



COVID-19 pandemic has affected the mental health system (MHS) globally, although significant geographical variation was found, particularly for depression and anxiety. The understanding of its impact at the regional level of the context of care is limited when compared to national evaluations.
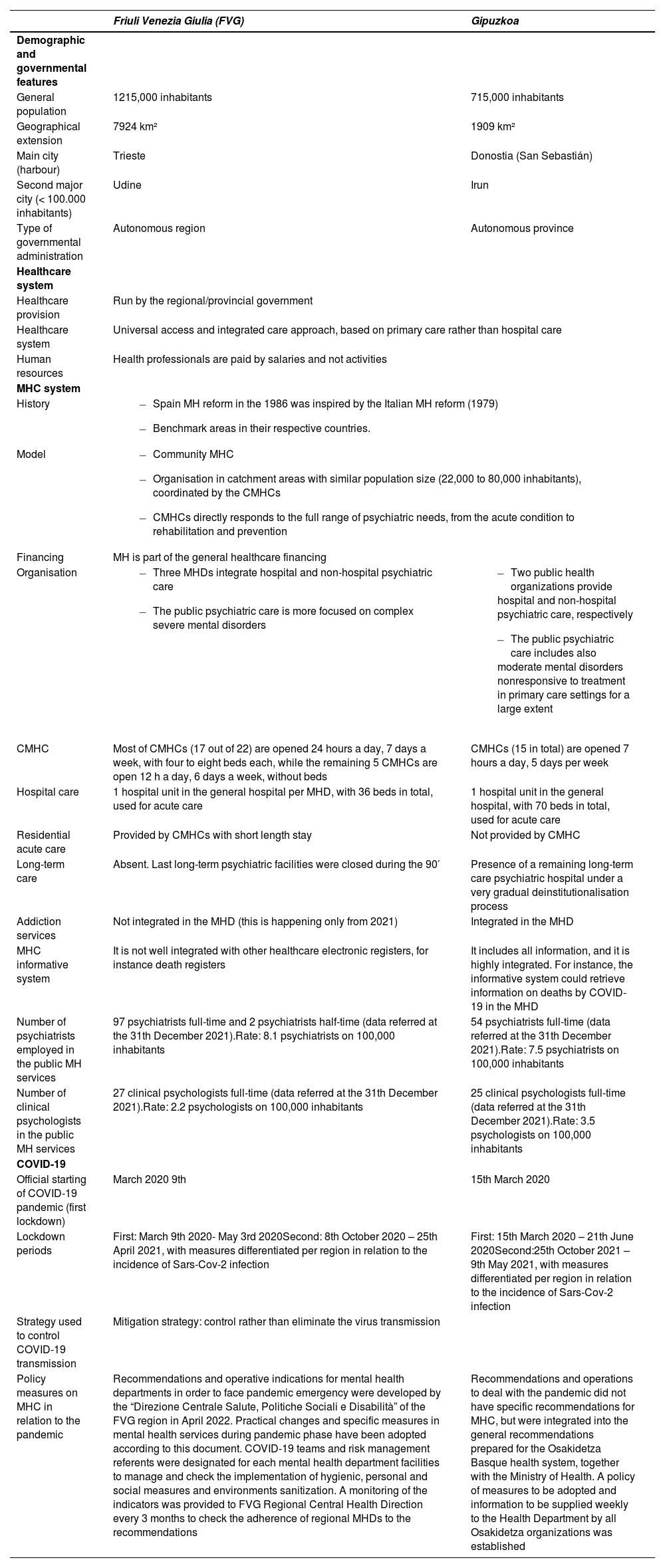
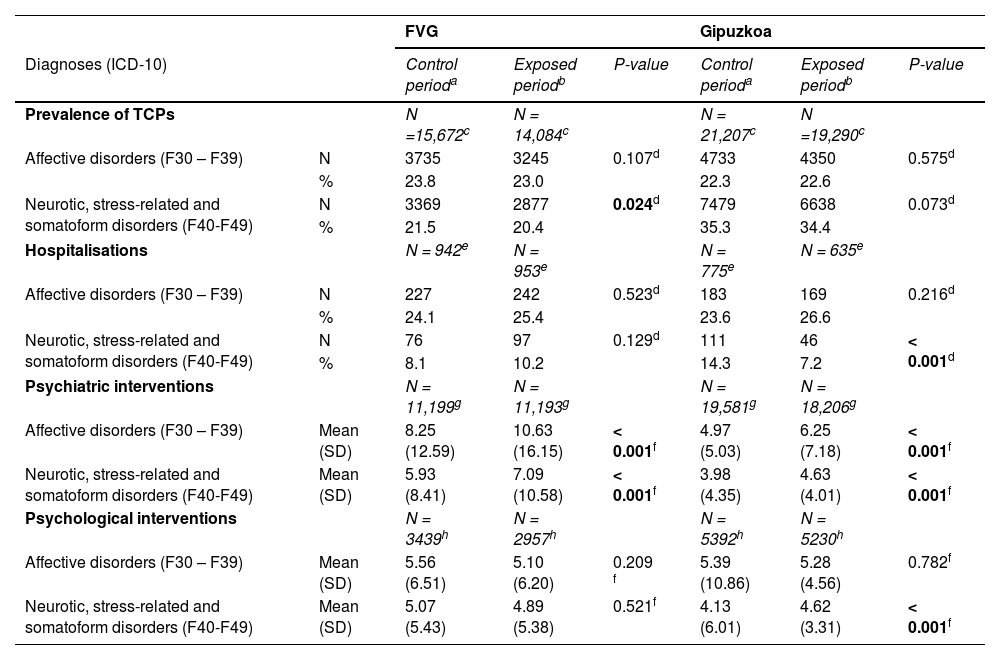
MethodsCollective case study comparing the prior pattern of care with the first 11 months of COVID-19 in two sites: Gipuzkoa (Spain) and Friuli Venezia Giulia - FVG (Italy). Information from both sites derive from administrative data of MHS in the two regions harmonized for comparison. Data included prevalence of psychiatric diagnoses (ICD-10 F30-F39 and F40-F49 codes), number of hospitalisations, mean and range of psychiatric and psychological interventions. Significance of time-period and location difference was assessed using the Chi-square and the T-statistics for prevalence and count data, respectively.
ResultsMHS is community-based in both sites. The prevalence of anxiety decreased in FVG, while a decrease in hospitalisations was found in Gipuzkoa. Both sites registered an increase in psychiatric visits for anxiety and depression. In both periods, FVG showed significant lower prevalence of diagnoses, but higher mean number of psychiatric interventions.
Conclusions: The COVID-19 outbreak is a paradigmatic example of complex dynamic systems in public health and illustrates the importance of considering its local context and time dependency. The Standard mapping and coding of local MHS provision is essential to allow comparison and reduce ambiguity. This study highlights the importance of ecosystem research to better interpret epidemiological data and support the development of evidence-informed policymaking.