










Poor sleep quality is a prevalent health issue among adolescents, and few studies have examined the variables affecting adolescents’ sleep quality from the perspective of the co-occurrence of sleep issues and anxiety disorders. Therefore, the current study investigated whether the cognitive model of generalized anxiety disorder applies to adolescents’ sleep quality.
MethodIn Study 1, a total of 2042 adolescents were recruited and they completed questionnaires relating to worry, intolerance of uncertainty (IU), negative problem orientation (NPO), cognitive avoidance (CA), and sleep quality. In Study 2, a total of 379 adolescents participated in a six-month longitudinal survey to verify the model that was obtained in Study 1.
ResultsStudy 1 showed the modified cognitive model of generalized anxiety disorder can be applied to adolescents’ sleep quality. Specifically, IU was a higher-order vulnerability factor that directly affected worry, and indirectly fostered worry via NPO and CA, where worry only mediated the relationships between IU, NPO, and sleep quality. However, CA exerted no independent effect on worry or sleep quality beyond the influences of IU and NPO, therefore, it dropped out of the final model. Study 2 partially confirmed the above model again from the longitudinal perspective.
ConclusionThe present study constructs a new model to explain adolescents’ sleep quality, providing a foundation for future interventions.
Poor sleep quality is a common health problem among adolescents. Prior research indicates that the occurrence of insomnia symptoms in Chinese adolescents ranges from 3.4% to 12.2% (Zhang et al., 2016), leading to several unfavorable consequences (Chiang et al., 2017; Roach et al., 2021). By now, there is a vast amount of literature exploring factors that affect adolescents’ poor sleep quality, mainly focusing on individual traits, social environmental factors, and mental disorders (Brown et al., 2018; Lin et al., 2019; Zou et al., 2023). Although researchers have noted the impact of mental disorders on sleep quality, there has been limited research on the underlying factors influencing poor sleep quality in adolescents, particularly with regard to comorbidity factors. Numerous studies have documented that anxiety often co-occurs with poor sleep quality (Baglioni et al., 2016; Blake et al., 2018; Cox & Olatunji, 2020). In particular, generalized anxiety disorder (GAD) is one of the most common anxiety disorders that is found in individuals with poor sleep quality (Hertenstein et al., 2019; Nguyen et al., 2022), suggesting that poor sleep quality and GAD may share the same pathological processes. Since the cognitive model of GAD is usually the most persuasive model to explain the occurrence, maintenance, and development of GAD (Dugas et al., 1998), this study aims to investigate whether this model can be applied to adolescents’ sleep quality from both cross-sectional and longitudinal perspectives.
The cognitive model of generalized anxiety disorderDugas et al. (1998) proposed a cognitive model of generalized anxiety disorder (GAD) that identifies four frequent cognitive components: intolerance of uncertainty (IU), negative problem orientation (NPO), cognitive avoidance (CA), and worry. In this model, intolerance of uncertainty (IU) refers to a cognitive bias whereby individuals perceive uncertainty as distressing and aversive that significant efforts are adopted to avoid it (Dugas et al., 1998; Dugas, 2000). It is typically the cornerstone of this model, which not only directly increases the risk of excessive worrying but also functions as a higher-order vulnerability factor for worry by predisposing individuals toward cognitive avoidance and negative problem orientation (Dugas et al., 1998). Negative problem orientation (NPO) describes a dysfunctional cognitive set of minds about a person's cognitive approach when faced with solving problems (Maydeu-Olivares & D'Zurilla, 1996). Meanwhile, cognitive avoidance (CA) indicates a person's tendency to use avoidance strategies when confronted with intrusive thoughts (Dugas et al., 1998; Dugas, Savard, et al., 2007). Both of them can lead to persistent worry, leaving the individual vulnerable to the full spectrum of anxiety symptoms (Borkovec et al., 1983; Koerner et al., 2020).
Combined with the cognitive-behavioral theory, IU is a dispositional characteristic that results from a set of acutely sensitive deep-seated beliefs that become activated in response to ambiguous situations (Koerner et al., 2020). Similarly, both cognitive avoidance and a negative approach to problem-solving, as intermediate beliefs, were specific strategies and attitudes for individuals to cope with uncertainty, which further serves to sustain and exacerbate their worries and anxiety. Excessive and uncontrollable worry is superficial automatic thought, being observed easily in patients with GAD. Due to the high co-occurrence rate of generalized anxiety disorder and poor sleep quality (Hertenstein et al., 2019; Nguyen et al., 2022), the following step is to explain the sleep quality of adolescents from the viewpoint of the cognitive model of GAD.
Explaining the adolescents’ sleep quality from the cognitive model of GADThe relationships between IU, NPO, CA, worry, and adolescents’ sleep qualityNumerous empirical studies have indicated that IU is closely associated with adolescents’ sleep quality (Clementi & Alfano, 2014; Lin et al., 2017; Tsypes et al., 2013). For instance, Bélanger et al. (2004) have found that GAD patients with higher IU tend to experience poor sleep quality such as prolonged sleep latency and reduced sleep duration. Similarly, intervention studies have also suggested that decreasing IU levels can lead to an improvement in patients’ sleep quality (Clementi & Alfano, 2014). These pieces of evidence provide preliminary support for the claim that IU may be a crucial factor affecting adolescents’ sleep quality.
Similarly, both CA and NPO may affect sleep quality in adolescents. On the one hand, existing studies have demonstrated that the maintenance of poor sleep quality is closely linked to CA (Capková et al., 2018; Ree et al., 2005; Scotta et al., 2022). For example, individuals with poor sleep quality tended to experience more intrusive and uncontrollable rumination thoughts during the pre-bed period compared to those with good sleep quality (Scotta et al., 2022). Certain intervention research has indicated that attempting to proceed with the thought control strategy during nighttime can potentially exacerbate sleep disorder symptoms (Ree et al., 2005). On the other hand, some studies also found that those with poor sleep quality had elevated levels of NPO (O'Kearney & Pech, 2015; Pech, 2012). Based on this, we predicted that CA and NPO may be significant factors in adolescents’ sleep quality.
Worry is also a core element of adolescents’ sleep quality based on the perspective of the cognitive model of sleep disturbance (Harvey, 2002; Clancy et al., 2020; Yan et al., 2013). Empirical studies have revealed that individuals with high levels of worry experience lower sleep efficiency compared to those with low levels of worry, and they tend to spend more time maintaining light sleep for longer (Clancy et al., 2020; Lin et al., 2017). Consequently, we predicted that worry played a crucial role in determining adolescents’ sleep quality.
Constructing the cognitive model of adolescents’ sleep quality and competitive modelsCombining the above evidence with the cognitive model of GAD (Dugas et al., 1998; Koerner et al., 2020), IU, as a core belief, may be a higher-order vulnerability factor that directly increases the risk of worry, which is considered as the automatic thought. For example, Lin et al. (2017) have found IU can predict sleep quality via the mediation of worry. Meanwhile, IU also indirectly intensify the likelihood of worry via NPO and CA, which were treated as intermediate beliefs. Ultimately, all of them may leave the individual susceptible to poor sleep quality. Consequently, the cognitive model of adolescents’ sleep quality was constructed (M1; also named the mixed path model).
However, two competing models were also constructed to explain the influencing factors of sleep quality in adolescents. First, previous studies found four cognitive components, including IU, CA, NPO, and worry, directly affected adolescents’ sleep quality (Capková et al., 2018; Clementi & Alfano, 2014; Pech, 2012; Tousignant et al., 2019). Therefore, a short-range path model (M2) was constructed, in which these four cognitive variables directly affected adolescents’ sleep quality. Second, according to the cognitive model of sleep disturbance (Harvey, 2002), worry is the core factor for people's poor sleep quality, which might play a mediation role in the relationships between IU, CA, NPO, and sleep quality. Theoretically, people who have poor sleep quality usually worry about uncertainty, and they may simultaneously adopt pessimistic attitudes and avoidance strategies to resist their concerns and fears regarding sleep, resulting in poor sleep quality (Dugas, 2000; Gosselin et al., 2007), Based on these findings, a long-range path model (M3) was constructed, in which IU, CA, and NPO simultaneously affected adolescents’ sleep quality through the mediating effect of worry. All models were shown in Fig. 1.
Present study
In summary, the current studies aimed to construct a model that explains adolescents’ sleep quality from the perspective of comorbidity between poor sleep quality and GAD. In Study 1, we selected the suitable model to explain adolescents’ sleep quality by comparing three competing models from a cross-sectional perspective. Study 2 verified the model obtained in Study 1 from a longitudinal perspective. The model constructed in Studies 1 and 2 can serve as a theoretical foundation for future interventions aimed at improving adolescents’ sleep quality.
Study 1: The applicability of the cognitive model of GAD in adolescent sleep quality: Based on a cross-sectional perspectiveMethodParticipantsA Monte Carlo power analysis was conducted to estimate the required sample size (Wang & Rhemtulla, 2021), assuming standardized factor loadings of 0.70, standardized regression coefficients of 0.40, and the randomly set residual variances. It suggested that a minimum sample size of 250 participants had already achieved more than 80% power for each target effect after simulating 1000 times. To obtain representative samples, a total of 2042 adolescents with ages ranging from 10 to 19 years old (mean age = 14.29 years, SD = 1.61) were recruited from five schools in the present study via a stratified cluster. Grade level was the basis for stratification, with 12 classes chosen from each of Grades 7, 8, 10, and 11, resulting in a total of 48 participating classes. Students in Grades 9 and 12 did not participate due to exam preparations. All participants completed the questionnaires in class, which were administrated by their head teacher and a postgraduate majoring in psychology. The local institution approved the study and written informed consent was acquired from the participants’ head teachers and parents. Finally, in this sample, 1022 were boys (50.00%) and 1002 were girls (49.10%), and 18 people didn't fill in gender. The numbers of students in Grades 7, 8, 10, and 11 were 516 (25.30%), 519 (25.40%), 537 (26.30%), and 463 (22.70%), and 7 people didn't fill in grades.
MeasurementPittsburgh sleep quality index (PSQI)PSQI was widely used to assess the subjective sleep quality of an individual in the past month (Buysse et al., 1989). It contains seven subdimensions that measure different aspects of sleep quality (e.g., “During the past month, what time have you usually gone to bed at night?”), including subjective sleep quality (SSQ), sleep latency (SL), sleep duration (SDT), habitual sleep efficiency (HSE), sleep disturbance (SD), used sleep medicine (USM), and daytime dysfunction (DD). All items were rated on a 4-point Likert scale ranging from 0 to 3, with higher scores implying poor sleep quality. The Chinese version of PSQI had good reliability and validity (Liu et al., 1996). In this study, the internal consistency for PSQI was 0.65.
Short version of the intolerance of uncertainty scale (IUS-12)IUS-12 was applied to assess the extent to which individuals experience distress and perceive uncertainty as unacceptable (Carleton et al., 2007). It includes 12 items which are comprised of two factors, namely prospective IU (7 items; e.g., “I should be able to organize everything in advance”) and inhibitory IU (5 items; e.g., “Uncertainty keeps me from living a full life”). All items were rated on a 5-point Likert scale ranging from 1(“not typical at all”) to 5(“very typical”), with higher scores indicating greater IU. IUS-12 demonstrated good internal consistency and validity (Carleton et al., 2007). In the current study, the internal consistency for IUS-12 and its dimensions were 0.84, 0.70, and 0.76, respectively.
Abbreviated Penn state worry questionnaire (PSWQ-A)PSWQ-A was employed to measure both frequency and intensity of worry (Hopko et al., 2003). It contained 8 items and all of them were rated on a 5-point Likert scale (e.g., “Many situations make me worry”), ranging from 1 (“not typical at all”) to 5 (“very typical”). Higher scores indicated a greater tendency to worry. The Chinese version of PSWQ-A had good reliability and validity in the Chinese adolescent sample (Xie et al., 2023). The Cronbach's of PSWQ-A in the current study was 0.88.
Negative problem orientation questionnaire (NPOQ)NPOQ is a 12-item questionnaire that was used to assess a dysfunctional cognitive set of negative problem orientation (Robichaud & Dugas, 2005). All items were rated on a 5-point Likert scale, ranging from 1 (“not typical at all”) to 5 (“very typical”). The total score ranged from 12 to 60, and higher scores indicated a higher tendency to adopt negative problem orientation (e.g., “I see problems as a threat to my well-being”). The Chinese version of NPOQ had good reliability and validity in the Chinese adolescent sample (Xiao et al., 2020). The Cronbach's of NPOQ in the current study was 0.93.
Cognitive avoidance questionnaire (CAQ)CAQ was used to measure the tendency of cognitive avoidance strategies when addressing threatening intrusive thoughts (Sexton & Dugas, 2008). CAQ contained 25 items measuring five types of cognitive avoidance strategies, including thought suppression, thought substitution, distraction, avoidance of threatening stimuli, and transformation of images into thoughts. All items were rated on a 5-point Likert scale, ranging from 1 (“not typical at all”) to 5 (“very typical”). Higher scores indicated a greater tendency for cognitive avoidance (e.g., “There are things that I would rather not think about”). The Chinese version of CAQ demonstrated good reliability and validity in the Chinese adolescent sample (Xie et al., 2022). The Cronbach's of CAQ and its subdimension in the current study were 0.91, 0.72, 0.69, 0.67, 0.79, and 0.73, respectively.
Data analytic strategyThe statistical analysis was carried out using SPSS 25.0 and Mplus 8.3. First, descriptive statistics and Pearson correlations were performed. Second, gender and grade differences on PSQI were tested by independent t-tests and one-way ANOVAs. Third, structural equation modeling (SEM) was employed to confirm the applicability of the cognitive model of GAD for adolescents’ sleep quality. Full information maximum likelihood (FIML) and bootstrapping using 1000 iterations were respectively conducted to deal with missing data, as well as, examine indirect effects and confidence interval estimation. When establishing SEM models, item parceling was performed. Since IUS-12 and CAQ were multidimensional questionnaires, isolated parceling was implicated (Wu & Wen, 2011). NPOQ and PSWQ-A were one-dimensional questionnaires, therefore, we parceled items based on whether their item numbers were odd or even (Matsunaga, 2008).
ResultsPrimary analysisDescriptive statistics and Pearson correlations for all study variables were provided in Table 1. The sleep quality index score for adolescents is 5.72. According to the critical criteria for sleep disorders (PSQI > 7; Liu et al., 1996), the number of detected cases of sleep disorders in adolescents is 449, with a detection rate of 22.51%. The skewness and kurtosis of all variables ranged from −0.65 to 1.15, which was less than 2 (Finney & DiStefano, 2006), suggesting that all variables were close to the normal distribution. Therefore, all SEM parameters were estimated by maximum likelihood estimation (ML). Moreover, the results of the correlation showed that PSQI was positively associated with IU, CA, worry, and NPO (rs = 0.27 ∼ 0.43). Additionally, gender difference (t(1975) = −5.18, p < .001, Cohen's d = .23) and grades difference (F(3, 1984) = 4.05, p = .01, ¿2 = .01) were found in PSQI. Consequently, gender and grade were considered as control variables in the subsequent analysis.
Descriptive statistics and the Pearson correlations of study variables (n = 2042).
| Variables | M ± SD | Skewness | Kurtosis | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|---|---|
| 1 PSQI | 5.72 ± 2.81 | 0.69 | 1.15 | 1 | ||||
| 2 worry | 24.26 ± 7.68 | −0.21 | −0.51 | 0.43⁎⁎ | 1 | |||
| 3 IU | 37.10 ± 8.79 | −0.35 | 0.34 | 0.37⁎⁎ | 0.72⁎⁎ | 1 | ||
| 4 NPOQ | 28.64 ± 11.60 | 0.29 | −0.65 | 0.43⁎⁎ | 0.65⁎⁎ | 0.60⁎⁎ | 1 | |
| 5 CAQ | 74.94 ± 18.50 | −0.20 | 0.11 | 0.27⁎⁎ | 0.50⁎⁎ | 0.57⁎⁎ | 0.43⁎⁎ | 1 |
Note: PSQI: Sleep quality; IU: Intolerance of uncertainty; NPOQ: Negative problem orientation; CAQ: Cognitive avoidance;
A confirmatory factor analysis was performed to test the measurement model, which is a precondition for structural equation modeling (SEM). The fit indices of the five-factor model were as follows: χ2 = 1065.617, df = 125, χ2/df = 8.52, CFI = 0.938, TLI = 0.924, RMSEA = 0.061, SRMR = 0.048, showing that the five measuring variables were suitable for further establishing the SEM model. The factor loadings of all items reached 0.40, except for three items: sleep duration (SDT, β = 0.29, p <0.001), habitual sleep efficiency (HSE, β = 0.23, p < 0.001), and used sleep medicine (USM, β = 0.24, p < 0.001). Due to the large number of zero values contained in the three dimensions of the PSQI after transformation, their factor loadings were relatively low. To convey information more accurately, we treated the PSQI as an observed variable for subsequent analysis.
Controlling gender and grade, SEM was constructed to compare three models to choose the suitable model (in Table 2). All models were satisfied with the criterion (Wen et al., 2004). However, compared to the short-range path model, the mixed path model not only saved one degree of freedom but also had no significant increase in the Chi-square value. Also, although the long-range model saved four degrees of freedom, the Chi-square value increased a lot. On this basis, the mixed path model was chosen.
Therein, direct paths “from IU to PSQI”, “from CA to PSQI”, and “from CA to worry” were non-significant and they were deleted gradually. Finally, the fitting indices of the revised cognitive model of adolescents’ sleep quality reached a good level (χ2 = 532.309, df = 70, χ2/df = 7.60, RMSEA = 0.057, CFI = 0.970, TLI = 0.962, SRMR = 0.045). And the standardized path coefficients are presented in Fig. 2. To maintain the simplicity of Fig. 2, parcelled items have been omitted.
.")
In this model, IU significantly and positively predicted PSQI independently through the mediating effect of negative problem orientation (0.18 [0.13, 0.23]) and worry (0.20 [0.15, 0.25]), as well as, the chain mediating effect of “from NPO to worry” (0.05 [0.03, 0.07]).
The current study confirmed that the revised cognitive model of GAD applies to explaining adolescents’ sleep quality. Specifically, IU not only affected adolescents’ sleep quality through worry and NPO, but also through the chain mediation starting from NPO leading to worry. However, CA did not have a separate impact on worry or PSQI beyond the influences of IU and NPO, and it was excluded from the final model. Since this study is a cross-sectional study, it didn't effectively demonstrate the causal relationship between variables. Therefore, Study 2 adopts longitudinal data at two time periods to validate this mode again.
Study 2: Re-examination of the cognitive model of adolescents’ sleep quality: Based on a longitudinal perspectiveMethodParticipantsA total of 408 adolescents from Grades 7 and 11 participated in a six-month follow-up survey (Sept. 2019 and Jan. 2020). All participants completed IUS-12, PSWQ-A, NPOQ, and PSQI at time 1 and time 2. After the questionnaires were collected, a primary check was conducted. And it was found that 29 people had missing data. Finally, a sample of 379 adolescents was retained (The dropout rate of 7.00%, mean age = 13.67 years, SD = 1.56). In the available sample, 190 were boys (50.10%) and 189 were girls (49.90%). The numbers of students in Grades 7 and 10 were 199 (52.50%) and 180 (47.5%).
MeasurementAll measurements which were used in Study 2 were the same as in Study 1. The internal consistency coefficients of IUS-12, PSWQ-A, NPOQ, and PSQI that were assessed at time 1 were 0.80, 0.84, 0.90, and 0.62, respectively. And their internal consistency coefficients that were assessed at time 2 were 0.87, 0.88, 0.93, and 0.64.
Data analytic strategyThe statistical analysis was carried out using SPSS 25.0 and Mplus 8.3. First, descriptive statistics and Pearson correlations were performed. Second, structural equation modeling (SEM) was employed to examine the measurement model of all four variables. The item parceling was the same as in Study 1. Then, the measurement invariance across time (e.g., configural, metric, scalar, and error invariances) was calculated to provide a prerequisite for subsequent cross-lagged analysis. Third, based on the cognitive model of adolescents’ sleep quality obtained in Study 1, the cross-lagged model was conducted (Cole & Maxwell, 2003). Fourth, to further understand the potential longitudinal mediating role of worry, NPO, and the chain “from NPO to worry,” SEM with bootstrapping analysis (bootstrap = 1000) was performed. Specifically, we analyzed whether T1 NPO, T1 worry, and the chain “from T1 NPO to T1 worry” mediated the relationship between T1 IU and T2 PSQI while controlling for gender and grade.
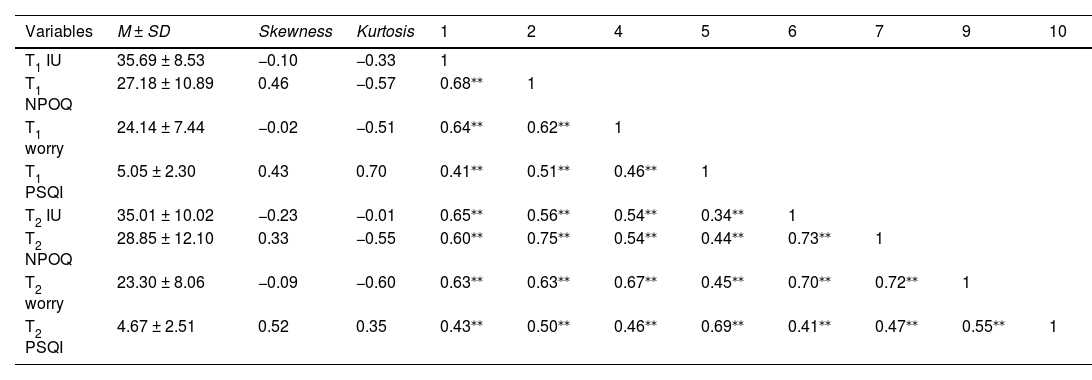
ResultsPrimary analysisDescriptive statistics and Pearson correlations for all study variables were provided in Table 3. The skewness and kurtosis of all variables ranged from −0.60 to 0.70, which was less than 2 (Finney & DiStefano, 2006), suggesting that all variables were close to the normal distribution. Meanwhile, there were moderate to high correlations between variables at times 1 and 2.
Descriptive statistics and correlation coefficients for variables in the longitudinal sample.
| Variables | M ± SD | Skewness | Kurtosis | 1 | 2 | 4 | 5 | 6 | 7 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 IU | 35.69 ± 8.53 | −0.10 | −0.33 | 1 | |||||||
| T1 NPOQ | 27.18 ± 10.89 | 0.46 | −0.57 | 0.68⁎⁎ | 1 | ||||||
| T1 worry | 24.14 ± 7.44 | −0.02 | −0.51 | 0.64⁎⁎ | 0.62⁎⁎ | 1 | |||||
| T1 PSQI | 5.05 ± 2.30 | 0.43 | 0.70 | 0.41⁎⁎ | 0.51⁎⁎ | 0.46⁎⁎ | 1 | ||||
| T2 IU | 35.01 ± 10.02 | −0.23 | −0.01 | 0.65⁎⁎ | 0.56⁎⁎ | 0.54⁎⁎ | 0.34⁎⁎ | 1 | |||
| T2 NPOQ | 28.85 ± 12.10 | 0.33 | −0.55 | 0.60⁎⁎ | 0.75⁎⁎ | 0.54⁎⁎ | 0.44⁎⁎ | 0.73⁎⁎ | 1 | ||
| T2 worry | 23.30 ± 8.06 | −0.09 | −0.60 | 0.63⁎⁎ | 0.63⁎⁎ | 0.67⁎⁎ | 0.45⁎⁎ | 0.70⁎⁎ | 0.72⁎⁎ | 1 | |
| T2 PSQI | 4.67 ± 2.51 | 0.52 | 0.35 | 0.43⁎⁎ | 0.50⁎⁎ | 0.46⁎⁎ | 0.69⁎⁎ | 0.41⁎⁎ | 0.47⁎⁎ | 0.55⁎⁎ | 1 |
Note: PSQI: Sleep quality; IU: Intolerance of uncertainty; NPOQ: Negative problem orientation; CAQ: Cognitive avoidance;
The measurement model with all four constructs correlated in two time periods was assessed by confirmatory factor analysis (CFA) and showed acceptable fit: χ2 = 585.790, df = 181, χ2/df = 3.24, RMSEA = 0.077, CFI = 0.922, TLI = 0.901, SRMR = 0.054.
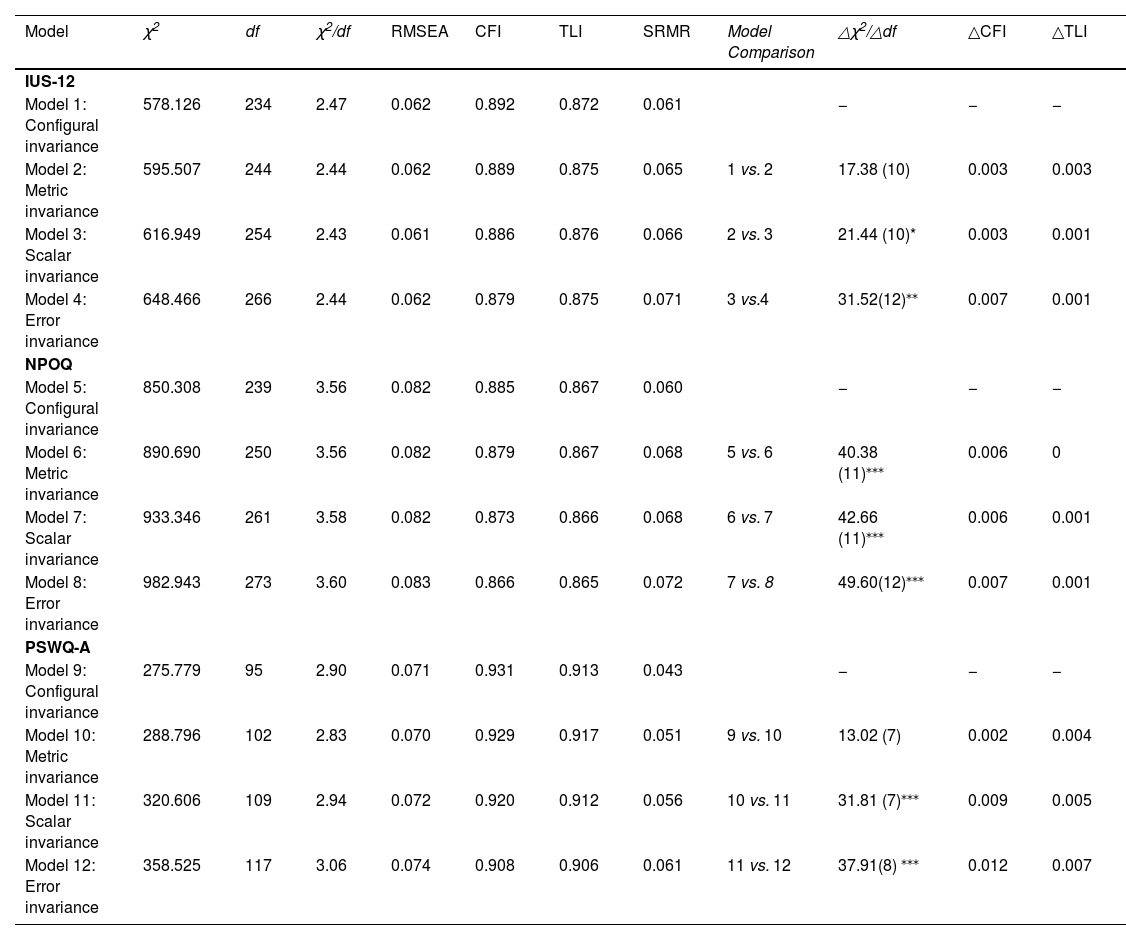
In addition, the measurement invariance for indicators across time was examined (In Table 4). According to the changes in χ2, IUS-12 and PSWQ-A reached metric invariance, while NPOQ reached configural invariance. However, according to Cheung and Rensvold (2002), when a change in CFI and TLI is less than or equal to 0.01, it can be seen there was no significant change in model fit, thereby avoiding sample size sensitivity problems with the χ2 test. Based on this, IUS-12 and NPOQ reached error variance invariance with both △CFI and △TLI less than 0.01, whereas PSWQ-A achieved scalar variance invariance. These results provided a prerequisite for subsequent cross-lagged analysis.
Measurement invariance of IUS-12, NPOQ, and PSWQ-A across times.
| Model | χ2 | df | χ2/df | RMSEA | CFI | TLI | SRMR | Model Comparison | △χ2/△df | △CFI | △TLI |
|---|---|---|---|---|---|---|---|---|---|---|---|
| IUS-12 | |||||||||||
| Model 1: Configural invariance | 578.126 | 234 | 2.47 | 0.062 | 0.892 | 0.872 | 0.061 | − | − | − | |
| Model 2: Metric invariance | 595.507 | 244 | 2.44 | 0.062 | 0.889 | 0.875 | 0.065 | 1 vs. 2 | 17.38 (10) | 0.003 | 0.003 |
| Model 3: Scalar invariance | 616.949 | 254 | 2.43 | 0.061 | 0.886 | 0.876 | 0.066 | 2 vs. 3 | 21.44 (10)* | 0.003 | 0.001 |
| Model 4: Error invariance | 648.466 | 266 | 2.44 | 0.062 | 0.879 | 0.875 | 0.071 | 3 vs.4 | 31.52(12)⁎⁎ | 0.007 | 0.001 |
| NPOQ | |||||||||||
| Model 5: Configural invariance | 850.308 | 239 | 3.56 | 0.082 | 0.885 | 0.867 | 0.060 | − | − | − | |
| Model 6: Metric invariance | 890.690 | 250 | 3.56 | 0.082 | 0.879 | 0.867 | 0.068 | 5 vs. 6 | 40.38 (11)⁎⁎⁎ | 0.006 | 0 |
| Model 7: Scalar invariance | 933.346 | 261 | 3.58 | 0.082 | 0.873 | 0.866 | 0.068 | 6 vs. 7 | 42.66 (11)⁎⁎⁎ | 0.006 | 0.001 |
| Model 8: Error invariance | 982.943 | 273 | 3.60 | 0.083 | 0.866 | 0.865 | 0.072 | 7 vs. 8 | 49.60(12)⁎⁎⁎ | 0.007 | 0.001 |
| PSWQ-A | |||||||||||
| Model 9: Configural invariance | 275.779 | 95 | 2.90 | 0.071 | 0.931 | 0.913 | 0.043 | − | − | − | |
| Model 10: Metric invariance | 288.796 | 102 | 2.83 | 0.070 | 0.929 | 0.917 | 0.051 | 9 vs. 10 | 13.02 (7) | 0.002 | 0.004 |
| Model 11: Scalar invariance | 320.606 | 109 | 2.94 | 0.072 | 0.920 | 0.912 | 0.056 | 10 vs. 11 | 31.81 (7)⁎⁎⁎ | 0.009 | 0.005 |
| Model 12: Error invariance | 358.525 | 117 | 3.06 | 0.074 | 0.908 | 0.906 | 0.061 | 11 vs. 12 | 37.91(8) ⁎⁎⁎ | 0.012 | 0.007 |
Note:
According to the recommendations of Cole and Maxwell (2003) and the cognitive model of adolescents’ sleep quality obtained in Study 1, we constructed an autoregressive cross-lagged model to examine the directional association among all research variables. The results showed that the fitting indexes of the cross-lagged panel model achieved acceptable: χ2 = 220.876, df = 82, χ2/df = 2.69, RMSEA = 0.067, CFI = 0.968, TLI = 0.953, SRMR = 0.053. As Fig. 3 indicated, IU at time 1 was a significant positive predictor of worry (β = 0.29, SE = 0.10, 95% CI = [0.09, 0.48]) and NPO (β = 0.18, SE = 0.08, 95% CI = [0.03, 0.33]) at time 2. Simultaneously, NPO at time 1 was a significant predictor of worry at time 2 (β = 0.18, SE = 0.08, 95% CI = [0.02, 0.33]). Both worry (β = 0.13, SE = 0.06, 95% CI = [0.003, 0.25]) and NPO (β = 0.15, SE = 0.06, 95% CI = [0.03, 0.28]) at time 1 were a significant predictor of PSQI at time 2. These results demonstrated that IU longitudinally predicted NPO and worry, and NPO also longitudinally predicted worry. Similarly, both worry and NPO predicted adolescents’ sleep quality in the long run. To maintain the simplicity of Fig. 3, parcelled items have been omitted.
Longitudinal mediation model.")
SEM and the bootstrapping method were used to test the mediation model with gender and grade as controlling variables (In Fig. 4). The results showed that the mediation model fit the data well, χ2 = 31.135, df = 22, χ2/df = 1.42, RMSEA = 0.033, CFI = 0.994, TLI = 0.991, SRMR = 0.051. Specifically, all paths were significant, except for the path from NPO to worry which was marginally significant (β = 0.21, p = 0.07). In this model, IU significantly and positively predicted PSQI independently through the longitudinal mediating effect of negative problem orientation (0.29 [0.15, 0.43]) and worry (0.14 [0.02, 0.26]). However, the longitudinal chain mediating effect of “from NPO to worry” (0.04 [−0.01, 0.09]) was non-significant. Study 2 partially validated the cognitive model of adolescents’ sleep quality from a longitudinal perspective.
General discussion.")
The present study is based on the cognitive model of GAD, targeting adolescents as participants, and using both cross-sectional and longitudinal data to preliminary test and verify the applicability of the cognitive model of GAD on adolescents’ sleep quality. Study 1 found that the mixed path model was better than the short/long-range path model. In the mixed path model, IU not only increased adolescents’ worry, but also acted as a higher-order vulnerability factor for CA and NPO. Meanwhile, worry mediated the relationships between IU, NPO, and poor sleep quality. However, CA had no independent influence on worry or PSQI beyond the influences of IU and NPO, resulting in its exclusion from the final model. Study 2 partially validated the cognitive model of adolescents’ sleep quality through a longitudinal sample. Therefore, the results supported the modified cognitive model of GAD applied to adolescents’ sleep quality.
The applicability of the cognitive model of GAD to adolescents’ sleep qualityIn Study 1, comparing the three competing models, the mixed path model is the best, suggesting that the effects of IU, NPO, CA and worry on adolescents’ sleep quality operate at different levels. Concretely, IU serves as a higher-order vulnerability factor for both NPO and CA, explaining almost identical amounts of variance in NPO and CA. Meanwhile, separate significant pathways were found between IU, NPO, and worry, with IU being the strongest predictor. It is consistent with previous studies that claim people who have poor sleep quality tend to interpret ambiguous stimuli in a threat-related manner, which is proposed to underlie pre-sleep worry (Gerlach et al., 2020; Harvey, 2002; Lin et al., 2017). However, CA had no independent influence on worry or PSQI beyond the effects of IU and NPO; therefore, it was left out of the final model. This result contrasts with previous studies that have found avoidance is closely associated with poor sleep quality and worry (Harvey, 2002; Kim et al., 2022; Ree et al., 2005). Nevertheless, the measurement of CA used in this study includes multiple strategies, such as distraction. Previous research has demonstrated that distraction strategies can improve sleep quality more effectively (Capková et al., 2018), which may explain why the non-significant direct relationship between CA and sleep quality in the present study.
In Study 2, all paths of the cognitive model of adolescents’ sleep quality are significant, except for the path from NPO to worry which is marginally significant. It contrasts with a previous study, which has claimed that targeting NPO decreases the contribution that trait worry plays in insomnia maintenance or in relapse (O'Kearney & Pech, 2015). We speculate that the reason for the inconsistency may be the relatively small number of people in the longitudinal sample. Further research can verify this pathway again.
Taken together, this study provided preliminary yet robust evidence that, with some modifications, the GAD cognitive model proposed by Dugas et al. (1998) applies to adolescents’ sleep quality.
Cognitive mechanisms affecting adolescents’ sleep qualityCombining with cognitive-behavioral theory, a linear causal relationship exists among core belief, intermediate belief, automatic thought, and psychological disorders (Beck, 1995; Koerner & Dugas, 2006). In the present study, IU can be defined as the core belief triggering adolescents’ poor sleep quality. It is located at the starting point of the linear chain, serves as the distal factor in adolescents’ poor sleep quality, and affects the strength and occurrence of the linear causal relationship. NPO represents intermediate belief, which is located in the middle of the causal linear chain, and reflects attitudes adopted to prevent adolescents’ poor sleep quality. Although CA has not been confirmed in the model of present study, it may still be an intermediate belief used as strategies for individuals with poor sleep quality based on previous studies highlighting the significant impact of CA on sleep quality (Capková et al., 2018). Worry is the most frequent automatic thought experienced by adolescents (David et al., 2018; O'Kearney & Pech, 2015). It is located at the end of the causal linear chain and serves as the most direct cause and the intrinsic mechanism underlying adolescents’ poor sleep quality (Fig. 5). Based on this model, we can apply targeted cognitive-behavioral therapy to effectively treat adolescents’ poor sleep quality in the future.
Strengths, limitation, and future research
The current study is the first to explore the applicability of the cognitive model of GAD to adolescents’ sleep quality from both cross-sectional and longitudinal perspectives, thereby extending upon relevant theories relating to sleep. Furthermore, it provides a theoretical foundation for future interventions targeting poor sleep quality in adolescents. Nevertheless, there are several limitations to the present study that need to be considered. First, the study only used self-report questions to measure subjective sleep quality, and objective sleep quality could be assessed in future research. Second, the questionnaires used in this study to measure IU, CA, NPO, and worry were not specifically designed for sleep-related issues, which might lead to insufficient validation of the proposed model. In future research, other more targeted questionnaires can be used. Third, although the cognitive model of GAD was tested on adolescents’ sleep quality, it remained unclear whether this model applied to children or adults. A prior study have found that there are some differences in the cognitive model of GAD among adult, adolescent, and child samples (Fialko et al., 2012), highlighting the need for subsequent studies in these populations.
