




The aim of the study was to analyze the relationship between being bullied and the physical fitness components, and to determine whether a healthy physical fitness level is related with lower victimization in children and adolescents with overweight and obesity compared to unfit overweight/obese peers. Method:The present cross-sectional study included a total of 7,714 youths (9-17 years), categorized as normal-weight or overweight/obese and fit or unfit according to sex-specific handgrip strength and cardiorespiratory fitness (CRF) cut-points. Bullying (physical, verbal, social exclusion, sexual harassment, and cyberbullying) was assessed through the Standard Health Behavior in School-aged Children survey questions. Results:Boys and girls that were categorized as fit (healthy level of CRF) showed lower traditional bullying compared to unfit counterparts. Also, a healthy level of CRF could be a protective factor of traditional bullying among overweight/obese youths compared to unfit overweight/obese peers. Conclusions:CRF is related with lower risk for experiencing traditional bullying in Latino youths with and without obesity, thus emphasizing the role of fitness even among youth with excess of adiposity.
El objetivo del estudio fue analizar la relación entre el bullying y la condición física, y determinar si un nivel físico saludable está relacionado con menor nivel de victimización en niños y adolescentes con sobrepeso y obesidad en comparación con sus compañeros con sobrepeso u obesidad no aptos. Método:Se incluyó un total de 7.714 niños y adolescentes (9-17 años), categorizados en peso normal o sobrepeso/obeso y aptos o no aptos a través de puntos de corte específicos para la capacidad aeróbica y fuerza manual en esta población. El bullying (físico, verbal, exclusión social, acoso sexual y cyberbullying) se evaluó a través de autoinforme. Resultados:Los jóvenes categorizados como aptos (capacidad cardiorrespiratoria) padecen menos bullying en comparación con sus homólogos no aptos. Además, un nivel saludable de capacidad cardiorrespiratoria se relacionó con menor bullying tradicional entre los jóvenes con sobrepeso/obesidad en comparación con sus homólogos no aptos. Conclusiones:La capacidad cardiorrespiratoria se relaciona con un menor riesgo de sufrir acoso escolar tradicional en los jóvenes latinos con y sin obesidad, lo que enfatiza el papel del buen estado físico incluso entre los jóvenes con exceso de adiposidad.
School bullying has been identified as a type of interpersonal violence between peers in childhood and adolescence, affecting school achievement, prosocial skills, and psychological well-being (e.g., specifically depression, anxiety, self-harm, and suicidal behaviour) for victims (Moore et al., 2017). Bullying victimization refers to the process by which a person is repeatedly and over time exposed to intentional negative actions by their peers (Olweus, 1994). There is evidence suggesting bullying victimization in children and adolescents has enduring effects which may persist into adulthood (deLara, 2018). Experts in the field classified bullying victimization into traditional forms (face to face) and electronic bullying (cyberbullying) (Waasdorp & Bradshaw, 2015). Traditional bullying includes physical contact (pushing, hitting) (i.e., physical bullying) as well as verbal harassment (name calling, teasing) (i.e., verbal bullying), rumor spreading, intentionally excluding a person from a group (i.e., exclusion bullying), and obscene gestures (sexual harassment). More recently, cyberbullying has captured media attention as another form of bullying victimization through the use of electronic devices (i.e. instant messaging, websites, chat room) (Sánchez, Muñoz-Fernández, & Vega-Gea, 2017).
Physical fitness is an important health-related marker across the lifespan (Ortega, Ruiz, Castillo, & Sjostrom, 2008). Also, attaining a high level of physical fitness is associated with a variety of markers of psychological health such as less dyadic loneliness, greater perceived social competence and athletic competence, and teacher-reported adaptive functioning (LaVigne, Hoza, Smith, Shoulberg, & Bukowski, 2016). In addition to potential deleterious effects on social and academic functioning, an increasing body of evidence suggests that verbal bullying victimization (e.g., weight-based teasing) from peers may influence engagement in health behaviors, such as physical activity, especially in overweight and obese youths. Despite physical activity and sedentary behavior (e.g., screen time) have been related with bullying victimization (Merrill & Hanson, 2016), evidence with physical fitness are scarce. As far as we know, only two studies have analyzed the association between physical fitness and bullying victimization in children and adolescents. However, these studies assessed subjectively the physical fitness through the Dartmouth COOP Functional Health Assessment Charts for Adolescents (Wilkins-Shurmer et al., 2003) or included only verbal bullying victimization (Greenleaf, Petrie, & Martin, 2014). On the basis of the cumulative results of these two studies, it is reasonable to expect that bullying victimization also might be related to poor physical fitness. It may be the case that bullied youth have lower levels of physical fitness than youth not bullied. For example, verbal bullying being seems to be related to lower levels of self-esteem, depression, physical self-concept, and physical activity self-efficacy (Greenleaf et al., 2014), which could favor lower physical fitness levels. Therefore, understanding how bullying status relates to whether youth meet or do not meet healthy levels of physical fitness is an important step in assessing whether promoting healthier lifestyles merit further attention in order to prevent bullying and their possible consequences among children and adolescents.
The aim of the present study was to analyze the relationship between being bullied and the physical fitness components, and to determine whether a healthy physical fitness level is related with lower risk for experiencing bullying in Colombian children and adolescents with overweight and obesity compared to unfit peers.
MethodParticipantsWe performed cross-sectional analyses of baseline data from participants in the FUPRECOL study, which was focused on the associations between fitness, health, and non-communicable diseases. We published a complete description of the FUPRECOL study design, methods, and primary outcomes for our current cohort (Ramírez-Vélez, Ojeda-Pardo et al., 2016). The sample comprised of 8,000 healthy Colombian children and adolescents aged 9-17.9 years. In this study, we included a sub-sample (N = 7,714; boys, n = 3,379; girls, n = 4,335). The participants were recruited between April 2012 and June 2015. The children and adolescents were of low to middle socioeconomic status (SES 1-3, as defined by the Colombian government), enrolled in public elementary and high schools (grades 5-11), and resided in the capital district of Bogota in a municipality in the Cundinamarca Department in the Andean region. A convenience sample of volunteers was included and grouped by sex and age in 1-year increments (a total of 9 groups). Individuals with endocrine disorders, psychiatric disorders, pregnancy, cardiovascular disease, systemic infections, asthma, or other physical impairments that made them unable to participate in this study, as well as individuals using any prescribed drugs or actively using illegal or illicit drugs, were excluded from this investigation.
InstrumentsBullying victimization. This content was assessed by means of the Revised Bully/Victim Questionnaire. A previous study has reported a good reliability and validity (Solberg & Olweus, 2003). Youths were asked how often they had been bullied at school in the past couple of months in a variety of different ways: (1) Physical bullying: hitting, kicking, pushing, shoving around, or locking indoors); (2) Verbal bullying: calling mean names and making fun of or teasing in a hurtful way; (3) Social exclusion bullying: socially excluding others and spreading rumors; (4) Sexual harassment: sexual comments, jokes, gestures, or looks; and (5) Cyberbullying: bullying using a computer or e-mail messages or pictures, and bullying using a cell phone. The questionnaire consists of seven items answered on a five-point scale: “none”, “only once or twice”, “2 or 3 times a month”, “about once a week”, and “several times a week”. Bullying victimization was categorized as traditional bullying (physical, verbal, social exclusion, and sexual harassment) and cyberbullying. A previous study recommended the cut-point of “2 or 3 times a month” to code a student as bullied or non-bullied (Solberg & Olweus, 2003). The scale presents a Cronbach's alpha of .75.
Anthropometric assessment. All data was collected at the same time in the morning, between 7:00 a.m. and 10:00 a.m. Body weight and height were measured following standard procedures using an electronic scale (Tanita® BC544, Tokyo, Japan) and a mechanical stadiometer platform (Seca® 206, Hamburg, Germany), respectively. Body Mass Index (BMI) was calculated as body weight in kilograms divided by the square of height in meters. BMI was classified as underweight, normal weight, overweight, or obese using the International Obesity Task Force criteria for age and sex (Monasta, Lobstein, Cole, Vignerová, & Cattaneo, 2011). In all measures, we found almost excellent test-retest reliability (body weight [intraclass correlation coefficient [ICC] = .98], height [ICC = .97], and BMI [ICC = .89].
Physical Fitness Assessment. The musculoskeletal component used is appropriate for this age group and has shown acceptable validity and reliability (Ramírez-Vélez, Martínez et al., 2016; Ramírez-Vélez, Morales et al., 2017). Handgrip strength was assessed as an indicator of upper-body MF using an adjustable analogue handgrip dynamometer, T-18 TKK SMEDLY III® (Takei Scientific Instruments Co. Ltd., Niigata, Japan). Students were shown a brief demonstration of technique, and were given verbal instructions on how to perform the test. The dynamometer was adjusted according to the child's hand size per predetermined protocols. Youth were classified as fit or unfit based on the sex-and age cut-points established among Colombian children and adolescents (Ramírez-Vélez, Peña-Ibagon et al., 2017). Handgrip measurement in a subsample (n = 229, similar in demographics and biological characteristics to the whole sample) was recorded to ensure reproducibility on the day of the study. The reproducibility of our data was R = .96 to the handgrip test.
Cardiorespiratory fitness (CRF) was assessed with the 20 meter Shuttle Run Test (20mSRT) (Ramírez-Vélez, Palacios López et al., 2016). This test requires participants to run back and forth between two lines set 20 m apart. Running speed started at 8.5km/h and increased by 0.5km/h each minute, reaching 18.0km/h per minute. Each level was announced on a recorded audio. The participants were instructed to keep up with the pace until exhausted. The test was finished when the participant failed to reach the end lines concurrent with the audio signals on two consecutive occasions. Otherwise, the test ended when the subject stopped because of fatigue. The participants received verbal encouragement from the investigators to achieve maximum performance to keep running as long as possible. The number of shuttles performed by each participant was recorded. To estimate VO2max using the 20mSRT, the equation developed by Barnett equation for boys and girls, VO2max = 25.8 × [6.6 × G × 0.2 × (body mass + 3.2 × (final speed)], where G is gender (male = 0; female = 1) and final speed (8 + 0.5 × last stage completed), was used (Barnett, Chan, & Bruce, 1993). Youth were classified as fit or unfit based on the sex-and age cut-points established among Colombian children and adolescents (Ramírez-Vélez, Correa-Bautista, Mota, & Garcia-Hermoso, 2018). The reproducibility of our data was R = .84. Intra-rater reliability was assessed by determining the ICC (.96, CI 95% .95 to .97).
Screen time. Screen time was assessed by asking participants to report the number of hours per typical day in the past seven days with a question: “Approximately how many hours a day do you usually watch television in your free time?”. Television use was dichotomized (< 2h/day; ≥2h/day) based on international guidance on limiting pediatric screen time (Bar-On et al., 2001). Previous studies have been related the screen time with higher bullying victimization (Merrill & Hanson, 2016).
Maturation Status Assessment. Maturation status (self-reported) was assessed by the classification described by Tanner (five stages: I–V) (Tanner & Whitehouse, 1976). Each participant entered into an isolated room where, using a set of images exemplifying the various stages of sexual maturation, they categorized the development of their own genitalia (for boys), breasts (for girls), armpits (for boys), and pubic hair (for both sexes). The reproducibility of our data was R = .84.
ProcedureThe study protocol was explained verbally to the participants and their parents/guardians before they gave their written consent. Participation in the study was fully voluntary and anonymous, with no incentives provided to participants. The Review Committee for Research on Human Subjects at the University of Rosario (code No. CEI-ABN026-000262) approved all study procedures. The protocol was in accordance with the latest revision of the Declaration of Helsinki and current Colombian laws governing clinical research on human subjects (Resolution 008430/1993 Ministry of Health).
Data analysesThe normality of the variables was verified using histograms and Q-Q plots. VO2max and handgrip strength/weight had skewed distributions and were log-transformed prior to analyses. To aid interpretation, data was back-transformed from the log scale for presentation in the results. Since no significant interaction (i.e., p>.10) was observed between age group (children or adolescents; e.g., age group x bullying victimization) to increase statistical power, all the statistical analyses were performed with both age groups together.
First, we tested associations between traditional bullying, cyberbullying, age, sex, pubertal status, BMI, excessive television use, cardiorespiratory fitness, and muscular strength by computing zero-order correlations using Pearson correlations.
Differences were analyzed using the chi-square test (χ2) in order to explore each group (fit vs. unfit). Analyses of covariance (ANCOVA) were used to assess the differences between mean cardiorespiratory fitness (ml/kg/min) and handgrip strength/weight according to bullying victimization categories (non-bullied vs bullied), adjusted for age, pubertal status, overweight/obesity, and excessive television use (≥ 2h/day).
To examine the odds of bullying victimization (Odds Ratio [OR] and 95% confidence interval) in fit but overweight/obesity youths compared to unfit and overweight/obesity peers, we used multinomial logistic regression. The first model was not adjusted. The second model was adjusted for age, pubertal status, and excessive television use (≥ 2h/day). We used SPSS V. 21.0 software for Windows (SPSS, Chicago, IL, USA). Statistical significance was set at p < .05.
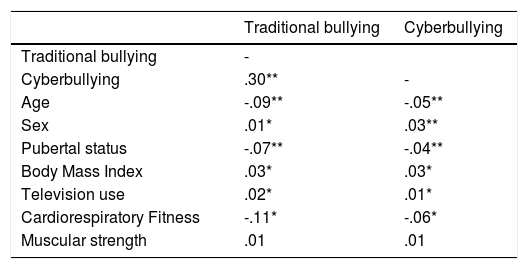
ResultsAs presented in Table 1, there were positive zero-order correlations between traditional bullying and cyberbullying with sex, BMI, television use and CRF. Also, there were negative correlations between traditional bullying and cyberbullying and age and pubertal status.
Correlations between traditional bullying, cyberbullying, age, sex, pubertal status, body mass index, excessive television use, cardiorespiratory fitness, and muscular strength.
| Traditional bullying | Cyberbullying | |
|---|---|---|
| Traditional bullying | - | |
| Cyberbullying | .30** | - |
| Age | -.09** | -.05** |
| Sex | .01* | .03** |
| Pubertal status | -.07** | -.04** |
| Body Mass Index | .03* | .03* |
| Television use | .02* | .01* |
| Cardiorespiratory Fitness | -.11* | -.06* |
| Muscular strength | .01 | .01 |
*p< .05; **p< .001
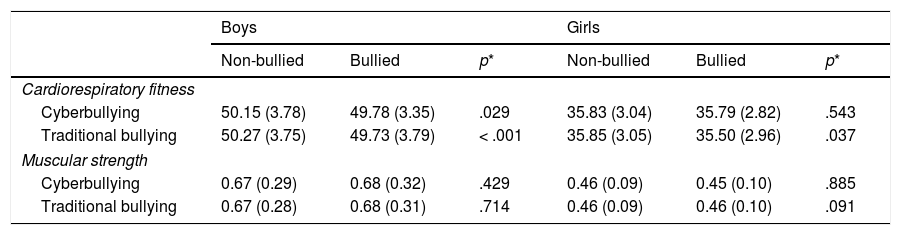
Table 2 shows differences between mean CRF (ml/kg/min) and handgrip strength/weight according to bullying victimization categories (non-bullied vs bullied) by sex. Non-bullied boys and girls show higher VO2max values in traditional bullying compared to bullied peers. Also, non-bullied boys show higher CRF in cyberbullying compared to bullied counterparts.
Differences between mean cardiorespiratory fitness (ml/kg/min) and handgrip strength/weight according to bullying victimization categories by sex.
| Boys | Girls | |||||
|---|---|---|---|---|---|---|
| Non-bullied | Bullied | p* | Non-bullied | Bullied | p* | |
| Cardiorespiratory fitness | ||||||
| Cyberbullying | 50.15 (3.78) | 49.78 (3.35) | .029 | 35.83 (3.04) | 35.79 (2.82) | .543 |
| Traditional bullying | 50.27 (3.75) | 49.73 (3.79) | < .001 | 35.85 (3.05) | 35.50 (2.96) | .037 |
| Muscular strength | ||||||
| Cyberbullying | 0.67 (0.29) | 0.68 (0.32) | .429 | 0.46 (0.09) | 0.45 (0.10) | .885 |
| Traditional bullying | 0.67 (0.28) | 0.68 (0.31) | .714 | 0.46 (0.09) | 0.46 (0.10) | .091 |
* Analysis adjusted for age, pubertal status, overweight/obesity, and excessive television use (≥ 2h/day).
Prevalence of bullied youths according to fitness categories (fit and unfit) by sex are despite in Figure 1. Fit boys (22.7% vs. 27.7%, p= .018) and girls (22.0% vs. 25.2%, p= .023) (for CRF) showed lower prevalence of traditional bullying victimization compared to unfit counterparts.
 by sex (* p< .05).")
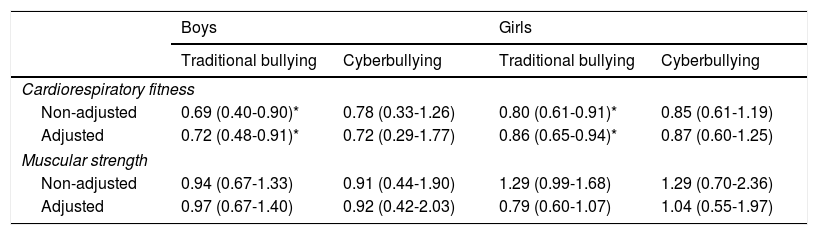
Finally, multiple logistic regressions predicting victimization in fit but overweight/obesity youths compared to unfit and overweight/obesity (fatness peers) is shown in Table 3. In CRF, fit but overweight/obesity boys (non-adjusted: OR=0.69 95% CI, 0.40 to 0.90, p= .012; adjusted: OR=0.72 95% CI, 0.48 to 0.91, p= .018) and girls (non-adjusted: OR=0.80 95% CI, 0.61 to 0.91, p= .023; adjusted: OR=0.87 95% CI, 0.65 to 0.94, p= .030) showed lower likelihood to traditional bullying. In muscular strength, not significant association was found.
Odds of bullying victimization in fit but overweight/obesity youths compared to unfit and overweight/obesity peers by sex.
| Boys | Girls | |||
|---|---|---|---|---|
| Traditional bullying | Cyberbullying | Traditional bullying | Cyberbullying | |
| Cardiorespiratory fitness | ||||
| Non-adjusted | 0.69 (0.40-0.90)* | 0.78 (0.33-1.26) | 0.80 (0.61-0.91)* | 0.85 (0.61-1.19) |
| Adjusted | 0.72 (0.48-0.91)* | 0.72 (0.29-1.77) | 0.86 (0.65-0.94)* | 0.87 (0.60-1.25) |
| Muscular strength | ||||
| Non-adjusted | 0.94 (0.67-1.33) | 0.91 (0.44-1.90) | 1.29 (0.99-1.68) | 1.29 (0.70-2.36) |
| Adjusted | 0.97 (0.67-1.40) | 0.92 (0.42-2.03) | 0.79 (0.60-1.07) | 1.04 (0.55-1.97) |
Note. Analysis adjusted by age, pubertal status, and excessive television use (≥ 2h/day). *p< .05
This is the first study examining the relationship between physical fitness assessed objectively and different bullying victimization types among children and adolescents. The findings from the present study indicate that (1) CRF is related with lower risk for experiencing traditional bullying in both boys and girls; and (2) a healthy level of CRF could be a protective factor of bullying victimization among overweight/obese youths. These findings contribute to the current knowledge by adding evidence about the role of physical fitness in terms of a possible protective factor of bullying victimization and their possible consequences.
The corpus of evidence to date suggests that the promotion of physical fitness in children and adolescents has few detriments and many potential benefits (Ortega et al., 2008), thus additional efforts to better understanding on how bullying might contribute to physical fitness are important. Research demonstrates that victims of bullying often experience low self-esteem, depression, anxiety, insecurity, oversensitivity, introversion, and withdrawal from social activities; therefore, higher levels of physical fitness could favor higher well-being in children and adolescents. A previous study in 222 US children ages 10-14 years shows a significant association between physical fitness and psychological well-being for both boys and girls (LaVigne et al., 2016). Our study provides evidence about the association between physical fitness and bullying victimization. Specifically, CRF and a healthy level associated with lower cardiometabolic risk (Ramírez-Vélez et al., 2018), seems to be a protective factor of being bullied (traditional bullying victimization) in both boys and girls. These findings are in line with a study published by Wilkins-Shurmer et al. Wilkins-Shurmer et al.(2003) which reported that lower physical fitness were associated with increased frequency of bullying over the last five days for both boys and girls. However, the relationship between victimization over the term and physical fitness was only evident in those experiencing the highest frequency of bullying. Also, it has been proven that children and adolescents who perform athletic skills well are treated favorably by their peers (Sweeting & West, 2001) and therefore, youths in poor physical condition could be more likely to become victims (i.e., bullies take advantage of their physical weaknesses) (Ma, 2004). It was suggested that it may be the case that bullying leads to decreased levels of physical activity self-efficacy and motivation to avoid physical activity (Greenleaf et al., 2014), which, in turn, may contribute to lower levels of physical fitness and vice versa.
In this study, we further aimed to test the phenotype known as “fat but fit” (McAuley & Blair, 2011) in terms of bullying victimization. Several studies suggested that overweight and obese youth are at substantially greater risk for experiencing teasing than their normal-weight peers (Losekam, Goetzky, Kraeling, Rief, & Hilbert, 2010). Consequently, children and adolescents who informed that they had been the targets of peer victimization (i.e., physical and verbal aggression) reported lower levels of physical activity when compared to non-victimized counterparts (Storch et al., 2006), which could benefit lower physical fitness level. Greenleaf et al.(2014) showed that adolescents who were teased (i.e. verbal bullying) about being overweight completed fewer PACER laps and had lower levels of upper body muscular strength fitness than participants who said they were not teased. In turn, our study suggested that a healthy level of CRF was related with lower risk for experiencing traditional bullying among overweight/obese youths. These youths with optimal level of CRF may have higher perceived physical ability and perceived physical appearance leading to a greater involvement on physical activities (Strong et al., 2005). Therefore, may appear less vulnerable and prone to experience bullying because they are more likely to be involved in protective behaviors such as participating in sports or being connected to school and peers (Merrill & Hanson, 2016). Following an evolutionary framework, previous studies consider that bullying is inherent in various animals because it promotes access to physical and social resources (Book, Volk, & Hosker, 2012). It means that children and adolescents who have more physical fitness can attain social reward of status and acceptance (Strong et al., 2005). Our study could show that youths with a healthy level of CRF carry a reputation in the social group and are perceived as being tough, which could protects them from being targeted for bullying.
The results of our study cannot be applied to the general population without some caution. Firstly, the study population was drawn from schoolchildren who attended a public school and may not be fully representative of the community. Secondly, due to the cross-sectional nature of the study design, we are unable to draw causal relationships. Thus, we are unable to deduce whether low fitness leads to higher odds of the bullying victimization, or conversely, whether victimization leads to poor physical fitness. Thirdly, our study may be biased towards under-representation of socially disadvantaged adolescents. The literature would indicate that bullying is more prevalent in schools with a higher proportion of socially disadvantaged students (Wilkins-Shurmer et al., 2003). Finally, it is likely that additional parameters, such as body image, loneliness, and disordered eating, will be important to include in future studies in order to gain a fuller picture of youths’ experiences of bullying victimization.
ConclusionsIn conclusion, this study reveals the association between bullying victimization and objectively measured CRF in Latino youths with and without overweight/obesity. From a public health perspective, promoting a physical activity program at school could be an effective strategy for increase physical fitness (Pozuelo-Carrascosa, García-Hermoso, Álvarez-Bueno, Sánchez-López, & Martinez-Vizcaino, 2018) and maybe bullying protection during the school years. For example, the school curriculum could integrate physical activities to improve student's physical fitness and consequently self-image, physical appearance and cooperation with peers.
FundingThe FUPRECOL Study was carried out with the financial support of Instituto Colombiano para el Desarrollo de la Ciencia y la Tecnología “Francisco José de Caldas” COLCIENCIAS (Contract N° 671-2014 Code 122265743978). This article presents independent research commissioned by COLCIENCIAS under its Programme Grants for Applied Research funding scheme (Convocatoria 671-2014). The content of this paper reflects the author's views alone, and the Colombian Community or the COLCIENCIAS is not liable for any use that may be made of the information contained herein.
We thank the children and adolescents who participated in the study and their parents and teachers for their collaboration. We also acknowledge the members involved in fieldwork for their effort, particularly physical activity and health masters students for their work in the field-based fitness assessment. The authors wish to thank C. A. C. Coloma, for revision of the English text.
