









To describe the levels of fear of recurrence in cancer patients in the follow-up phase.
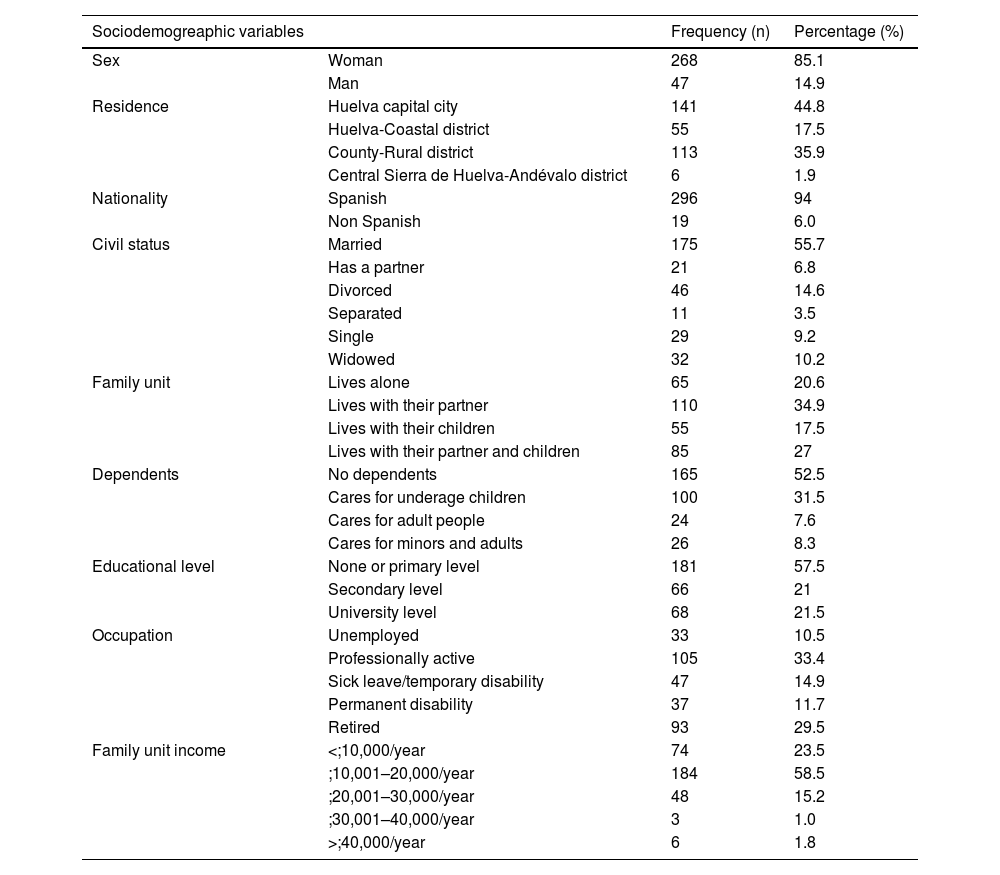
MethodCross-sectional descriptive study carried out from June 2023 to February 2024. A sample of 315 adult patients with a diagnosis of non-metastatic cancer in the process of follow-up at least 6 months after the end of active treatment, seen in the oncology department of the Juan Ramón Jiménez University Hospital in Huelva, was included. The FCR7-SP questionnaire was used to measure fear of recurrence. Permission was obtained from the Provincial Ethics Committee. Data analysis was performed using SPSS software v.29.0.1.0.
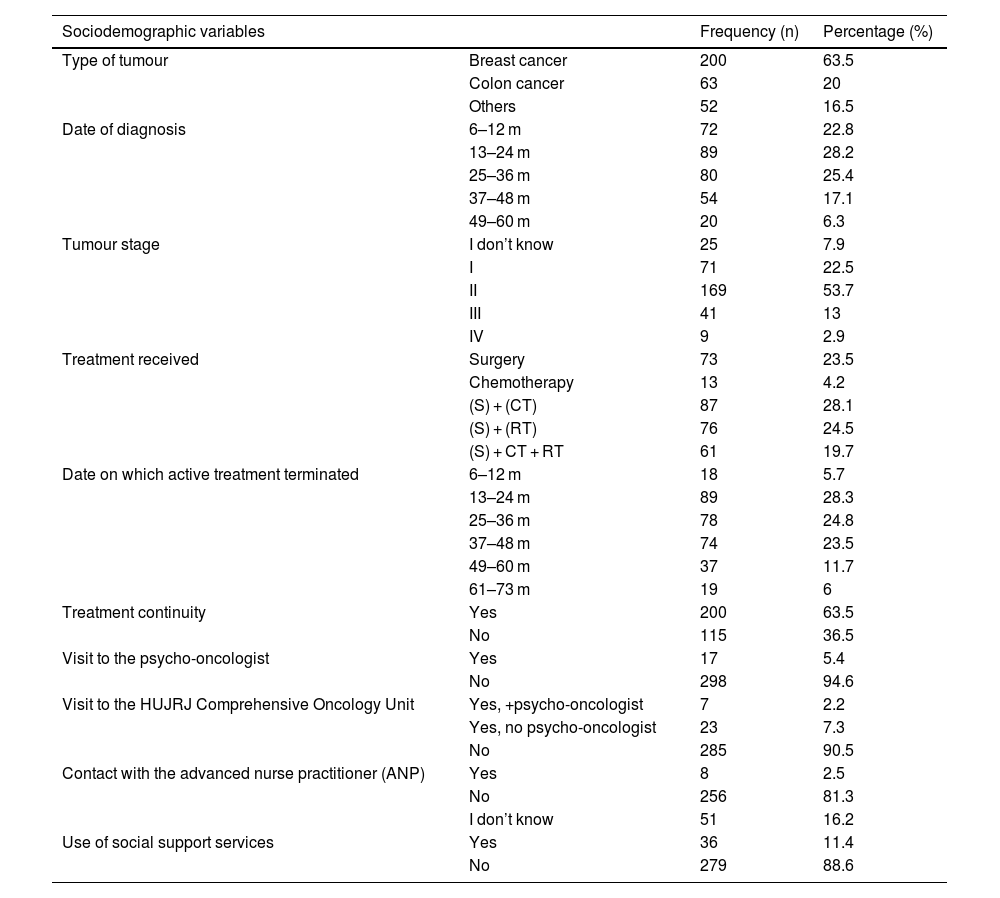
ResultsAn average score of 26.5 out of 35 points was observed on the FCR7-SP scale, suggesting a moderate level of fear. Mean age was 57.91 years (SD ± 11.80). The most frequent cancer was breast cancer (63%) followed by mostly stage II colorectal cancer (20%). There is a statistically significant relationship between fear of recurrence and gender, nationality, treatment and type of cancer. Five cut-off points of the FCR7-SP scale are proposed based on the percentiles obtained.
ConclusionsThe level of fear of recurrence in cancer patients in the follow-up phase at the Juan Ramón Jiménez University Hospital in Huelva is moderate. It is essential to identify the factors that influence the level of fear of recurrence in order to design preventive interventions and/or an early approach.
Describir los niveles de miedo a la recidiva en pacientes oncológicos en fase de seguimiento.
MetodologíaEstudio descriptivo transversal llevado a cabo desde junio de 2023 hasta febrero de 2024. Se incluyó una muestra de 315 pacientes adultos, con diagnóstico de cáncer no metastásico en proceso de seguimiento tras al menos 6 meses después de la finalización del tratamiento activo, atendidos en consulta de Oncología del Hospital Universitario Juan Ramón Jiménez de Huelva. Se utilizó el cuestionario para medir el miedo a la recidiva el FCR7-SP. Se obtuvo el permiso del Comité de Ética Provincial. El análisis de datos se realizó con el programa SPSS® v.29.0.1.0.
ResultadosSe observó una puntuación media de 26,5 sobre 35 puntos en la escala de FCR7-SP, lo que sugiere un nivel moderado de miedo. La media de edad fue 57,91 años (DE ± 11,80). El cáncer más frecuente fue el cáncer de mama (63%) seguido del cáncer colorrectal (20%) en estadio II mayoritariamente. Existe una relación estadísticamente significativa entre el miedo a la recidiva y género, nacionalidad, tratamiento y tipo de cáncer. Se proponen cinco puntos de corte de la escala FCR7-SP en base a los percentiles obtenidos.
ConclusionesEl nivel de miedo a la recidiva en los pacientes oncológicos en fase de seguimiento del Hospital Universitario Juan Ramón Jiménez de Huelva es moderado. Es fundamental identificar los factores que influyen en el nivel de miedo a la recidiva para diseñar intervenciones preventivas y/o abordaje precoz.
