

To describe the use and effectiveness of linezolid as an alternative treatment for methicillin-resistant Staphylococcus aureus.
MethodDemographic, clinical and safety data were collected from hospitalised patients. The information sources were the clinical records and the pharmacy programme.
ResultsThirty patients were treated with linezolid (median age 69.3, 63% male). The median duration of treatment was 8 days. The most prevalent indication was soft tissues and skin infections (46.7%). The indications were off-label in 40% of cases. Linezolid was used as a targeted therapy in 53%, especially for coagulase-negative Staphylococcus. Clinical healing occurred in 83.3% and microbiological healing in 40%. Three patients (10%) experienced side effects from using linezolid.
ConclusionThe effectiveness and safety of linezolid is similar to that described in the trials. Its off-label use and the high number of empirical treatments mean that new strategies must be developed.
Linezolid supone una alternativa frente a Staphylococcus aureus resistente a meticilina. Describir la utilización y efectividad de linezolid.
MétodosSe recogieron datos demográficos, clínicos y de seguridad de los pacientes hospitalizados. Las fuentes de información fueron las historias clínicas y el programa de gestión de farmacia.
ResultadosTreinta pacientes recibieron tratamiento con linezolid (mediana de edad 69,5 años, 63% varones). La mediana de días con tratamiento fue de 8. La indicación más prevalente fue infección de piel y partes blandas (46,7%). En un 40%, las indicaciones no se ajustaban a las aprobadas por la agencia reguladora. Linezolid se utilizó como tratamiento dirigido (53%) mayoritariamente frente a Staphylococcus coagulasa-negativo. La curación clínica se obtuvo en el 83,3% de los casos, y curación microbiológica en el 40%. En 3 pacientes (10%) se describieron reacciones adversas asociadas al tratamiento.
ConclusiónLa efectividad y seguridad de linezolid es parecida a la descrita en los ensayos. Su uso fuera de indicación y el elevado número de tratamientos empíricos debe plantearnos el desarrollo de estrategias.
Linezolid is an oxazolidinone antibiotic. It acts on gram-positive and anaerobic microorganisms, although it is primarily known for its activity against meticillin-resistant Staphylococcus aureus (MRSA). Its oral formulation (100% bioavailability) enables use of sequential therapy.1–3
Linezolid was approved by the Agencia Española de Medicamentos y Productos Sanitarios (AEMPS, the Spanish drug and medical product agency) in July 2001 and modified on April 2007, for the following1:
- -
Hospital-acquired pneumonia and community-acquired pneumonia, either proven or suspected to have been caused by linezolid-sensitive gram-positive bacteria.
- -
Complex skin and soft tissue infections only in cases in which microbial testing shows that the infection is caused by linezolid-sensitive gram-positive bacteria.
On 26 April 2007, the AEMPS issued a statement warning of the increase in mortality among patients treated with linezolid and the possibility of mixed infections or infection with gram-negative bacteria. This statement resulted in changes to its summary of characteristics.4
Drug use studies are descriptive studies intended to examine to what extent knowledge acquired through clinical trials can be applied to daily practice. They also constitute a sort of treatment audit allowing us to improve the quality of clinical practice.5,6
This study will describe the effectiveness, safety, and usage of linezolid in a secondary care hospital in Andalusia (600 beds, 490 with single-dose dispensing), following the modifications made to its summary of characteristics. The study was approved by the hospital's Ethics Committee.
MethodPopulationRetrospective descriptive study. The target population was 100% of patients admitted during 2008. The inclusion criteria stipulated patients ≥14 years admitted to inpatient wards and who received at least 1 dose of linezolid. We excluded patients admitted to the intensive care unit (ICU) and the gynaecology and paediatrics wards. Our information sources included patients’ medical histories and the single-dose management programme (MultiBase-TransTOOLs, version 4.3, rev. 7.08).
VariablesRecorded demographic data were age, sex, the patient's unit and the prescribing department; clinical data were the indication, empirical or rational therapy, clinical healing (resolution of the signs and symptoms of infection at the end of treatment), microbiological healing (cultures negative at the end of treatment), and treatment duration; safety data were adverse drug reaction (ADR) and death rates.
StatisticsQualitative data were analysed descriptively using frequencies and quantitative data were analysed using central tendency and dispersion measures (median and range). SPSS 12.0 statistical software was used for all analyses.
ResultsIn 2008, 16399 patients were admitted of which 0.18% were treated with linezolid. In total, 36 patients received linezolid in an inpatient ward; only 30 patients had a recoverable medical history and met the minimum conditions for patient evaluation (complete histories of both the episode and administration of the drug).
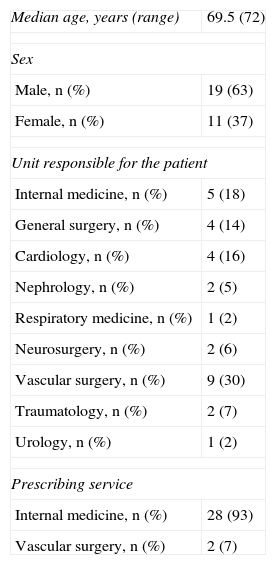
The patients’ median age, sex, assigned ward and prescribing department appears in Table 1.
Characteristics of Our Population.
| Median age, years (range) | 69.5 (72) |
| Sex | |
| Male, n (%) | 19 (63) |
| Female, n (%) | 11 (37) |
| Unit responsible for the patient | |
| Internal medicine, n (%) | 5 (18) |
| General surgery, n (%) | 4 (14) |
| Cardiology, n (%) | 4 (16) |
| Nephrology, n (%) | 2 (5) |
| Respiratory medicine, n (%) | 1 (2) |
| Neurosurgery, n (%) | 2 (6) |
| Vascular surgery, n (%) | 9 (30) |
| Traumatology, n (%) | 2 (7) |
| Urology, n (%) | 1 (2) |
| Prescribing service | |
| Internal medicine, n (%) | 28 (93) |
| Vascular surgery, n (%) | 2 (7) |
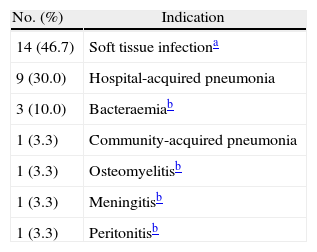
The most prevalent indication was skin and soft tissue infection (SSTI) with a total of 14 (46.7%) cases (Table 2); 5 of these were infected surgical wounds. The second most prevalent indication was hospital-acquired pneumonia with 9 cases (30.0%).
In 12 patients (40%), the indication was off-label with respect to uses approved by the AEMPS. Of these patients, 6 suffered soft-tissue infections that were treated empirically. Doctors chose linezolid treatment for 2 patients with kidney failure and 1 patient with a vancomycin allergy.
The hospital began 14 empirical treatments and 16 rational treatments. Treatment was adapted in 5 of the patients receiving empirical treatments according to the antibiogram; another 5 in this group began linezolid treatment due to treatment failure (4 patients had treatment that did not cover MRSA and 1 was on vancomycin). Of the 16 patients who received rational treatment, 15 had multiresistant microorganisms: 8 (50%) had coagulase-negative Staphylococcus; 3 (18.7%) had MRSA; 2 (12.5%) had Enterococcus faecium; 2 (12.5%) had Enterococcus faecalis. All microorganisms were sensitive to vancomycin (MIC≤1), cotrimoxazole, clindamycin or teicoplanin. Treatment with linezolid was started in 3 patients due to vancomycin treatment failure. MRSA was only isolated in 1 patient with hospital-acquired pneumonia; in this patient, vancomycin was replaced with linezolid.
The median number of days of treatment was 8 (range 29). Only one patient was treated for a period longer than 28 days (30 days).
The episode healed clinically in 25 patients (83.3%). Microbiological healing was only demonstrated in 12 patients (40% of the patient total). For the rest of the patients, we have no information regarding negative cultures after treatment, either due to the patient recovering clinically and being discharged without further testing, or due to death.
ADRs were described in 3 patients (10%). There was one case of thrombocytopenia, classified as conditional under a modified Karch-Lasagna algorithm, which led to discontinuing linezolid treatment. There was also a case of pain during intravenous linezolid administration, classified as “probable” by the algorithm, which led to discontinuing treatment. In addition, one case of candidiasis classified as “probable” resolved without affecting the treatment duration or the patient's state. The detected ADRs were reported to the Andalusian pharmacology centre. During the course of the infection, 5 patients died (16.7%).
DiscussionThe initial increase in multiresistant hospital microbial flora,7,8 in addition to the meagre effect of traditional antibiotics on these organisms in certain cases (the controversial use of vancomycin in intermediate-sensitivity MRSA infections9,10) mean that new antibacterial agents may be admitted to the list of conventional treatments. It is therefore important to make rational use of new treatment alternatives so that they do not lose efficacy in the near future.
Our study aims to present the current panorama for this antibiotic, with a view to detecting possible cases of irregular use and employ antimicrobial treatment in a more rational manner.
The most common indication for linezolid is SSTI, and most of these patients are treated by the vascular surgery department. It would be reasonable to think that many of these infections have to do with diabetic foot infections (these data were not recorded on our data sheet).
In studies completed by Ziglam et al.15 and Walker et al.16 on linezolid, some data differ from our current data. In both studies, soft tissue infection was the most frequent indication (26% and 32%), as in our study. However, the isolated microorganisms were different; in both cases, the most prevalent was MRSA (55% and 44.7%). Our median number of 8 treatment days (range=29) is substantially lower than that reported in these studies (14.4 and 22 days). In our study, adherence to the approved indications listed on the drug's summary of characteristics (40%) is more comparable to the Walker et al. study (53%) than to the Ziglam et al. study (which only indicates that adherence to recommended indications was very good). We should point out that in the articles cited above, “adherence” means compliance with a series of in-house recommendations designed by hospital experts. This is normally done by a multidisciplinary team (and infectious disease specialist, an infectious disease pharmacist, microbiologist, preventive medicine specialist, etc.). The only recommendations used in our hospital are those found on the summary of characteristics; we do not have an antibiotics use monitoring programme. The rate of off-label use (in 40% of the patients), and the fact that nearly 50% of the treatments were empirical, mean that we should re-examine its use in the hospital. Most of the patients were monitored by the internal medicine department.
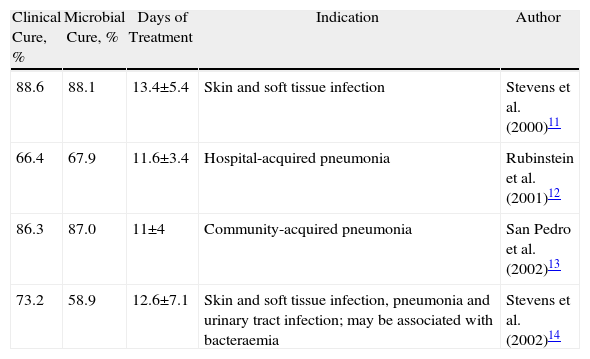
Table 3 shows the results with regard to clinical cure, microbial cure, and treatment duration that were gathered from different trials that supported the use of linezolid for the different indications. The studies may not be compared to one another because they contain different populations and were not designed for that purpose, but they do serve as a reference. We must point out that our study does not differentiate between the different illnesses, since the patient number for each disease was not high enough to establish a comparison. In our study, the effectiveness of linezolid is similar to that described in clinical trials. Obviously, given the lack of a control group, these data must be used with caution and provide only approximate information that should not be used in decision-making processes.
Studies Cited for Approving Different Indications.
| Clinical Cure, % | Microbial Cure, % | Days of Treatment | Indication | Author |
| 88.6 | 88.1 | 13.4±5.4 | Skin and soft tissue infection | Stevens et al. (2000)11 |
| 66.4 | 67.9 | 11.6±3.4 | Hospital-acquired pneumonia | Rubinstein et al. (2001)12 |
| 86.3 | 87.0 | 11±4 | Community-acquired pneumonia | San Pedro et al. (2002)13 |
| 73.2 | 58.9 | 12.6±7.1 | Skin and soft tissue infection, pneumonia and urinary tract infection; may be associated with bacteraemia | Stevens et al. (2002)14 |
The ADRs we detected are fully described in the literature and on the summary of characteristics.
Our study has the typical limitations found for descriptive, retrospective studies based on reviewing medical histories. Our population is quite limited, especially as we have selected only those patients who were admitted to the inpatient ward. Patients from the ICU were excluded, although this unit uses a large quantity of linezolid (15% of the hospital total).
Closer cooperation between the internal medicine and pharmacy departments should result in better management of the drug. While linezolid use is not excessive at our hospital, and we do not have high levels of multiresistant microorganisms, it may be useful to implement a posteriori control policies, for use after initial prescription of the drug, or list it as a restricted-use drug. The increase in MRSA, including linezolid-resistant strains,17,18 the high cost of the drug (€114.70/day of treatment) and the limited number of available antibiotics should convince us that the drug should only be used for well-documented infections (SSTI and HAP) and when alternative treatments may not be used (due to allergy or glycopeptides being contraindicated).
Conflict of InterestThe authors have no conflict of interest to declare.
Please cite this article as: Rivas R, et al. Efectividad y uso del linezolid en planta de hospitalización. Farm Hosp. 2011;35:322–5.

