

The aim of this study is to determine the hospital's efficiency as regards neoadjuvant chemotherapy for the resection of initially unresectable metastases for patients with metastatic primary colorectal cancer and to describe the chemotherapy used.
MethodsDescriptive, retrospective study of patients with colorectal cancer from 2004 to 2007. The percentage of resection for metastases following neoadjuvant chemotherapy administration was studied.
ResultsClinical histories of 118 patients diagnosed with metastatic colorectal cancer were reviewed. Metastases were initially resectable in ten patients (8.5%) and unresectable in the remaining 108 patients (91.5%). Following neoadjuvant chemotherapy, metastatic resection was performed on 19 patients.
ConclusionsNeoadjuvant chemotherapy played an important role in treating patients with disseminated metastatic colorectal cancer by reducing, in some cases, tumour size and treating initially unresectable metastases susceptible to subsequent surgical resection.
FOLFOX scheme was the most used neoadjuvant chemotherapy treatment.
El objetivo de este trabajo es determinar la efectividad en el hospital de la quimioterapia neoadyuvante en la resección de metástasis inicialmente irresecables, en pacientes con cáncer colorrectal diseminado y describir la quimioterapia utilizada en este contexto.
MétodoEstudio descriptivo, retrospectivo de los pacientes con cáncer colorrectal diseminado desde el año 2004 hasta el año 2007. Se estudió el porcentaje de pacientes diagnosticados de cáncer colorrectal diseminado cuyas metástasis fueron resecadas tras recibir tratamiento con quimioterapia.
ResultadosSe revisaron las historias clínicas de 118 pacientes diagnosticados de cáncer colorrectal metastásico. Las metástasis fueron resecables de inicio en 10 pacientes (8,5%) e irresecables en 108 (91,5%). Se administró quimioterapia neoadyuvante a 19 pacientes de los cuales 7 pudieron rescatarse quirúrgicamente.
ConclusionesLa quimioterapia neoadyuvante demostró tener un papel importante en el tratamiento de los pacientes con cáncer colorrectal diseminado, disminuyendo el tamaño de las metástasis y posibilitando, en algunos casos, la conversión de metástasis irresecables en metástasis resecables para su posterior resección quirúrgica.
El tratamiento más utilizado como quimioterapia neoadyuvante fue el esquema FOLFOX.
Colorectal cancer (CRC) has the highest incidence of any type of cancer in Spain (25600 cases per year).1 The incidence rate has increased among both sexes and all age groups in the last few decades.2
In terms of absolute mortality, CRC caused 7703 deaths in men and 5631 in women in 2006.1
The high mortality rate is explained by the fact that approximately 30%–40% of patients diagnosed with CRC suffer metastasis in the course of the disease,3,4 with 15%–20% of metastasis at the time of diagnosis. Metastases are most commonly found in the liver,4 followed by the lungs. Metastasis in both locations is present in 5%–10% of all patients.5
Resection is impossible for approximately 80% of liver metastases in patients with metastatic CRC (mCRC). The 5-year survival rate for patients with inoperable mCRC is less than 20%.6 When metastases can be surgically resected, the 5-year survival rate is 30%–40%.5,7,8 The only potential cure for disseminated mCRC is surgical resection of the metastases. Patients whose metastases are not initially operable have the possibility of undergoing a systemic treatment known as neoadjuvant chemotherapy (NAC) prior to surgery.4
Recently developed chemotherapy agents such as oxaliplatin and irinotecan make it possible to shrink tumours, increase survival rates in inoperable cases and increase the original 20% of patients able to undergo metastasectomy by 10%.4,8–10
Associating chemotherapy with the monoclonal antibodies bevacizumab and cetuximab leads to a 12%–20% increase in treatment response compared to chemotherapy alone.3
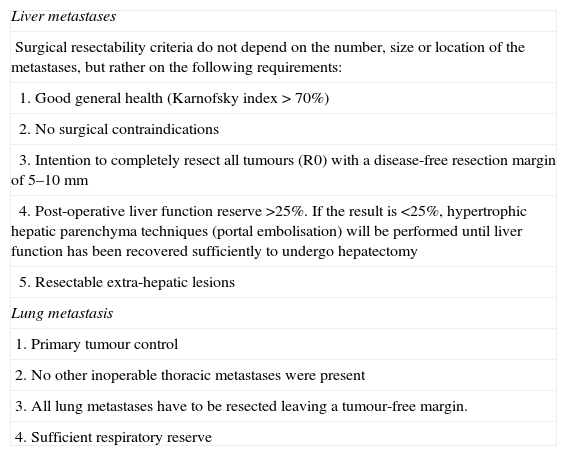
The definition of surgical resectability of liver metastases has changed over time as new chemotherapy agents have been introduced4 and new diagnostic and surgical techniques have been developed (Table 1).
Resectability Criteria (Summary Version).
| Liver metastases |
| Surgical resectability criteria do not depend on the number, size or location of the metastases, but rather on the following requirements: |
| 1. Good general health (Karnofsky index>70%) |
| 2. No surgical contraindications |
| 3. Intention to completely resect all tumours (R0) with a disease-free resection margin of 5–10mm |
| 4. Post-operative liver function reserve >25%. If the result is <25%, hypertrophic hepatic parenchyma techniques (portal embolisation) will be performed until liver function has been recovered sufficiently to undergo hepatectomy |
| 5. Resectable extra-hepatic lesions |
| Lung metastasis |
| 1. Primary tumour control |
| 2. No other inoperable thoracic metastases were present |
| 3. All lung metastases have to be resected leaving a tumour-free margin. |
| 4. Sufficient respiratory reserve |
The aim of this study was to determine in-hospital effectiveness of NAC in resecting initially inoperable metastases in patients with mCRC and describe chemotherapy used in this context.
MethodDescriptive retrospective study was done of CRC patients admitted between 2004 and 2007 to a 500-bed university hospital serving 250000 patients and located in an area with 700000 inhabitants.
Patients with mCRC were identified based on the intravenous chemotherapy records in the pharmacy service. We then proceeded to review the medical histories of all patients to identify those who had undergone NAC according to hospital protocol. Prescribing doctors recorded the purpose of the chemotherapy treatment (neoadjuvant, adjuvant or palliative) in the patients’ medical histories. We studied the group of patients diagnosed with mCRC whose liver or lung metastases had been resected surgically following treatment with NAC. Patient treatment and progress were monitored until February 2008.
According to the protocol, potentially resectable liver metastases are treated with 6–8 cycles of FOLFOX4 and the lesions are subsequently evaluated. Hepatectomy will be performed if the lesion becomes surgically correctable. If the lesion cannot be corrected, 6 or 8 cycles of FOLFIRI are administered and the liver lesions are evaluated once more. If they become surgically operable, hepatectomy will be performed. If they remain inoperable, each patient is evaluated on an individual basis.
Where lung metastases are present, we follow the same steps and use the same treatment as for liver metastases.
ResultsWe reviewed the clinical histories of 118 patients diagnosed with mCRC with a mean age of 65.66±12.8 years (35–84). Males accounted for 67% of the patients and the primary tumour location was the colon in 77%. Metastases were synchronous in 60% of the patients. Metachronous metastases (40%) broken down by the initial stage for the primary tumour are: 6% in stage I, 49% in stage II and 45% in stage III.
Metastases were initially resectable in 10 patients (8.5%) and inoperable in 108 patients (91.5%).
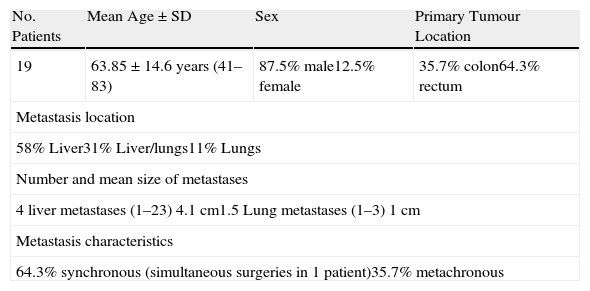
Of the 108 patients, 19 met the criteria for the hospital's NAC mCRC protocol in order to reduce tumour size and resect lesions surgically. The demographic characteristics of these 19 patients are shown in Table 2.
Demographic and Tumour Characteristics for Patients Eligible to Receive Neoadjuvant Chemotherapy.
| No. Patients | Mean Age±SD | Sex | Primary Tumour Location |
| 19 | 63.85±14.6 years (41–83) | 87.5% male12.5% female | 35.7% colon64.3% rectum |
| Metastasis location | |||
| 58% Liver31% Liver/lungs11% Lungs | |||
| Number and mean size of metastases | |||
| 4 liver metastases (1–23) 4.1cm1.5 Lung metastases (1–3) 1cm | |||
| Metastasis characteristics | |||
| 64.3% synchronous (simultaneous surgeries in 1 patient)35.7% metachronous | |||
The Karnofsky index was unavailable for half of the medical histories and ranged between 80% and 90% in the other half.
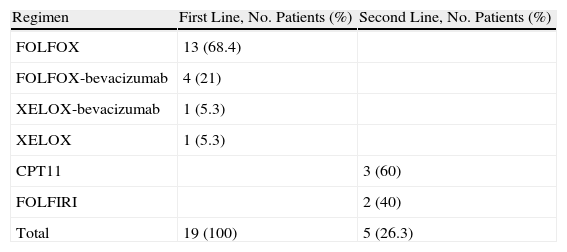
These 19 patients received first-line chemotherapy and 5 (26.3%) underwent second-line treatment as well, which was also neoadjuvant, due to disease progression.
The NAC regimens are shown in Table 3.
The mean number of cycles administered prior to rescue surgery was 7±2.2 (5–10).
Following administration of NAC, it was possible to perform rescue surgery on 7 patients (37%): liver metastases were resected in 3 patients (43%), both liver and lung metastases were resected in another 3 patients (43%), and lung metastases were resected in 1 patient (14%).
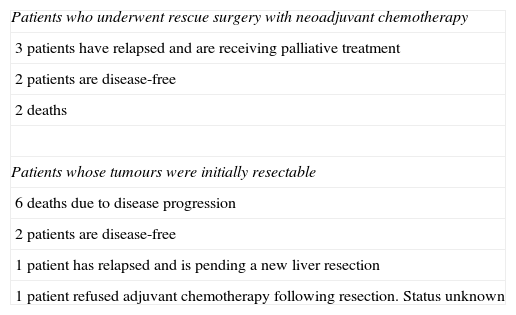
The progress of these 7 patients and the 10 initially operable patients can be seen in Table 4. No statistical analysis was performed for the two groups due to sample size being too small.
Patient Progress Following Resection of Metastases.a
| Patients who underwent rescue surgery with neoadjuvant chemotherapy |
| 3 patients have relapsed and are receiving palliative treatment |
| 2 patients are disease-free |
| 2 deaths |
| Patients whose tumours were initially resectable |
| 6 deaths due to disease progression |
| 2 patients are disease-free |
| 1 patient has relapsed and is pending a new liver resection |
| 1 patient refused adjuvant chemotherapy following resection. Status unknown |
Primary tumour location was different among patients receiving NAC. While 77% of the general population with mCRC had lesions in the colon, primary location was the rectum in 64.3% of our sample of 19 patients.
All patients received NAC with oxaliplatin regimens as recommended by hospital protocol. FOLFOX4 was the treatment administered to 68.4% of the patients.
The percentage of patients treated with the monoclonal antibody bevacizumab in addition to the oxaliplatin regimen was 26.3%. This percentage is low if we consider that associating chemotherapy with monoclonal antibodies results in an increase in treatment response,3 but bevacizumab was first commercialised in 2005 and included in the hospital's protocol in mid-2007. Since then, this combination has been administered to patients with potentially resectable mCRC as a first-line treatment, but it was not a common clinical practice during the data collection period.
Oxaliplatin combined with oral capecitabine (XELOX) and the FOLFOX regimen have been shown to be similarly effective, and both may be used interchangeably.11 The results show little use of the XELOX regimen, which eliminates the need to implant a port-a-cath for continuous 5-FU infusion. This can be explained by the same reason we provided regarding use of bevacizumab, namely that this regimen was introduced more recently.
Until now, it has not been proven that regimens with irinotecan are more effective than regimens with oxaliplatin and vice versa. Both types of regimens are considered equivalent choices for first-line treatment.12
The reason why the hospital used oxaliplatin-based regimens has to do with local choices, since both regimens are equally effective.12
Patients receiving capecitabine monotherapy may not have been identified due to the methodology employed in this study. This does not affect neoadjuvant treatments but it could have an effect on the global data for mCRC patients provided in the results, as certain patients, due to age and/or co-morbidities, may have been treated exclusively with oral capecitabine.
Second-line treatments were administered to patients whose disease progressed during NAC. They were also used as neoadjuvant treatments even if the metastases remained unresectable.
Following NAC administration, 37% of the patients were able to undergo rescue surgery.
Percentages of conversion to resectability vary among the different published studies, from 10% to 20%3–5,12,13 to as much as 40% in the study by Alberts et al.14 in patients with liver metastasis only.
Our study sample included 4 patients whose lung metastases were resected: 3 had lung and liver metastases, and 1 had lung metastases only.
The differences between the two studies may be due to variations in patient selection criteria, resectability criteria and the experience of the different surgical teams.
In conclusion, NAC plays an important role in treating patients with mCRC. It decreased the size of the lesions and in some cases, resulted in the conversion of inoperable to operable tumours that could then be resected. The most commonly used NAC was the FOLFOX regimen.
Conflict of InterestThe authors have no conflicts of interest to declare.
Please cite this article as: Redondo Capafons S, et al. Quimioterapia neoadyuvante en la resección de metástasis hepáticas y pulmonares de cáncer colorrectal. Farm Hosp. 2011;35:255.e1–e5.

