




This review aims to analyze the studies on cleaning practices and the efficiency of the cleaning carried out in environments that have a great risk of resistant microorganism infection, such as intensive care units.
MethodsIn this study, a retrospective literature review was undertaken of the relevant publications between the years 2005 and 2020, using the keywords “Cross Infection, Infection Control, Multidrug-Resistant Bacteria, Intensive Care, Room Cleaning, Environmental Cleaning, Hospital-Associated Infection”; using the international databases Pubmed, CINAHL and EBSCO and domestic database ULAKBIM on search engines. Titles and abstracts of all relevant articles found on electronic searches were reviewed by the researchers independently. The Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols guideline and Patient, Intervention, Comparison, Outcomes, Study design model were used in analysing the studies.
ResultsThe selected studies were reviewed in four main categories: Materials used in cleaning, the period between taking environmental samples, cleaning methods, and the efficiency of cleaning. Among the studies included herein, eight were randomized controlled trials, three were retrospective intervention studies, two were case-control studies and one was a retrospective cohort study.
ConclusionsToday, the assessment of cleaning in environments can be evaluated by different methods, but there are advantages and disadvantages of these methods. Therefore, in the relevant literature, it is suggested that cleaning must be evaluated by several methods, not only one. Also, training the staff that carries out the cleaning and rewarding correct behavior by giving feedback are important approaches to increase the efficiency of cleaning. It is suggested that cleaning must be carried out every day, regularly with effective methods and equipment; frequency of cleaning during epidemics must be increased, institutions must prepare cleaning manuals according to evidence-based guidelines that are recognized at an international level.
El objetivo de esta revisión es analizar los estudios sobre la práctica y la eficacia de la limpieza realizada en entornos con alto riesgo de infección por microorganismos resistentes, tales como las unidades de cuidados intensivos.
MétodosEn este estudio se realizó una revisión retrospectiva de la literatura dentro de las publicaciones relacionadas entre los años 2005 y 2020, utilizando palabras clave tales como cross infection, infection control, multidrug-resistant bacteria, intensive care, room cleaning, environmental cleaning, hospital-associated infection (infección cruzada, control de infecciones, bacterias multirresistenes a los fármacos, cuidados intensivos, limpieza de habitaciones, limpieza ambiental, infección adquirida en los hospitales), utilizando bases de datos internacionales tales como Pubmed, CINAHL y EBSCO, y la base de datos nacional ULAKBIM en los motores de búsqueda. Los títulos y resúmenes de todos los artículos relacionados seleccionados en las búsquedas electrónicas fueron revisados por investigadores de manera independiente. Se utilizaron las directrices de The Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols y el modelo del diseño Patient, Intervention, Comparison, Outcomes, Study para analizar los estudios.
ResultadosSe revisaron los estudios seleccionados en 4 categorías principales: materiales utilizados en la limpieza, periodo transcurrido entre las tomas de muestras ambientales, métodos de limpieza y eficacia de la limpieza. Entre los estudios incluidos en la revisión 8 eran ensayos controlados aleatorizados, 3 eran estudios retrospectivos de intervención, 2 eran estudios de control de casos y uno era un estudio retrospectivo de cohorte.
ConclusionesHoy en día la evaluación de la limpieza en los entornos puede evaluarse mediante métodos diferentes, aunque existen dichos métodos tienen ventajas y desventajas. Por tanto, en la literatura relevante se sugiere que la limpieza debe ser evaluada por diversos métodos, y no solo por uno. De igual modo, formar al personal a cargo de la limpieza y apreciar el comportamiento correcto mediante la aportación de comentarios son metodologías importantes para incrementar la eficacia de la limpieza. Se sugiere que la limpieza debe llevarse a cabo cada día, de manera regular, y con métodos y equipos efectivos. Debe incrementarse la frecuencia de la limpieza durante las pandemias, quedando a cargo de las instituciones el deber de preparar manuales de limpieza acordes a las directrices basadas en la evidencia a nivel internacional.
When vital functions of the patients are damaged in a way that carries risk, they must be treated in Intensive Care Units (ICU) to maintain vital functions and practice appropriate treatment methods.1 Patients admitted to ICU have a high risk of getting a nosocomial infection, partly because of their serious diseases, and partly because they were subject to life-saving invasive procedures.2 Nosocomial infection is a common morbidity and mortality reason among the patients.3 Due to high number of patients and the use of medical equipment that requires constant cleaning for patient care, the hospitals become a reservoir of possible pathogens.4,5 This kind of infection is related to longer time in ICU, a higher rate of mortality, and higher hospital costs.6 The environment plays a vital role in the transition of hospital-associated pathogens, and therefore, the pathogenesis of hospital-associated infection. The infection developed in ICU mostly stems from Multi-Drug Resistant Bacteria (MDRO).7 This bacterium can survive for hours or days, and in some cases, even months, including the dry environment. Bacteria that survive on surfaces may contaminate medical devices via the staff's hands.8 Pathogens existent in the environment may infect the patients.5 Transmission of pathogens from the environment to patients occurs via direct and indirect contact with contaminated surfaces.9 They transmit the pathogens by touching the patients. Therefore, the quality of the environment's sanitation is critical.9,10 Also, it is crucial to assess the clean-up to prevent hospital-associated pathogens and to control hospital-associated diseases.11 It is not enough for the environment to be clean visually.12 A microbiologically sanitized environment is essential. Improvement in existing hospital cleaning techniques may result in decreasing in hospital-associated pathogen development and therefore decreasing hospital-associated infections.13–15
As the number and rate of patients with an immune-deficiency increase, environmental risks become more problematical, and the evaluation of settings becomes more critical. The cleaning and disinfection strategy of environmental surfaces depends on the surface to be cleaned and may vary from basic water and soap cleaning to low-level disinfection.16 A lot of studies suggest that it is crucial to change environmental disinfection procedures in line with the characteristics of the environment to control epidemics.16,17 Today, to limit the transmission of infections associated with ICU and limit the morbidity and mortality associated with these infections, strategies to prevent transmission of MDRO have gained significance. In this sense, the cleaning must be done and evaluated in the most efficient way to prevent and control infections in hospital settings.13
ICU beds are a limited number of beds that need to be used effectively. The acute need for ICU beds reminds us of the importance of safely cleaning these beds and opening them to use in a short time. In environments with high risk of MDRO infection, such as intensive care units, effective cleaning will provide easy access to information on materials and methods used in cleaning, thus contributing to the application. We also think that cleaning the units effectively can contribute to improving patient safety by reducing hospital-related infection rates.
Which interventions give faster and more effective results among the studies investigating the cleaning interventions applied to patient unit with MDRO infection? This systematic review sought to answer the that question:
This review aims to analyze the studies about cleaning practices and the effectiveness of the cleaning carried out in environments that have a high risk of resistant microorganism infection, such as ICUs.
MethodologyThe systematic review was designed according to the Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) checklist.18
Screening strategyThe studies included here were screened according to the following criteria [Patient, Intervention, Comparison, Results, Study Design (PICOS) model].
- •
Study group (P): Health care-associate infections with MDRO
- •
Response (I): Cleaning the areas with MDRO infection
- •
Comparison (C): Interventions for effective cleaning
- •
Results (O): Health care-associate infections rates
- •
Study design (S): Randomized controlled trials, experimental and quasi-experimental trials, controlled clinical trials and case control studies
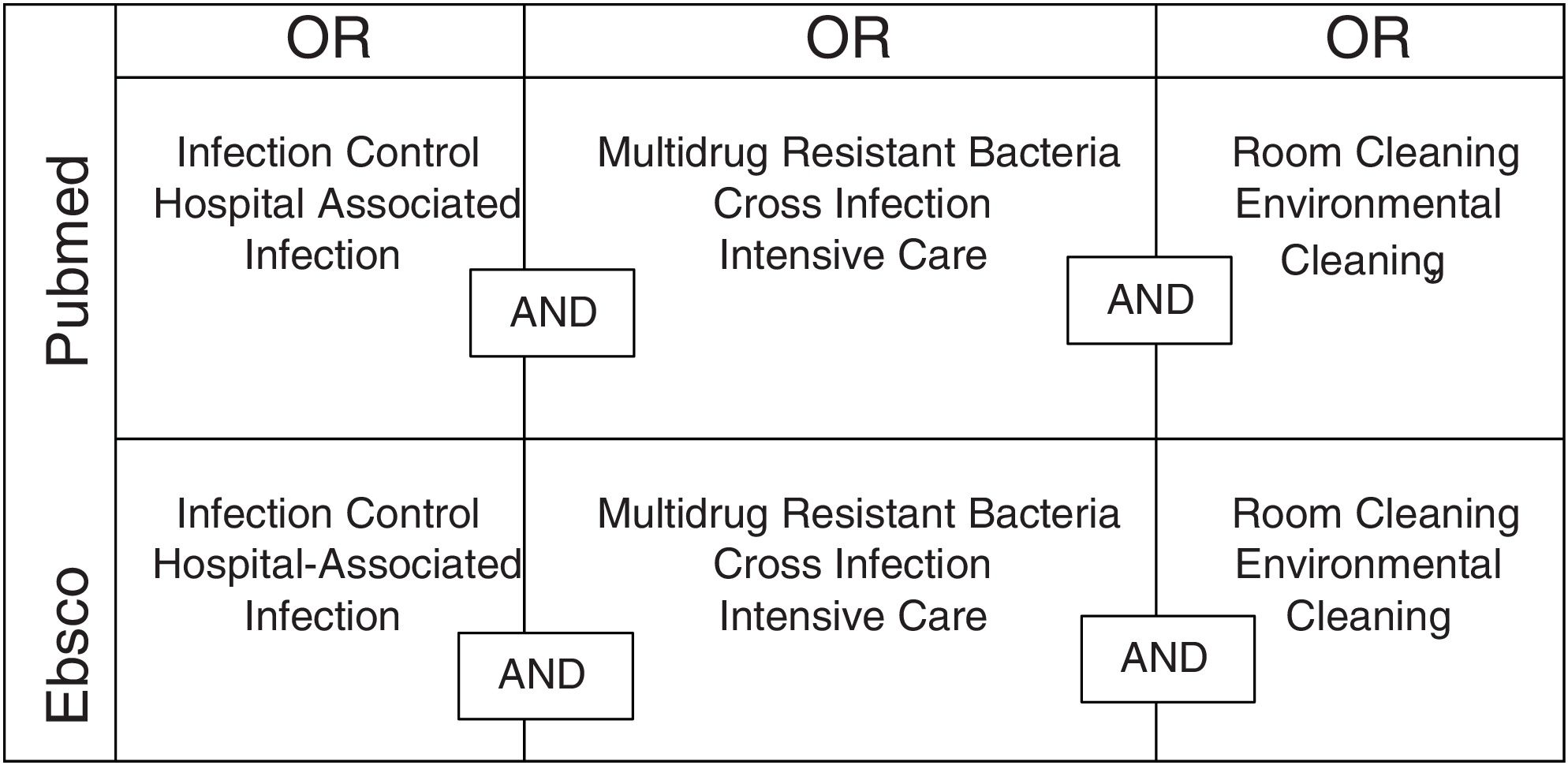
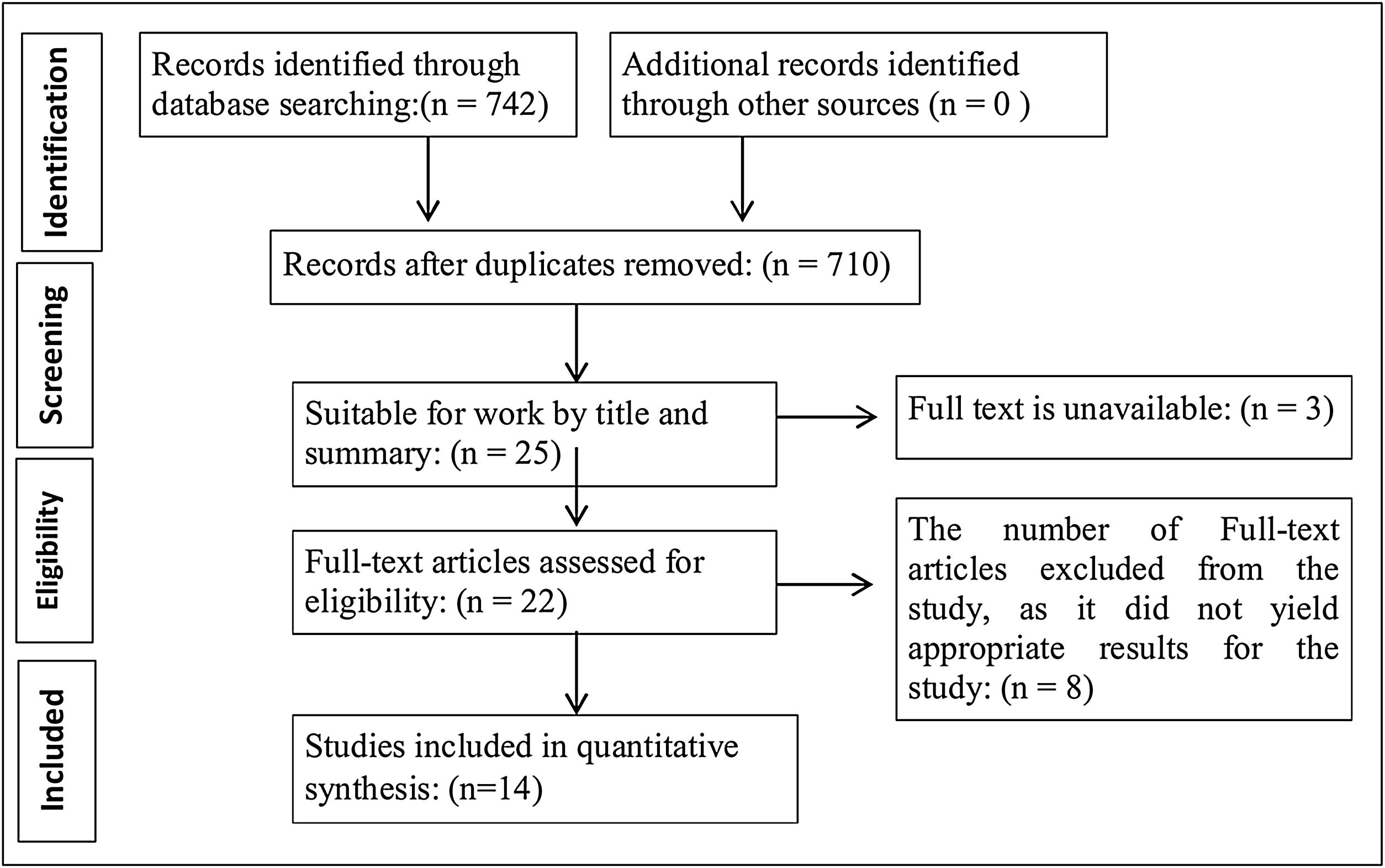
In this study, a retrospective literature review was made within the concerned publications between the years 2005 and 2020, using the keywords such as “Cross Infection, Infection Control, Multidrug Resistant Bacteria, Intensive Care, Room Cleaning, Environmental Cleaning, Hospital-Associated Infection”; using international databases Pubmed, EBSCO, CINAHL and domestic database ULAKBIM on search engines. The searching strategy was created by Boolean Operators OR and is shown in Fig. 1. Postgraduate theses in the electronic environment, nursing journals and medical journals were examined. Randomized controlled studies, experimental and quasi-experimental studies, controlled clinical studies, cohort studies and control cases were determined among the studies. The titles and abstracts of all the determined relevant articles were reviewed independently by the researchers. In cases where the title or the abstract were unclear, the full text was reviewed to determine whether the study was relevant. The studies obtained as a result of the screenings made by two independent, blind researchers were reviewed separately by the authors in terms of inclusion criteria, and a consensus was achieved. Reasons for exclusion were noted by the researchers (Fig. 2). After being reviewed by researchers, 728 sources of the 742 studies included were eliminated, considering the criteria and full texts of studies. 14 were chosen for systematical review. Language limitations were not applied for article determination.
Inclusion criteria for the study

Studies evaluating the effectiveness of cleaning carried out in critical sections of the hospital, studies published in the last fifteen years, the accessible full text of the studies, studies evaluating the effectiveness of cleaning with at least one of Adenosine Triphosphate (ATP), microbiological examination, ultraviolet (UV) fluorescent marker and visual inspection methods were taken into the examination. The language limitations were not applied for article determination.
Exclusion criteria for the studyStudies carried out in non-clinical areas with beds such as laboratory, polyclinic and operating room, cleaning studies other than MDRO and Vancomycin Resistance Enterococcus (VRE) infections, studies whose full texts are not available, studies that do not evaluate the effectiveness of cleaning have not been examined.
Data analysisA standard data summarizing form was developed, and data were evaluated according to it.
Data summarizing form contains; Authors, year, and country, aim of the study, sampling method, cleaning evaluation method, results of the study
Evaluation of methodological qualityStudies included herein were evaluated using the quality evaluation lists prepared by the Joanna Briggs Institute (JBI) according to research design.19 The control checklists consisted of 13 questions for randomized controlled studies, nine for quasi-experimental research, eight for cross-sectional research, and 10 for case–control studies. Each question in these lists can be answered by “Yes, No, Unclear, and Not Applicable.” (Table 1). GRADE was used to evaluate the evidence of the studies. In addition, the selected studies have been organized in Table 1 according to the year of publication.
Characteristics of the selected studies in the literature review.
| Author, year, country | Methodology | Objective | Sample | Data control method | Results | Bias risk score |
|---|---|---|---|---|---|---|
| White et al. 2007United Kingdom | Non-randomized controlled study | To evaluate the effectiveness of four different cleanup methods in the hospital | This study evaluated four hospital cleaning methods: ‘mop and vacuum’, ‘spray clean’ and ‘wet scrub’ for floors, and one steam cleaning method. Samples were taken from the same ten spots before and 1h after the cleanup. (Detergent and cotton cloth used) | A standardized microbiological screening method was used to sample the environment before and after cleaning to quantify total viable counts as well as identify specific organisms. | Results indicate that all surface cleaning methods reduced the total microbial load. Spray clean shows better results compared to traditional mopping and vacuuming. Steam cleaning for curtain also reduced microbial load. But it is less effective on Staphylococcus aureus (S. aureus) and other potential pathogens. These results may help administrators evaluate the costs of different cleanup methods that will improve to control the potential infection in a hospital | Yes 7/9No 2/9Unclear 0/9Not Applicable 0/9Low Risk |
| Hardy et al. 2007United Kingdom | Prospective studyCross sectional studiesTraining applied | This study aims to evaluate the rate of bacterial recontamination in ICU and the effect on the development of infection after the use of HPV | The study took place in an open-plan nine-bed capacity ICU without isolation rooms in five months. Environmental scanning was carried out monthly, three months before; weekly, four weeks before the use of HPV. All the patients were evacuated from the ICU before using HPV, and cleanup was carried out using the protocols, including washing all the walls in the ICU and thorough clean up. | Microbiological method | As a result, HPV is an effective way to eliminate bacteria from the environment. But it may not be effective means of recontamination of the unit rapidly and in cases when admitting infected patients to the unit after clean up. It is a proper cleaning method during epidemics to eliminate nosocomial bacteria if no reinfected or colonized patients will be admitted to the processed unit after the cleanup | Yes 4/8No 2/8Unclear 2/8Not Applicable 0/8Unclear Risk |
| Dancer et al. 2008United Kingdom | Cross sectional studiesTraining applied | This study aimed to investigate the microbiological cleaning of two hospital services in a consecutive 6-month period by comparing the presence of resistant micro-organisms. It also aimed to examine the relationships between microbial dirt levels and bed occupancy rates in hand-contact areas. | Ten hand-touch sites were screened weekly on two surgical wards over two consecutive six-month periods. | Dipslides were used for microbiological sampling, and visual assessment was used for environment screening | This study shows that there is a direct relationship between bed occupancy rates and high levels of microbial contamination of hand- touch surfaces. This study presents more evidence supporting the importance of environmental cleanliness to control MSSA and MRSA | Yes 6/8No 2/8Unclear 0/8Not Applicable 0/8Low Risk |
| Al-Hamad And Maxwell 2008United Kingdom | Prospective studyCross sectional studiesTraining applied | This study aimed to assess the effectiveness of cleaning/disinfection in critical care units to detect an indicator organism and dip-slides to quantitatively determine the microbial load. | Samples were collected from possible high contact environments such as the patient environment and common fields away from the patients in two different units. | Micro-Biological sampling was conducted using the wipe-rinse method and the dip slide method. | There is no direct relationship between two sampling methods in means of aerobic count results. In addition to this, it is recommended to combine two methods to evaluate the cleanup/disinfection and the changes made to clean up methods (such as agent used), more efficiently | Yes 6/8No 2/8Unclear 0/8Not Applicable 0/8Low Risk |
| Young et al. 2009Korea | Case–control studiesTraining applied | This study aimed to describe a vancomycin-resistant enterococci (VRE) outbreak across three intensive care units (ICUs) of a Korean hospital from September 2006 to January 2007 | Environmental surveillance cultures for VRE were performed three times (July, September and October 2006) before and after implementation of the extensive cleaning practices for environmental surfaces in the ICUs. | Environmental sampling cultures, antibiotic restrictions, and education of hospital staff were aspects of the study | The study defined the VRE outbreak across three ICUs at the molecular level and potential factors associated with VRE transmission. It further suggests that an aggressive multifaceted control strategy might be a rapid and effective approach for controlling the VRE outbreak in non-endemic hospitals | Yes 9/10No 1/10Unclear 0/10Not Applicable 0/10Low Risk |
| Choi et al. 2010Korea | Case–control studiesTraining applied | An increased number of infections or colonizations due to CRAB strains was noted in a hospital in Korea. In this study, it is aimed to conduct the control program that proved successful in reducing the CRAB outbreak spread of CRAB in two ICUs | All patients infected or colonized with CRAB were included in the study during the epidemic. A total of 135 swab samples were taken from the environment of patients infected or colonized with CRAB. The hands of health care workers, including doctors, nurses, and nursing aides, were also sampled to assess the potential of hand carriage, given the multiple contacts with ventilators and other patient-care items | Microbiological method; species identification and antibiotic susceptibility testing was conducted using a MicroScan automated instrument. Epidemic prevention strategies were also used (isolation preventions, hand hygiene practices, environmental cleanup, closed suctioning system). | Contamination was reduced after the use of epidemic prevention methods. Since August 2008, no CRAB colonization or infection case was seen. | Yes 8/10No 2/10Unclear 0/10Not Applicable 0/10Low Risk |
| Hall et al. 2011United Kingdom | Cross sectional studiesTraining applied | This study compared the relative ability of ultramicrofibre cloths and mops (UMF) moistened with either water or copper biocide (UMF+CuWB50; 300ppm) to remove bacteria from several environents in comparison to standard cleaning with cotton cloths | Samples were collected from designated surfaces on four different units before and right after the cleaning for microbiological screening and Adenosine Trifosfat (ATP). | Microbiological samples were collected three times a week 1h before the cleanup and 1h after it from designated surfaces. Sampling via ATP was conducted every day before and after the cleanup. | When standard clean up with hypocrite and cleanup using moistened CuWB50 UMF were compared, it was concluded that CuWB50+UMF showed more efficient cleanup performance | Yes 7/8No 1/8Unclear 0/8Not Applicable 0/8Low Risk |
| Knape et al. 2015Sweden | Prospective studyCross sectional studiesTraining appliedFeedback provided | This study was conducted to examine whether the amount of biological load, as measured by ATP on frequently touched near-patient surfaces, had been reduced after an intervention; to evaluate the relationship between visual assessment and ATP levels; to identify the ATP method as a tool in evaluating hospital cleanliness. | A prospective intervention study in three phases was carried out in a medical ward and an intensive care unit (ICU) at a regional hospital. Existing cleaning procedures were defined, and baseline tests were sampled by visual inspection and ATP measurements of frequently touched surfaces in patients’ rooms before and after the intervention. Nursing staff was educated about the importance of hospital cleaning and direct feedback of ATP levels before and after cleaning. All results were documented by simultaneously conducting visual assessment and ATP measurements. | Visual assessment and ATP measurements | Cleanliness was improved according to visual assessment. Visual assessment correlated with the level of ATP | Yes 7/8No 1/8Unclear 0/8Not Applicable 0/8Low Risk |
| Woltering et al. 2015Germany | Prospective studyCross sectional studiesTraining appliedAudit applied | This study aims to evaluate objective observation of clean up and disinfection in the hospitals and to review obligatory corrective precautions | Samples were collected from designated spots from 5 hospitals with a UV fluorescent gel marker to control cleanliness and disinfection | Samples were collected from designated spots from 5 hospitals with a UV fluorescent gel marker to control cleanliness and disinfection | An improvement in cleanliness performance was noted after the cleaning and disinfection of surfaces with fluorescent lighting in 3 of 5 hospitals. A statistically significant improvement was noted after screening the cleanup in services. As a result, cleaning of surfaces with UV fluorescent lighting and monitoring disinfection provides an important improvement in cleaning performance. As a part of improving hospital infection control, fluorescent lighting could provide cheap and simple monitoring of cleanup performance and correcting precautions | Yes 6/8No 2/8Unclear 0/8Not Applicable 0/8Low Risk |
| Hall et al. 2016Australia | Randomized controlled studyTraining applied | To improve clean up practices, generate evidence about the effectiveness and cost-effectiveness of the cleaning. | Data was collected by performing sequential roll-out of an environmental cleaning bundle intervention to 11 Australian public and private hospitals that complied with the study criteria and agreed to participate in the study over 62 weeks, on control and intervention stages. | Each hospital evaluated the practices using its control methods. UV fluorescent marker technology, ATP tests were used for the effectiveness of clean up. Surveying was conducted to assess the change of staff knowledge level, and hospital surveillance records were used for newly formed resistant nosocomial infection rates. | It can be concluded that evidence from the REACH trial will contribute to future policy and practice guidelines about hospital environmental cleaning. | Yes 10/13No 2/13Unclear 1/13Not Applicable 0/13Low Risk |
| Chironda et al. 2016Canada | Retrospective cohort studyTraining applied | To evaluate the practice of new procedures of cleaning to improve hospital cleanliness | Process Improvement Work Group (PIWG) was created in an urban public hospital with a capacity of 515 beds in Toronto, Ontario, Canada, with the participation of Environment Services responsible for the improvement of hospital cleanliness. A total of 1558 ATP load samples were collected after the hospital rooms were cleaned. | Cleaning carried out with Accelerated Hydrogen Peroxide (AHP) with ATP method and Sodium Hypochlorite (SH) wipes were screened | ATP environmental evaluations showed a lower risk of contamination of surfaces far from the patient and surfaces cleaned with SH wipes. | Yes 10/11No 0/11Unclear 1/11Not Applicable 0/11Low Risk |
| Li et al. 2017 China | Non-randomized controlled studyTraining applied | This study to evaluates the comprehensive impact of relocating a neonatal intensive care unit (NICU) to a new facility and improved environmental cleaning practice on the presence of MRSA on inanimate surfaces | Different methods are used in two time periods in this study. In the first period, routine cleaning was carried out twice a day, with cotton cloths and hypocrites. In the second period, routine cleaning was carried out twice a day with color-coded MF cloths instead of cotton cloths. In addition to this, environmental disinfection was practiced using wet wipes moistened with disinfectant. One or two wet wipes were used for each patient section. The cleaning staff was trained on the clean up in the second period. | Microbiological samples were collected using the CHROMagar method. | The study concluded that routine clean up with MF cloths and hypochlorite and environmental disinfection practice using wet wipes moistened with disinfectants showed better results in reducing biological load and infections associated with health care services, compared to standard clean up in the first period | Yes 7/9No 2/9Unclear 0/9Not Applicable 0/9Low Risk |
| Casini et al. 2018Italy | Cross sectional studiesTraining applied | This study evaluated the effectiveness and residual disinfectant activity of disposable pre-impregnated wipes (Modified Operative Protocol, MOP) as an alternative to standard methods | Samples were collected from designated five high touch surfaces in 12-bed capacity ICUs, before and after the cleaning during carbapenem-resistant Acinetobacter baumannii (CRAB) endemoepidemic situations | In the ICU, systematic screening for CRAB colonization/infection was performed through weekly rectal swabs and/or bronchial aspirate sampling. | It is concluded that the use of disposable wipes by in-house assistant nurses on near-patient inanimate surfaces may represent a more effective alternative to the two-step procedures performed by outsourced cleaning services in reducing the microbial contamination. It is important for the assistant nurses to have a greater awareness of the crucial rule of cleaning and disinfection in infection prevention, and be trained about the proper use of wipes for forming a difference | Yes 5/8No 2/8Unclear 1/8Not Applicable 0/8Unclear Risk |
| Saleh et al. 2018Iran | Non-randomized controlled studyAudit applied | This study was conducted to evaluate the cleanliness of medical equipment used often in Neyshabur Hospital. | Microbiological samples were collected before and after the cleanup. | Study was conducted by collecting samples once in ten weeks, twice a week before and after daily cleaning. ICNA observational method and the ACC microbial method was performed on the selected sites | The results suggest that the frequency of contamination points decreased after cleaning, and the cleaning can be an effective method in eliminating microbial load. This study suggests that visual evaluation is not enough to ensure the quality of the process, and level of cleanliness must be documented with quantitative methods. Also, the study states that preparing instructions and guides and monitoring it continually would be effective in decreasing the microbial contamination. | Yes 8/9No 1/9Unclear 0/9Not Applicable 0/9Low Risk |
Joanna Briggs Institute Bias Risk Score.
Since our study is a literature review, ethical approval has not been obtained. There is no conflict of interest among the authors in our study.
FundingThis research was not funded by any public, commercial or nonprofit organizations.
ResultsAs a result of this systematic review, fourteen international articles published between the years 2005 and 2020 were found that compiled with the determining criteria. The year and the aim of the studies reviewed, method of the study, sampling methods, and results of cleaning evaluations are summarized in Table 1. Each article chosen for the study includes studies evaluating the effectiveness of cleaning carried out in of the hospital. Among the studies included herein, one were randomized controlled trials, six was a prospective intervention studies, two were case control studies and one were retrospective cohort study. The results of the studies were examined by two independent authors and consensus was achieved.
A total of 14 studies included are evaluated in means of the cleaning method they use, cleaning evaluation tool, and results. Fourteen studies emphasize that the aim of the cleaning carried out in hospitals and ICUs is to reduce environmental contamination or to prevent it. It is possible to analyze these practices under four main categories: Materials used for cleaning, the period between samplings, cleaning methods, and evaluation of cleaning. While the JBI bias score of 12 of the 14 studies included in the study was evaluated as low risk, two were evaluated as unclear risks.
Materials used for cleaningSingle-use wet wipes moistened with disinfectant, standard cotton cloths, microfiber (MF) cloths, and water –ultramicrofiber (UMF) or UMF+copper-based biocide (CuWB50) and mops made out of these materials were used in the articles reviewed for this study. SH, Hydrogen Peroxide (HP) and quaternary ammonium compounds were used as a disinfectant. According to the data we obtained from the study, Chirondo et al. (2016), Young et al. (2009), Li et al. (2017) and Casini et al. (2018) used sodium hypochlorite as the cleaning agent.20–23 While Hall et al. (2011) preferred Actichor Plus as the cleaning agent, Choi et al. (2010) used sodium dichloroisocyanurate in his study describing the method of combating epidemic.24,25 While Hydrohen peroxide was used by Chirondo et al. (2016), Hardy et al. (2007), Hall et al. (2011), Li et al. (2017) and Casini et al. (2018) used wipes or cleaning agents containing copper biocides.20,22–24,26 It is worth noting that there are studies that do not give the active substance of the agent used in the examination and describe it as detergent. Studies using detergents as cleaning agents are of Saleh et al. (2018), Al-Hamad et al. (2008), White et al. (2007), Li et al. (2017), Knape et al. (2015) and Hardy et al. (2007).22,26–30 Knape et al. (2015), compared the effectiveness of detergent with alcohol based disinfectants, Casini et al. (2018), compared the effectiveness of copper biocide-containing cleaning agent with alcohol based disinfectants.23,30 In addition, it is seen that in Chirondo et al. (2016) compares the effectiveness of sodium hypochlorite with hydrogen peroxide in his study.20
Cleaning methodsCleaning procedures in health institutions were scheduled once a day for some studies and twice a day for some.22,28 In the article about the precautions for the VRE epidemic, it was stated that the environmental cleaning was done three times a day.21 In addition to cleaning methods, such as “Mop and vacuum, spray clean and wet scrub, the steam cleaning method, and HP” standard cleaning methods determined by the institutions such as water-detergent and wiping with disinfectant were also used.23 In the studies reviewed, it is seen that methods such as “mop and vacuum” “spray clean” and “wet scrub” for floors and steam cleaning, standard water-detergent wipe method are compared.29 Cleaning efficiency, the convenience of use, and the cost of disposable wipes were also compared.20,22–24,28,30 According to the data obtained from the study, Hall et al. (2011), and Li et al. (2017) compared the effectiveness of the MF and UMF cloth and the cotton cloth in the cleaning process while Knape et al. (2015) used MF diaper.22,24,30
Casini et al. (2018) as a result of his work, he found that nurse assistants obtained better cleaning results than the cleaning company team.23 Knape et al. (2015) recommends that cleaning employees be given feedback on their cleaning as a result of their work.30
It is seen that education is applied to healthcare professionals and/or cleaning staff in 12 of the studies examined. Education is not included in the works of White and Saleh.27,29 In addition, studies suggest regular and/or aggressive monitoring of cleanliness.27,31 Woltering et al. (2015) expresses that the lack of importance given to cleaning as a result of their work will prevent other cleaning practices.31
Environmental sampling periodsWhen studied were reviewed, it was concluded that in some of the studies, environmental swabs were collected just before the cleaning, while in some studies, they were collected an hour before the cleaning to assess the effectiveness of cleaning. Swabs were collected just after the cleaning in some studies, while they were collected an hour later in the others. The fact that samples were collected before each cleaning and 0.5, 2.5, 4.5, and 6.5h after in only one study is significant.
Assessment of the effectiveness of the cleaningATP tests, microbiological sampling method, UV fluorescent marker technology, and visual assessment methods were used to assess the effectiveness of the cleaning. To assess the effectiveness of cleaning, in four studies, microbiological assessment,22,26,28,29 in one study, both ATP and microbiological method24 was used. The fact that both microbiological methods and visual assessments were used in the study by Dancer et al. (2008), Woltering et al. (2015) and Saleh et al. (2018) draws attention.27,31,32 It was seen that cleaning was assessed by fluorescent marker technology in studies by Woltering et al. (2015) and Hall et al. (2016) and it was assessed by ATP and visual assessment in the studies by Hardy et al. (2007), Chironda et al., 2016, and Knape et al. (2015).20,26,30,31,33 It was seen that cleaning was assessed by ATP technology in studies by Hall et al. (2011), and Choi et al. (2010) and it was assessed by microbiological methods in the studies by White et al. (2007), Young et al. (2009), and Al-Hamad et al. (2008).21,24,25,28,29 The fact that both fluorescent marker technology and microbiological methods were used in the study by Hall et al. (2016).33
As a result of the completion of twelve studies on assessment of cleaning equipment and the effectiveness of the cleaning done to fight MDRO infections and two studies explaining what to do in cases of epidemics were found.15,16 When the units in which the studies took place was examined, it was found that; one study was carried out in neonatal unit17 other studies took place in units following; with adult ICU having the highest number of studies,14,20–22 adult surgical clinics23–25 and elderly care units.25 It stands out that the studies published by Chironda et al. (2016), Hall et al. (2016), White et al. (2007) took place in the hospitals overall,20,29,33 while the other studies were carried out in designated places or units of the hospital, except for three studies.26–28
DiscussionICUs are one of the most important units of the hospitals that are filled with specially designed high-tech medical equipment and employed with specially trained personnel and have the precedence compared to other healthcare units in means of medical treatment and patient care. They usually have the highest bed occupancy rate. More medical equipment is used for the patients treated in these units, because of reasons such as admittance of critical patients, duration of hospital stays, monitoring of vital activity, and invasive procedures. This is important since it shows that ICU patients carry more risk of getting a nosocomial infection.27
In this compilation, studies about the cleaning, procedures, and effectiveness of the cleaning are assessed, which are carried out in environments carrying a great risk of drug-resistant microorganism infections, such as ICUs.
It seems that some of the studies comparing the cleaning method are intended to contribute to the regulation of technical specifications for the purchase of cleaning supplies for the hospital, and/or the provision of effective and low-cost services. As a result of the study conducted by Chironda et al. (2016) it is believed that wipes used for cleaning may cause environmental contamination.20 Gold et al. (2013) Sifuentes et al. (2013) and Bergen et al. (2009) it is concluded that reusing wipes without fully cleaning them may cause spreading of live bacteria by increasing biological load in the environment.34–36 For this reason, Rutala et al. (2012) and Siani et al. (2011) it is recommended to use disposable wipes moistened with disinfectant, instead of reusing cloths.37,38 Studies by Knape et al. (2015) and Li et al. (2017) support these results.22,30
When the methods used to assess the effectiveness of cleaning are compared, it is found that every method has advantages and disadvantages. While the visual assessment is easy and low-cost, it is not credible since it cannot detect the microbiological contamination in the environment and is not able to submit quantitive proof of the cleanliness.27 Hence, it is not recommended to use the visual assessment method solely in critical patient care environments in which the patient will experience the harmful effects of contamination at a greater level. However, UV fluorescent marker technology makes it possible to control the cleanliness of hospital environments fast and at a low-cost. Because it is easy to apply, this method is also suitable for outpatient care centers.31 However, since this method cannot detect the contamination of the environment, like visual assessment, it can be foreseen that it won’t be suitable to use alone, in critical patient care environments. ATP method is intriguing due to having advantages such as giving fast results, making it possible to assess the cleaning quantitively, detecting the biological load in the environment.39 But in this method could be misleading to collect random ATP samples from hospital surfaces to decide whether a clinic or a room is “clean” or “dirty.” Therefore, the ATP method can only provide insight into the area from that samples were collected. In this sense, the ATP method is not adequate to assess the cleanliness of the hospital alone, since it can only assess a limited part of a large area. To assess all surfaces cleaned, it is recommended to use the ATP method with visual assessment.30
When the studies were reviewed, the period between the collection of samples is another point that caught our attention. Common ground in all reviews of the studies is that the environmental samples were collected before and after the cleaning. In some studies, samples were collected just before the cleanings, and in some, they were collected an hour before it. Similarly, samples after the cleaning were collected 1h after the cleaning, except for one study in which the samples were collected 0.5, 2.5, 4.5, and 6.5h after the cleaning.23 In addition to this, in one study, it is specified that there should not be any detergent residue in the environment and the environment should be dry for the ATP method, as detergent residue and ATP could interact and cause false results.40 The use of disinfectant is needed in cases where standard cleaning cloths or mop is used to remove pathogens.37,38 Additionally, MF and UMF cloths are superior to cotton cloths, if used repeatedly. MF cloths are 10 times more absorbent compared to other cloths and do not accommodate bacteria. Hall et al. (2011) in one study, two significant effects of cleaning done with UMF cloth moistened with CuWB50 are identified.24 The first one is direct antimicrobial effects, which occurred after cleaning. The second one is reducing the bacterial level up to 23h after cleaning.24 Ready to use wipes are used more and more in health care environments. However, one study suggests that different antimicrobial wipes show a variant effect in removing microbial biofilms from inanimate objects and reducing pathogen transfers between surfaces.41
In one of the articles reviewed in our study Hardy et al. (2007) decontamination with hydrogen peroxide vapour (HPV) is used aside from wiping with disinfectant.26 HPV is a quite effective method in removing bacteria from the environment for unit cleaning. But the unit must be emptied before the use of this method, and disinfectant residue in the environment must be recleaned with the standard method after HPV decontamination. Besides, the recontamination of the unit after 24–48h after the patients are admitted to the unit, shows that HPV is not an efficient method that can comply with expectations. Therefore, the HPV method has disadvantages because it requires more time, is inconvenient, and is costly. In cases in which no patients will be admitted to the unit after HPV decontamination, it is a suitable method to remove nosocomial bacteria from the unit completely.26
Two of the articles are case control studies and advice on controlling epidemics.21,25 Both studies give the common advice as following; Preventing the health staff from being carriers by contact precautions, reducing environmental contamination by cleaning clinical areas including medical equipment, staff education, and assessment of environmental cleanliness with surface cultures.
Training was applied in 12 of the studies examined. As a result of this determination, it can be concluded that the importance of cleaning staff for cleaning is directly proportional to the success of other hygiene practices. For this reason, it is necessary to train cleaning staff to make cleaning effective. ATP and UV fluorescent marking, which are the objective assessment tools used in evaluating cleaning, can be used as educational tools. Because seeing the pollution can cause the cleaning staff to be careful. Education is not included in the works of White and Saleh.27,29 In addition, when the results of the studies are examined, regular and aggressive control of cleaning increases the success of cleaning.
Limitations of the studyThe fact that there are studies not evaluating the effectiveness of cleaning, cleaning studies not concerning MDRO and VRE infections, studies conducted in non-clinical areas of the hospital, and studies whose full texts are not available on the databases, create the limitations of this review; which are mentioned under the methodology title.
ConclusionMulti-drug resistant microorganism infections are very common in hospitals, especially in ICUs. Due to high number of patients and the use of medical equipment that requires constant cleaning for patient care, the hospitals become a reservoir of possible pathogens. In this sense, the latest studies on the quality of environmental clean-up show that microbial contamination is not prevented despite the efforts to clean all surfaces efficiently. For this reason, actively done environmental cleaning and the assessment of the results carry vital importance in hospitals, especially in ICUs. Today, assessment of cleaning activity in environments that provide healthcare can be evaluated by different methods, but there are advantages and disadvantages of these methods. For this reason, in concerned literature, it is suggested that cleaning must be evaluated by several methods, not only one. Also, training the staff that carries out the cleaning, appreciating correct behavior by giving feedback are important approaches to increase the effectiveness of the cleaning. It is recommended that the disinfectants are concentrated suitably to the area that will be cleaned and is in contact with the area a suitable duration for efficient cleaning. In addition, the use of disposable wipes moistened with disinfectant and CuWB50 and UMF cloths are also recommended to use prevent environmental contamination. During epidemics, the use of CuWB50 and UMF cloths is recommended for reducing the quantity of bacterial count. Also, an inspection of the cleaning is another major factor to increase the quality of the cleaning. Forming ‘Cleaning packages’ that merge more than one evidence-based intervention could have the potential to prevent cross-contamination that could form during the maintenance period.
Recommendations for clinical practiceAn important way to support healing is to clean the patient's surroundings. Transmitting of microorganisms from the environment to the patients mostly happens via contact with surfaces. The most efficient and economical way to reduce the incidences of hospital infections is efficient cleaning procedures and measurable results. In this sense, as a result of this study; it is recommended to:
- -
Organize regular in-service training, since it is thought that sensibility and information level of the person who is doing the cleaning could change the efficiency of cleaning.
- -
Regularly inspect staff for the reasons that it could affect the quality of the cleaning. Clean the patient units every day, regularly with efficient cleaning methods and equipment, because the contamination in the patient environment is faster compared to areas away from the patient and has a higher possibility of not being cleaned. And increase the number of cleanings during epidemic.
The authors declare that they have no conflict of interest.

