




Breast cancer is the most common malignancy in women, but only 6% of newly diagnosed patients have distant metastasis at diagnosis.1 Metastatic spreading disease to the gastrointestinal tract is very rare.2 Here we report a case of bowel metastasis as the initial presentation of lobular breast carcinoma.
A 67-year-old female presented with six months of diffuse abdominal pain, diarrhea and weight loss. She had a past history of dyslipidemia, currently medicated with simvastatin. Abdominal examination was unremarkable. Laboratory investigation and upper endoscopy were normal. Colonoscopy revealed eodema and loss of vascular pattern in the ascending colon and cecum; the ileocecal valve presented marked erythema and friability, preventing ileoscopy (Fig. 1A). Pathologic evaluation of biopsies from the ileocecal valve showed poorly cohesive tumor cells in lamina propria and some signet ring cells (Fig. 1B); immunohistochemistry was positive for estrogen receptor (Fig. 1C), cytokeratin 7 and AE1/AE3. These findings were consistent with metastatic lobular breast carcinoma to the colon.
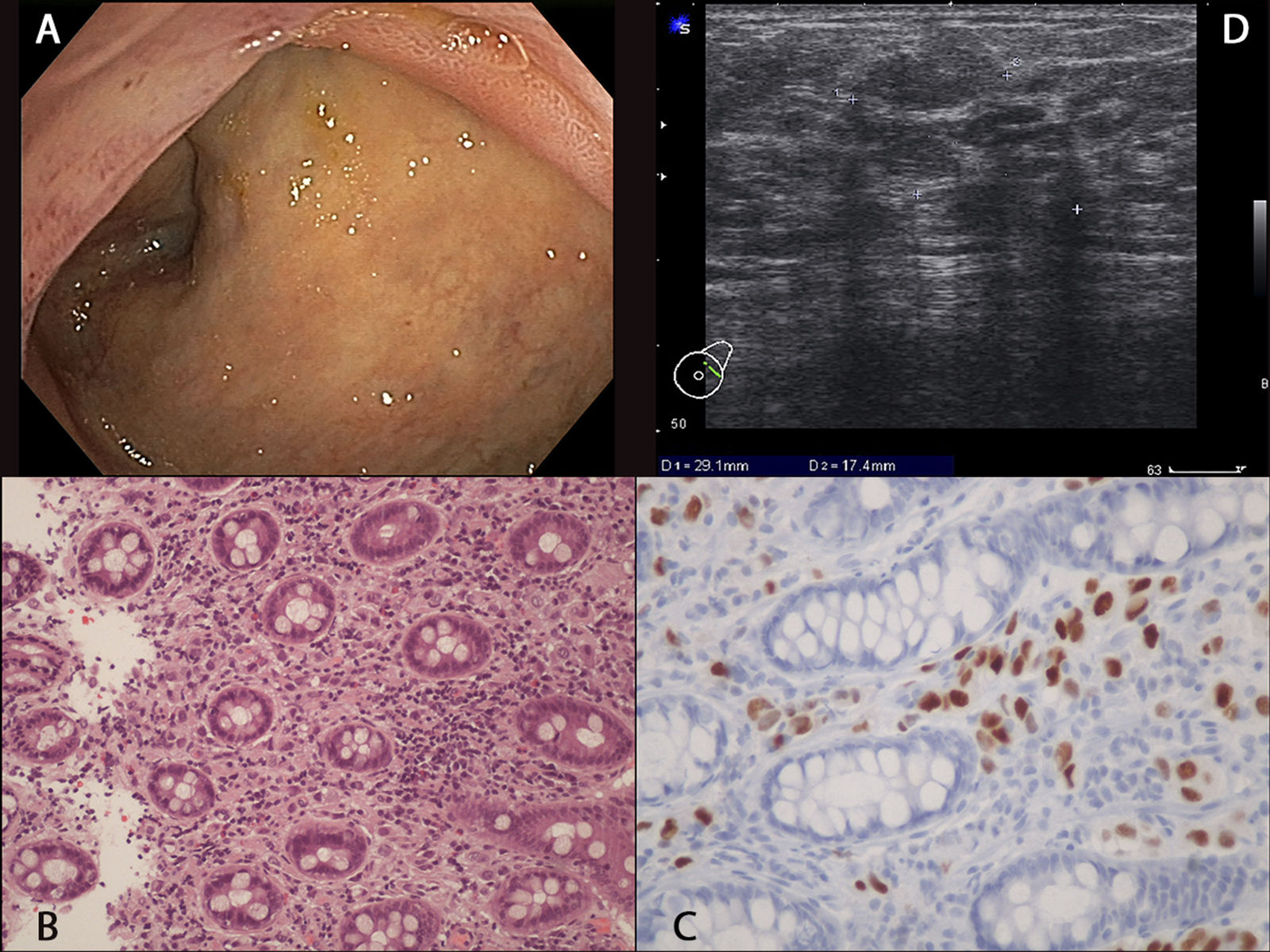
 Endoscopic image showing marked erythema of the ileocecal valve and eodema and loss of vascular pattern of the cecum mucosa. (B) Histopathology of biopsies from the ileocecal valve showing poorly cohesive tumor cells in lamina propria and signet ring cells, 200×. (C) Positive immunohistochemistry for estrogen receptor. (D) Breast ultrasound image showing a hypoechoic nodule with posterior acoustic shadowing.")
(A) Endoscopic image showing marked erythema of the ileocecal valve and eodema and loss of vascular pattern of the cecum mucosa. (B) Histopathology of biopsies from the ileocecal valve showing poorly cohesive tumor cells in lamina propria and signet ring cells, 200×. (C) Positive immunohistochemistry for estrogen receptor. (D) Breast ultrasound image showing a hypoechoic nodule with posterior acoustic shadowing.
The patient was sent to Ginecology clinic for examination and, in the upper outer quadrant of the left breast, it was palpable a hard, immovable, painless mass with irregular borders, associated with ipsilateral retracted nipple and axillary adenopathy. Breast ultrasound demonstrated a hypoechoic nodule with posterior acoustic shadowing, measuring 29mm×17mm (Fig. 1D). Histology of nodule biopsy confirmed invasive lobular carcinoma (estrogen receptor positive, progesterone receptor negative, Her2 negative, Ki-67 10%). Further staging imaging also revealed axillary lymph nodes and bone metastasis. The patient was proposed for palliative hormonal therapy.
Metastatic breast cancer is uncommon at the time of diagnosis,1 usually spreading to the bone, lung, liver and brain.3 Gastrointestinal metastasis from breast cancer are rare and usually associated with lobular histology.2 The most frequent site of metastasis on the gastrointestinal tract is the stomach, followed by the small bowel and the colon.2 Clinical manifestations are non-specific and include abdominal pain, bowel obstruction or inflammatory diarrhea.2 Endoscopic features include mucosal nodularity and rigidity, or lobulation and deformity caused by the presence of a mass. Therefore, diagnosis is challenging as metastasis may mimick inflammatory bowel disease or primary colon cancer.2 In conclusion, we report a rare case of bowel metastasis as the initial presentation of lobular breast carcinoma, that requires a high index of suspiction for the diagnosis from the pathologist and the gastroenterologist.
Conflicts of interestNo conflicts of interest to declare.

