations. First, because of the sensitive nature of the survey, findings are subject to social desirability bias. Second, there is the possibility of recall bias since respondents were expected to provide information on previous behaviours. Third, that it only represents university students, not all 18-35 year olds.
Conclusion
Findings from the current research have practical implications for both contraceptive education and STI prevention among university students. The data from this survey could be a useful guide in the development of campaigns or programs designed to convey accurate information about contraception and STIs transmission routes and prevention strategies and to dispel erroneous beliefs about sexual risks.
Because young people today prefer smaller families and delay childbearing longer, more family planning is necessary than in the previous generation. Given the greater diversity in contraceptive technology that is available today, young people need increasingly comprehensive education so that they are aware of all of their options. A focus on the advantages and disadvantages of all methods can help students make informed decisions (Kirby, Laris, & Rolleri, 2007). Because not all students go to health centers it is imperative to create a space in university for this exchange of information.
University students in particular face new challenges in sexual health and need more comprehensive education aimed at promoting healthy decision-making about family planning and STI prevention. Present actions can have considerable influence over future decisions; more sexuality education during the college years, when students are exploring sexuality and developing standards for future relationships can lead to greater sexual and reproductive health as adults.
Future directions
The role of communication regarding contraception and STIs prevention including for example condom use efficacy, and refusal self-efficacy related to incidental sex and alcohol/ drug use in the context of sex need further study. Interventions designed specifically for older students that focus on condom promotion and education need to be implemented and evaluated. Condom education that focuses on condom negotiation skills and self-efficacy should be implemented and evaluated for university students. In addition, given the importance of our findings on correlation of alcohol and drugs with unsafe sexual practices, further research regarding the context of substance use behaviours is recommended.
Funding
This study was supported by a FCT grant - (SFRH/ BD/37583/2007) and ACS/CNIVIH/SIDA.
*Corresponding author at:
Faculdade de Motricidade Humana, Estrada da Costa, 1495-688
Cruz Quebrada, Portugal.
E-mail address:reispsmarta@gmail.com (M. Reis).
Received June 25, 2012;
accepted December 4, 2012
References
American College Health Association (2009). American College Health Association-National college health assessment Spring 2008 reference group data report (abridged). Journal of American College Health, 57, 477-488.
Basen-Engquist, K., Mâsse, L. C., Coyle, K., Kirby, D., Parcel, G., Banspach, S., & Nodora, J. (1998). Sexual risk behavior beliefs and self-efficacy scales. Handbook of Sexuality - Related Measures(pp. 541-544). Thousand Oaks: Sage.
Bazargan, M., Kelly, E. M., Stein, J. A., Husaini, B. A., & Bazargan, S. H. (2000). Correlates of HIV risk-taking behaviors among African-American college students: The effect of HIV knowledge, motivation, and behavioural skills. Journal ofthe National Medical Association, 92, 391-404.
Bermúdez, M. P., Herencia-Leiva, A. J., & Uribe Rodríguez, A. F. (2009). Resumen de versiones fuerte y débil del modelo de información-motivación-habilidades conductuales en la predicción del uso del preservativo. Revista Latinoamericana de Psicología, 41, 587-600.
Bermúdez, M. P., Teva, I., Ramiro, M. T., Uribe-Rodríguez, A. F., Carlos, J., & Buela-Casal, G. (2012). Knowledge, misconceptions, self-efficacy and attitudes regarding HIV: Cross-sultural assessmeent and analysis in adolescents. International Journal of Clinical and Health Psychology, 12, 235-249.
Bontempi, J. B., Mugno, R., Bulmer, S. M., Danvers, K., & Vancour, M. L. (2009). Exploring gender differences in the relationship between HIV/STD testing and condom use among undergraduate college students. American Journal of Health Education, 40, 97-105.
Castro, A., & Bermúdez, M. P. (2011). Native and immigrant adolescents in Spain: Adaptation and perceived discrimination as HIV-risk factors. International Journal of Clinical andHealth Psychology, 11, 34-47.
Centro de Vigilância das Doenças Sexualmente Transmissíveis (2011). Infecção VIH / SIDA. A situação em Portugal a 31 de Dezembro de 2010. Lisboa: INSA.
Currie, C., Samdal, O., Boyce, W., & Smith, R. (2001). HBSC, a WHO cross national study: Research protocol for the 2001/2002 survey. Copenhagen: WHO.
Direcção-Geral do Ensino Superior/Ministério da Ciência, Tecnologia e Ensino Superior (2011). Available from: http://www.dges. mctes.pt/DGES/pt [retrieved 3 Dec 2011].
Direcção Geral de Saúde (2011). Relatório dos registos das Interrupções da Gravidez - Dados referentes ao período de Janeiro a Dezembro de 2010. Divisão de Saúde Reprodutiva. Lisboa, Portugal: Direcção Geral de Saúde.
Finer, L. B., & Henshaw, S. K. (2006). Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspectives on Sexual and Reproductive Health, 38, 90-96. Fisher, J., & Fisher, W. (1992). Changing AIDS risk behaviour. Psychological Bulletin, 111, 455-474.
Fisher, J., Fisher, W., Bryan , A., & Misovich, S. (2002). Information- motivation-behavioral skills model-based HIV risk behavior change intervention for inner-city high school youth. Health Psychology; 21, 177-186.
Fisher, J. D., Fisher, W. A., Williams, S. S., & Malloy, T. E. (1994).
Empirical tests of an information-motivation-behavioral skills model of AIDS-preventive behavior with gay men and heterosexual university students. Health Psychology,13, 238-250.
Fisher, W., & Fisher, J. (1993). Understanding and promoting AIDS preventive behaviour: A conceptual model and educational tools. The Canadian Journal of Human Sexuality, 1, 99-106.
Ganczak, M., Barss, P., Alfaresi, F., Almazrouei, S., Muraddad, A., & Al-Maskari, F. (2007). Break the Silence: HIV/AIDS Knowledge, Attitudes, and Educational Needs among Arab University Students in United Arab Emirates. Journal of Adolescent Health, 40, 572-578.
Instituto Nacional de Estatística (2011). Taxas de Natalidade referentes ao ano 2010. Available from: www.ine.pt [retrieved 7 Dec 2011].
Kaiser Family Foundation, Hoff, T., Greene, L., & Davis, J. (2003). National surveyof adolescents and young adults: Sexual health knowledge, attitudes and experiences. Menlo Park, CA: Henry J. Kaiser Family Foundation.
Kalichman, S., Stein, J. A., Malow, R., Averhart, C., Devieux, J., Jennings, T., Prado, G., & Feaster, D. J. (2002). Predicting protected sexual behaviour using the Information-Motivation-Behaviour skills model among adolescent substance abusers in court-ordered treatment. Psychoogyl Health & Medicine, 27, 327-338.
Kirby, D., Laris, B. A., & Rolleri, L. (2007). Sex and HIV education programs: Their impact on sexual behaviors of young people throughout the world. Journal of Adolescent Health, 40, 206-217.
Matos, M. G., Reis, M., Ramiro, L., & Equipa Aventura Social (2011). Saúde sexual e reprodutiva dos estudantes do ensino superior - Relatório do estudo HBSC/SSREU. ACS/FMH/UTL/CMDT-UNL.
Matos, M. G., Simões, C., Tomé, G., Camacho, I., Ferreira, M., Ramiro, L., Reis, M., & Equipa Aventura Social (2011). A Saúde dos adolescentes portuguesesrelatório do estudo HBSC 2010. Lisboa: ACS/FMH/UTL/CMDT-UNL.
Nodin, N. (2001). Os jovens portugueses e a sexualidade em finais do século XX. Lisboa: Associação para o Planeamento da Família. Reis, M., & Matos, M. G. (2007). Knowledge and attitude towards contraceptive methods and STIs among youngsters. Revista Lusófona de Ciências e Tecnologias da Saúde, 4, 23-35.
Reis, M., Ramiro, L., & Matos, M. G. (2009). Contracepção, parceiros ocasionais e consumo de substâncias em jovens portugueses. Revista Lusófona de Ciências e Tecnologias da Saúde, 6, 206-214.
Reis, M., Ramiro, L., Matos, M.G., & Diniz, J.A. (2011). The effects of sex education in promoting sexual and reproductive health in Portuguese university students. Procedia - Social and Behavioral Sciences, 29, 477-485.
Reis, M., Ramiro, L., Matos, M.G., Diniz, J.A., & Simões, C. (2011). Information and attitudes about HIV/Aids in Portuguese adolescents: State of art and changes in a four year period. Psicothema, 23, 260-266.
Robinson, B., Scheltema, K., & Cherry, T. (2005). Risky sexual behaviour in low income African American women: The impact of sexual health variables. The Journal of Sex Research, 42, 224-237.
Synovitz, L., Herbert, E., Kelley, R., & Carlson, G. (2002). Sexual knowledge of college students in a southern state: Relationship to sexuality education results of Louisianna college student study shows need for sexuality programs. AmericanJournal of Health Studies,17, 163-173.
UNAIDS (2009). Joint United Nations Programme on HIV/AIDS.Report on the globalHIV/AIDS epidemic. Available from: http:// data.unaids.org/pub/report/2009/jc1700_epi_update_2009_ en.pdf [retrieved 16 Nov 2011].
UNAIDS (2011). Joint United Nations Programme on HIV/AIDS. Report on the global HIV/AIDS epidemic. Available from: http:// www.unaids.org/en/media/unaids/contentassets/documents/ unaidspublication/2011/JC2216_WorldAIDSday_report_2011_ en.pdf [retrieved 16 Nov 2011].
Weinstein, R. B., Walsh, J. L., & Ward, L. M. (2008). Testing a new measure of sexual health knowledge and its connections to students' sex education, communication, confidence, and condom use. International Journal of Sex Health, 20, 212-221. World Health Organization (2009). A Snapshot of the Health of Young people in Europe. Geneva: WHO.
World Health Organization (2010). Position paper on mainstreaming adolescent pregnancy in efforts tomake pregnancy safer. Geneva, Switzerland: Department of Making Pregnancy Safer: WHO Document Production Services.
World Health Organization (2011). Facts on induced abortion worldwide. Geneva, Switzerland: Department of Reproductive Health and Research. WHO Document Production Services.
