



To determine the maternal and perinatal impact of pregnant women with SARS-CoV-2 positive polymerase chain reaction during childbirth and post clinical period.
MethodObservational descriptive, retrospective, and multicentre study carried out through the review of clinical records of pregnant women admitted for delivery from 1 March to 30 June 2020.
ResultsThirteen women with SARS-CoV-2 positive polymerase chain reaction were tested. The prevalence of positive cases was 0.48% of the total number of births attended during the study period. None of the mothers developed complications from COVID-19 infection, nor did they require admission to the Intensive Care Unit. Of the births, 15.4% ended in caesarean section, 7.7% were premature, 53.8% of the newborns were isolated from their mothers, 61.5% had late clamping of the umbilical cord and the rate of exclusive breastfeeding at discharge was 76.9%. All the newborns were polymerase chain reaction-negative for COVID-19 and had no postpartum complications.
ConclusionsVertical transmission during childbirth in newborns of COVID-19 positive mothers has not been reported. Clinical practices not supported by scientific evidence were detected at the beginning of the pandemic and adapted to international recommendations as the pandemic evolved.
Determinar las repercusiones maternas y perinatales de las gestantes con reacción en cadena de la polimerasa positiva para SARS-CoV-2 durante el parto y el puerperio clínico.
MétodoEstudio observacional descriptivo, retrospectivo y multicéntrico realizado mediante la revisión de historias clínicas de las gestantes ingresadas por parto desde el 1 de marzo hasta el 30 de junio de 2020.
ResultadosSe analizaron 13 mujeres con reacción en cadena de la polimerasa positiva a SARS-CoV-2. La prevalencia de casos positivos fue del 0,48% sobre el total de partos atendidos en el periodo de estudio. Ninguna de las madres desarrolló complicaciones derivadas de la infección por COVID-19 ni necesitó ingreso en la Unidad de Cuidados Intensivos. El 15,4% de los partos terminó en cesárea, el 7,7% fueron prematuros, el 53,8% de los recién nacidos fueron aislados de su madre, en el 61,5% se realizó pinzamiento tardío del cordón umbilical y la tasa de lactancia materna exclusiva al alta fue del 76,9%. Todos los recién nacidos fueron negativos a COVID-19 mediante reacción en cadena de la polimerasa y no tuvieron complicaciones posteriores al parto.
ConclusionesNo ha quedado constatada la transmisión vertical durante el parto en los recién nacidos de madres positivas a COVID-19. Han sido detectadas prácticas clínicas no avaladas por la evidencia científica al inicio de la pandemia que han ido adaptándose a las recomendaciones internacionales a medida que esta evolucionaba.
The SARS-CoV-2 pandemic has affected care during maternity, directly influencing attention during birth and contributing to interventions which are hardly supported by scientific evidence, such as separating mothers from their newly born baby.
What does this paper contribute?Many of the women who give birth while COVID-19 positive remain asymptomatic, and vaginal birth does not cause an increase in the vertical transmission of the SARS-CoV-2 virus to new-born babies. Within the context of this pandemic it is fundamental to respect practices such as accompanying women during birth, not separating mothers from new-born infants and breastfeeding.
The disease caused by SARS-CoV-2 is now a worldwide medical emergency.1 SARS-CoV-2 may cause severe disease, above all in older individuals with concomitant diseases, although the whole population is susceptible to infection.2
Experience with known viral infections during pregnancy shows an increase in maternal complications, including spontaneous abortions, premature membrane rupture and prematurity.2 In particular, previous outbreaks of other types of coronavirus showed that pregnant women who were infected may suffer severe complications such as acute respiratory syndrome, anxiety syndrome and multiple organ failure.3 It is well-known that viral pneumonia, especially when it is accompanied by comorbidities (such as cardiovascular problems and chronic respiratory problems or obesity) may significantly increase maternal and neonatal morbidity.2
Given the uncertain prognosis for pregnant women affected by SARS-CoV-2 in the first months of the pandemic, many concerns arose regarding the clinical management of such a sensitive group of patients.3 The main aim of this study was therefore to determine the maternal and perinatal repercussions during birth and the clinical puerperium in pregnant mothers infected by SARS-CoV-2 in the Valencian Community. The secondary objectives were to determine the existence or absence of vertical transmission, and to describe the maternal care given during the epidemic and the type of lactation implemented.
MethodThis descriptive, observational, retrospective and multicentre study was undertaken in 5 public hospitals in the Valencian Community (Hospital Universitario de La Ribera, Hospital Lluis Alcanyis, Hospital de Ontinyent, Hospital General de Valencia and Hospital Universitari i Politècnic La Fe).
The target population were women who gave birth in these hospitals. The inclusion criteria were: a positive polymerase chain reaction (PCR) determination for SARS-CoV-2, a new-born infant with a positive PCR determination for SARS-CoV-2 and a single pregnancy. Pregnant women with a positive PCR admitted for a medical or surgical reason other than birth were excluded. All of the positive cases seen during the data gathering period were included.
Participant data were obtained from the electronic registries of their clinical histories from 1 March to 30 June 2020. Sociodemographic, obstetric and clinical variables were recorded, together with those in connection with lactation. Quantitative variables were expressed as an average with standard deviation or their median and interquartile range, depending on their nature. Qualitative variables were expressed as percentages and absolute frequencies. Statistical analysis was performed using IBM® SPSS® v.22 software.
This study was approved by the Research Ethics Committee of the Research Commission of Hospital Universitario de La Ribera (Registration number: HULR2020_27), as well as by the other hospitals.
ResultsThirteen women and their new-born infants were included. Respecting the distribution of the hospitals, 38.5% (n=5) were treated in La Fe, 30.8% (n=4) in La Ribera, 15.4% (n=2) in the Hospital General de Valencia, 7.7% (n=1) in Hospital Lluis Alcanyis and 7.7% (n=1) in Hospital de Ontinyent. The prevalence of positive cases amounted to 0.48% of the total number of births seen during the study period.
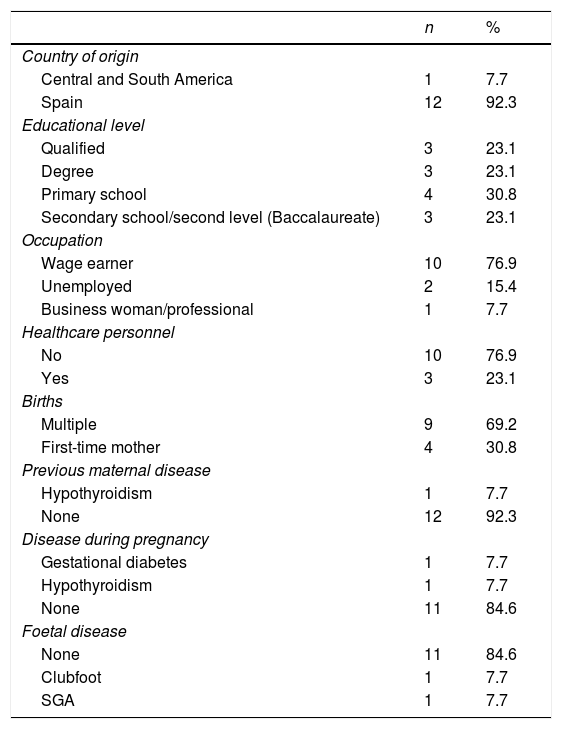
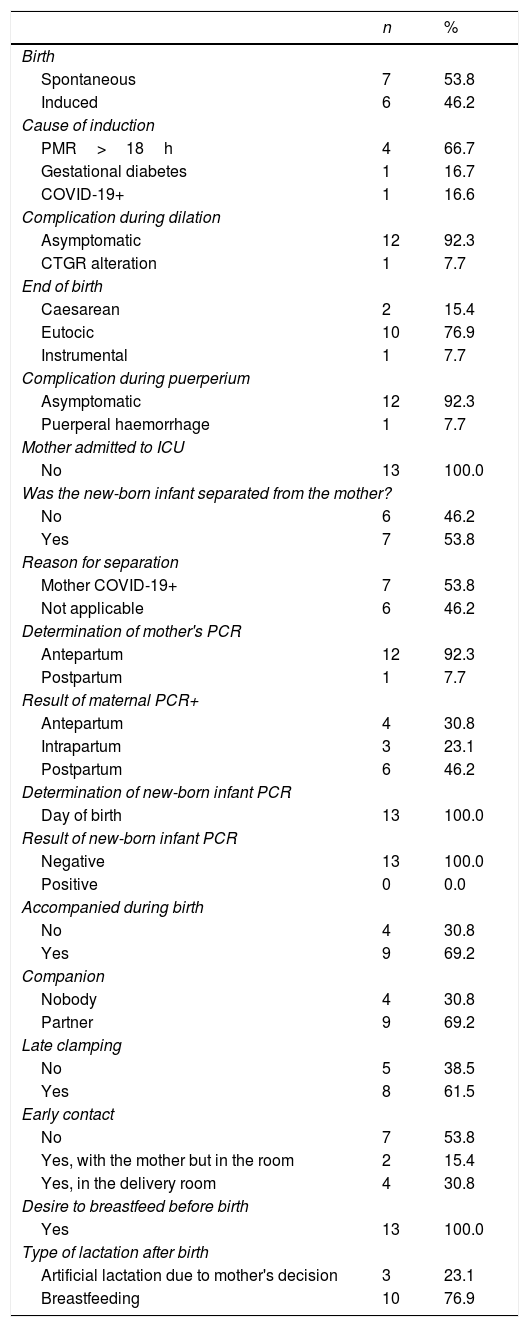
The average age of the women was 35.31±4.2 years. Almost one third of the infected pregnant women were first-time mothers (30.8%, n=4), without any previous maternal disease (92.3%, n=12), gestational disease (84.6%, n=11) or foetal disease (84.6%, n=11) (Table 1). 53.8% (n=7) of the births commenced spontaneously. In 16.6% (n=1) birth the cause of induction was attributed to SARS-CoV-2 infection. 76.9% (n=10) of the births were eutocic and 15.4% (n=2) terminated in caesarean section. The causes of the latter were the risk of losing foetal well-being and knowledge of the positive result of the COVID-19 test in a case of premature membrane rupture (>18h) with a previous caesarean. There was one case of post-partum haemorrhage (7.7%). None of the women were admitted to the Intensive Care Unit after giving birth, and nor did they show any symptoms during the same (Table 2).
Sociodemographic and obstetric characteristics of the sample (n=13).
| n | % | |
|---|---|---|
| Country of origin | ||
| Central and South America | 1 | 7.7 |
| Spain | 12 | 92.3 |
| Educational level | ||
| Qualified | 3 | 23.1 |
| Degree | 3 | 23.1 |
| Primary school | 4 | 30.8 |
| Secondary school/second level (Baccalaureate) | 3 | 23.1 |
| Occupation | ||
| Wage earner | 10 | 76.9 |
| Unemployed | 2 | 15.4 |
| Business woman/professional | 1 | 7.7 |
| Healthcare personnel | ||
| No | 10 | 76.9 |
| Yes | 3 | 23.1 |
| Births | ||
| Multiple | 9 | 69.2 |
| First-time mother | 4 | 30.8 |
| Previous maternal disease | ||
| Hypothyroidism | 1 | 7.7 |
| None | 12 | 92.3 |
| Disease during pregnancy | ||
| Gestational diabetes | 1 | 7.7 |
| Hypothyroidism | 1 | 7.7 |
| None | 11 | 84.6 |
| Foetal disease | ||
| None | 11 | 84.6 |
| Clubfoot | 1 | 7.7 |
| SGA | 1 | 7.7 |
SGA: small for gestational age.
Characteristics and care during birth and the puerperium (n=13).
| n | % | |
|---|---|---|
| Birth | ||
| Spontaneous | 7 | 53.8 |
| Induced | 6 | 46.2 |
| Cause of induction | ||
| PMR>18h | 4 | 66.7 |
| Gestational diabetes | 1 | 16.7 |
| COVID-19+ | 1 | 16.6 |
| Complication during dilation | ||
| Asymptomatic | 12 | 92.3 |
| CTGR alteration | 1 | 7.7 |
| End of birth | ||
| Caesarean | 2 | 15.4 |
| Eutocic | 10 | 76.9 |
| Instrumental | 1 | 7.7 |
| Complication during puerperium | ||
| Asymptomatic | 12 | 92.3 |
| Puerperal haemorrhage | 1 | 7.7 |
| Mother admitted to ICU | ||
| No | 13 | 100.0 |
| Was the new-born infant separated from the mother? | ||
| No | 6 | 46.2 |
| Yes | 7 | 53.8 |
| Reason for separation | ||
| Mother COVID-19+ | 7 | 53.8 |
| Not applicable | 6 | 46.2 |
| Determination of mother's PCR | ||
| Antepartum | 12 | 92.3 |
| Postpartum | 1 | 7.7 |
| Result of maternal PCR+ | ||
| Antepartum | 4 | 30.8 |
| Intrapartum | 3 | 23.1 |
| Postpartum | 6 | 46.2 |
| Determination of new-born infant PCR | ||
| Day of birth | 13 | 100.0 |
| Result of new-born infant PCR | ||
| Negative | 13 | 100.0 |
| Positive | 0 | 0.0 |
| Accompanied during birth | ||
| No | 4 | 30.8 |
| Yes | 9 | 69.2 |
| Companion | ||
| Nobody | 4 | 30.8 |
| Partner | 9 | 69.2 |
| Late clamping | ||
| No | 5 | 38.5 |
| Yes | 8 | 61.5 |
| Early contact | ||
| No | 7 | 53.8 |
| Yes, with the mother but in the room | 2 | 15.4 |
| Yes, in the delivery room | 4 | 30.8 |
| Desire to breastfeed before birth | ||
| Yes | 13 | 100.0 |
| Type of lactation after birth | ||
| Artificial lactation due to mother's decision | 3 | 23.1 |
| Breastfeeding | 10 | 76.9 |
PCR: polymerase chain reaction; PMR: premature membrane rupture; CTGR: cardiotocography recording; ICU: intensive care unit.
Ninety-two point three percent (n=12) of the new-born infants were born at term, with an average gestational age of 38.6±1.5 weeks. The Apgar test after 1min and at 5min gave a median of 10 (interquartile range 9–10) points. The umbilical cord was clamped late in 61.5% (n=8) of cases, and in 46.2% (n=6) cases skin to skin contact was made. Before birth the desire to breastfeed was total, although after learning of the positive COVID-19 result, 23.1% (n=3) decided not to do so. 53.8% (n=7) of the new-born babies were separated from their mothers and admitted to the neonatal Intensive Care Unit as an isolation measure, after which no complication was identified during admission (median admission 2 days, interquartile range 1–3). All of the new-born infants were found to be negative in PCR for SARS-CoV-2. A retest was performed in 23.1% (n=3) of cases 24h and 48h after admission, and these tests were negative. 69.2% (n=9) of their partners accompanied the women during birth (Table 2).
DiscussionThe clinical characteristics of this series of women were similar to those reported in other publications.4 The scientific literature shows that pregnancy does not increase the probability of complications associated with COVID-19, although some have been described.2
Due to the current pandemic and the threat of new waves caused by SARS-CoV-2, it is necessary to have clinical data which aid clinical decision-making. This scenario and the swift modification and adaptation of working routine in maternity care across Europe5 has meant that concern has increased about ensuring safe care for pregnant women, sometimes leading to medical interventions that were not properly justified.5 These factors may have affected compliance with care quality indicators, giving rise to situations that may have been classified within the context of obstetric violence, although they were masked by the structural and medical context arising from SARS-CoV-2.6
Regarding the maternal care and right of COVID-19 positive women, several important points for concern exist: being accompanied during birth, skin-to-skin contact, not separating mothers from their new-born baby and breastfeeding.5 Although the recommendations of the Ministry of Health support the implementation of all 4 elements, it seems that clinical practice differed.
This study shows a certain degree of variability respecting being accompanied during birth. This practice is not solely governed by a right, as it is also associated with increased safety and well-being for women during birth.7 Movements by midwives’ collectives in the Valencian Community may have influenced the change of attitude to this aspect.8
Vertical infection of the new-born infants was ruled out in the sample. Contact between mothers and their new-born infants was maintained in this study, given its premise of not causing harm.2,9 Moreover, separating a mother from her healthy new-born child in a healthcare system under stress leads to increased workload for the system and the professionals involved, who have worked above their capacities during the whole duration of the pandemic.
No studies were found that offer data on the late clamping of the umbilical cord during the pandemic. Nevertheless, the high general percentage of caesarean sections, systematic separations and strict measures of isolation may have led to the abandonment of this practice.2 The consequences of certain clinical actions due to the pandemic in terms of the health of new-born infants have yet to be determined. These actions include early clamping of the umbilical cord, isolating new-born babies from their mother or preference for bottle feeding.
This study seems to indicate a certain degree of rejection of breastfeeding in women who know they are COVID-19 positive. The causes of this rejection may include fear of infecting their baby,2 although the strict measures to prevent the horizontal transmission of the virus may also have had an influence. There were many recommendations to discourage or forbid breastfeeding during the first wave of SARS-CoV-2.2,10 Different scientific societies have gradually adapted or modified their protocols for action during the pandemic. The latest versions of these protocols express the advisability of non-separation, skin-to-skin contact and the encouragement of breastfeeding.
LimitationsAlthough this study centres on a small group of women, it is important to underline that European Union countries have reported changes in how pregnant women and their families are treated.5 In the majority of cases retrospective data gathering is influenced by the lack of records. In this case, given the exceptional nature of the cases treated in each one of the hospitals, it was complete and exhaustive. Awareness of the positive PCR result of the mother may affect the results, above all in the management of the new-born infant during the first months (March and April) of the pandemic, as this may have led to increased restrictions.
All of the women analysed were asymptomatic and had no complications. No vertical transmission to the new-born infants of SARS-CoV-2 positive mothers was detected in this study. During the first months of the pandemic, the lack of available scientific evidence on SARS-CoV-2 had a negative effect on birth, puerperium and breastfeeding management in the COVID-19 positive women, as they were separated from their new-born babies. This affected early skin-to-skin contact and reduced beneficial practices such as late clamping of the umbilical cord and breastfeeding.
Conflict of interestsThe authors have no conflict of interests to declare.
We would like to thank Víctor Manuel González-Chordá and Francisco Javier Soriano-Vidal for all their help and valuable contributions to this work. We would also like to thank all of the obstetric and paediatric staff who took part in caring for the cases, for their work and dedication.
Please cite this article as: Vila-Candel R, Mena-Tudela D, Gómez-Seguí A, Asensio-Tomás N, Cervera-Gasch A, Herraiz-Soler Y. Manejo del parto, el puerperio y la lactancia en mujeres positivas para SARS-CoV-2. Estudio multicéntrico en la Comunidad Valenciana. Enferm Clin. 2021;31:184–188.
