





The purpose of the study was to identify the impact of family empowerment model intervention on family satisfaction and children’s length of stay in the hospital due to pneumonia.
MethodThe design of the study was that of a quasi-experiment. About 83 family-child groups were divided into 42 pair in the intervention group and 41 pair in the control group; which were recruited using consecutive sampling using certain inclusion criteria. Three district hospitals in Jakarta were used in this study. A questionnaire and family empowerment instrument were developed and used to collect the data. An analysis of the data used independent and paired t-test.
ResultsThe results of the study showed a significant difference between the intervention and control groups in empowerment and satisfaction aspects after the intervention (p= 0.000; p= 0.000). An analysis of length of stay using the t-test indicates a significant difference between the intervention and control groups (p= 0.000).
ConclusionsThe family empowerment model (FEM) intervention has a positive impact on families, as it can increase both the satisfaction and the empowerment of the family. Another important indicator of the FEM’s success is its ability to decrease the length of stay of patients.
In developing countries, an estimated three million neonates and children under the age of 5 die each year from pneumonia—the equivalent of 8,200 every day1. A variety of risk factors for pneumonia exist, such as low socioeconomic status, low level of mother’s education, inappropriate child care, high population area, incomplete immunization status, especially for measles, premature baby, inadequacy of breast milk consumption, climate change, anemia, malnutrition, house pollution, passive smoker, and house lacking kitchen ventilation2–5. Around 7-13% of pneumonia cases oc-curring in the community are quite severe and require hos-pitalization, as early detection and management are still poor5.
Hospitalization for children under 5 is an unpleasant, painful, irritating, fearful, and stressful experience, as they have to be separated from their closest persons and placed in a new environment6,7. The parents are believed to be the most important ecological factor that can minimize the effects of a child’s hospitalization. Thus, it would appear that family-centered care is the main concept in pediatric nursing practices.
A qualitative study that aimed to explore the meaning of family’s or parents’ involvement from pediatric nurses’ perspective highlighted the empowerment issue8. The issue can be solved by clearly identifying the essential tasks and roles shared between the nurse and the family. There are advanced roles that the family can fill after they obtain knowledge related to nurses’ roles when dealing with children who need care in their homes. Likewise, a qualitative study that aimed to view family empowerment from the perspective of family and nurses has identified three main themes, which are: (1) family empowerment understanding, (2) the family empowerment process, and (3) family empowerment effects9. The term “empowerment” refers to a process that includes boosting the awareness a person needs to cooperate in care10. Furthermore, other studies have called attention to the term “psychological empowerment”, which refers to a motivation construction that has four cognitions: meaning, competency, self-determination, and effect/impact11.
Empowerment is closely related to the education and promotion process. The success of this process depends on the support received from the internal and external factors of family. The external factors include support from the hospital environment, support from health care providers, and caring from health care providers to children and their families, whereas internal factors include motivation, self-efficacy, and caring from families to children. The implementation of health promotion through health education has moved from a community-based process to a hospitalbased one, fitting in appropriately with nurses’ role and functions12. One of nurses’ responsibilities as health care providers is to empower the family or parents of the patient13. However, the success of the health education provided to the family can be affected by demographic factors, such as education level, employment, socioeconomic status, severity of the child’s condition, and family mental status14.
The studies presented thus far provide evidence that research focusing on how to maximize the family’s role through education that nurses provide is of paramount importance. Therefore, the main purpose of this study was to identify the impact of family empowerment model (FEM) intervention on families’ satisfaction and children’s length of stay in the hospital.
MethodThe quantitative quasi-experimental design was employed in this study. The respondents were families of under-5-year-old children who were hospitalized with pneumonia. The inclusion criteria were: (1) Under-5-year-old children were diagnosed by the doctors responsible for the patients (DRP) with pneumonia; (2) the family or parents of these subjects were the mother/ father/ other family members responsible for taking care of the children; (3) the families were able to read and write; and (4) the children were treated in the third class ward. The main variables in this study are the characteristics of the respondent dyad of family-child (ethnicity, education, number of children, child gender, and hospitalization history), empowerment, family satisfaction, and length of stay of children with pneumonia. For the total respondents of 83 families, 42 were in the intervention group, and 41 were in the control group. Two groups of subjects were recruited from three district general hospitals in Jakarta. The data collection techniques that were used in the study were questionnaires and instruments (focusing on satisfaction and empowerment). Two sets of anonymized questionnaires and instruments were completed by the family before and after the intervention of the FEM.
In an attempt to control for bias, the pre-test for the intervention and control groups was performed on the first day of the child’s hospitalization. For the intervention group, immediately after the family adaptation phase, the trained nurses provided health education related to pneumonia. The health education was carried out individually/ in groups using a flipchart and booklets for a maximum duration of 45 minutes. The intervention was given immediately on the first day of hospitalization to prevent the family from receiving information about pneumonia from other health care professionals. The family empowerment module, which contains information on pneumonia and nursing care for children with pneumonia focusing on the family, family empowerment and concepts related to empowerment (motivation, caring, social support, and self-efficacy), was prepared to support the trained nurses in performing the intervention. The post-test was performed on the last treatment day, before the child of the respondent was to be discharged from the hospital.
Family empowerment is seen from the score of all constructs of the empowerment instrument ranging from the value of 82-328. Another instrument was also applied to measure the level of satisfaction of the family. For categorical data, an analysis was performed using a frequency distribution. Meanwhile, the t-test and paired t-test were employed to analyze the numerical data to determine the most significant impact on family empowerment. Ethical approval for the study was obtained from the Ethical Board Faculty of Nursing Universitas Indonesia.
ResultsThe results of this study were processed through two types of statistical analysis: univariate and bivariate. The results from the univariate analysis can be seen in Tables 1 and 2, whereas the results from the bivariate analysis can be seen in Tables 3-5.
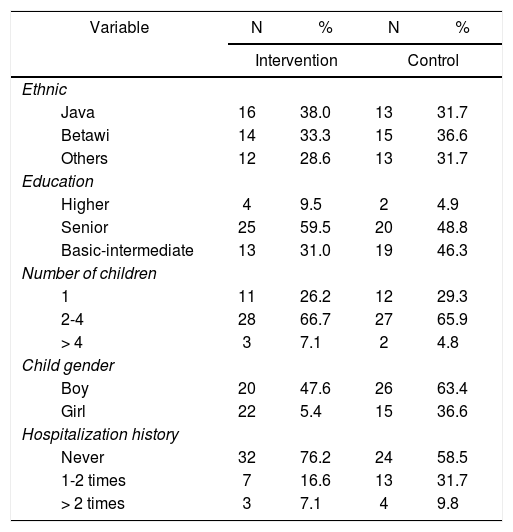
Distribution of Intervention and control groups: family-child characteristics in three hospitals, August-November 2014 (N=83).
| Variable | N | % | N | % |
|---|---|---|---|---|
| Intervention | Control | |||
| Ethnic | ||||
| Java | 16 | 38.0 | 13 | 31.7 |
| Betawi | 14 | 33.3 | 15 | 36.6 |
| Others | 12 | 28.6 | 13 | 31.7 |
| Education | ||||
| Higher | 4 | 9.5 | 2 | 4.9 |
| Senior | 25 | 59.5 | 20 | 48.8 |
| Basic-intermediate | 13 | 31.0 | 19 | 46.3 |
| Number of children | ||||
| 1 | 11 | 26.2 | 12 | 29.3 |
| 2-4 | 28 | 66.7 | 27 | 65.9 |
| > 4 | 3 | 7.1 | 2 | 4.8 |
| Child gender | ||||
| Boy | 20 | 47.6 | 26 | 63.4 |
| Girl | 22 | 5.4 | 15 | 36.6 |
| Hospitalization history | ||||
| Never | 32 | 76.2 | 24 | 58.5 |
| 1-2 times | 7 | 16.6 | 13 | 31.7 |
| > 2 times | 3 | 7.1 | 4 | 9.8 |
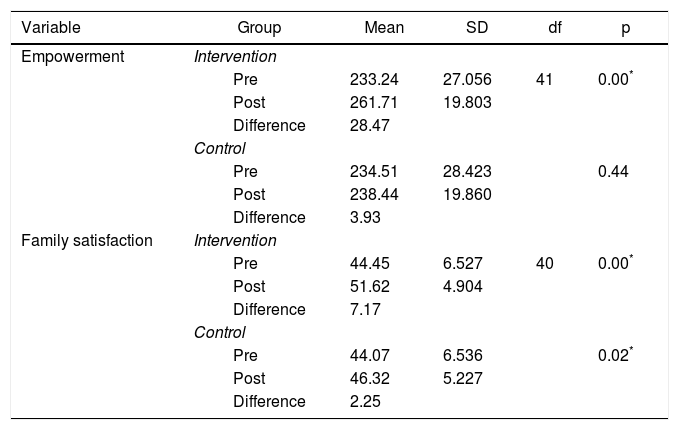
Empowerment and family satisfaction scores’ difference between intervention and control groups in three hospitals, August-November 2014 (N=83).
| Variable | Group | Mean | SD | df | p |
|---|---|---|---|---|---|
| Empowerment | Intervention | ||||
| Pre | 233.24 | 27.056 | 41 | 0.00* | |
| Post | 261.71 | 19.803 | |||
| Difference | 28.47 | ||||
| Control | |||||
| Pre | 234.51 | 28.423 | 0.44 | ||
| Post | 238.44 | 19.860 | |||
| Difference | 3.93 | ||||
| Family satisfaction | Intervention | ||||
| Pre | 44.45 | 6.527 | 40 | 0.00* | |
| Post | 51.62 | 4.904 | |||
| Difference | 7.17 | ||||
| Control | |||||
| Pre | 44.07 | 6.536 | 0.02* | ||
| Post | 46.32 | 5.227 | |||
| Difference | 2.25 |
* p=a < 0.05.
Differences in empowerment and satisfaction scores: post-intervention between intervention and control groups in three hospitals, August-November 2014 (N=83).
Length of stay score difference between intervention and control groups in three hospitals, August-November 2014 (N=83).
| Group | n | Mean | SD | df | 95%CI | P |
|---|---|---|---|---|---|---|
| Intervention | 42 | 4.64 | 1.96 | 41 | 4.03-5.23 | 0.00* |
| Control | 41 | 5.29 | 1.96 | 40 | 4.67-5.91 |
The univariate analysis in this study described that the majority of respondents’ ethnic groups were Javanese and Betawi in both the intervention and control groups. Pneumonia occurred in both genders. However, pneumonia tended to appear more commonly in boys than in girls. Based on the history of hospitalization, the majority of the children (67.5%) in this study had never been hospitalized, whereas 27 out of 83 children (32.5%) had experienced recurrent hospitalization. The high percentage of recurrent hospitalization showed that both health education programs and discharge planning in the hospital need to be improved (Table 1).
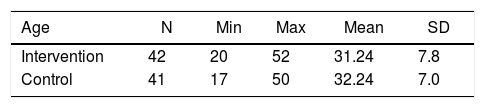
The age of the majority of the respondents (mothers) was similar in the intervention and control groups, which was around 31-32 years old (Table 2). A homogeneity test was employed to make sure that the intervention was not affected by the characteristics of the respondents. The results showed that the characteristics of the respondents in both the intervention group and the control group were similar (α > 0.05).
Bivariate analysisThe bivariate analysis showed a significant difference in the empowerment score in the intervention group before and after the intervention. Meanwhile, the empowerment score in the control group showed no significant difference between before and after the intervention (Table 3). The analysis indicated that the differences between the empowerment and satisfaction scores in the two groups were statistically significant (p < 0.05) (Table 4). Further more, the length of stay also described a significant difference statistically between the intervention group and the control group (p < 0.05) (Table 5).
DiscussionThe results of this study indicated that pneumonia occurred more in the Javanese and Betawi ethnicities than in others. It may impact the majority of those ethnicities living in Jakarta. Furthermore, some authors have speculated about how cultural backgrounds can affect individuals. Cultural background was explained as one of many factors that can affect individual knowledge and also influence a family’s way of thinking and acting15–17. Extensive knowledge can also contribute to families’ practice of taking care of their children. Knowledge also has an important consequence in finding meaning and in transforming information as a dynamic process to discover a new experience that can affect individual perception16.
Pneumonia was found to be more common in boys than in girls. The reason for this incidence is based on the fact that boys are more likely to participate in activities outside of their homes, which makes them more prone to being exposed to pollution compared to girls.
Based on educational background, only 10% of the respondents had completed higher education. These data show that an individual with a 12-year educational background tends to need more health information, particularly that related to healthy behavior for taking care of under-age-5 children. This finding explains that an individual’s knowledge might be affected by his/her educational background15.
The majority of the respondents in the intervention and control groups had 2-4 children. It showed that the number of children could affect families’ ability to take care of their children. Having a large number of children in a family tends to cause the parents’ concentration to be divided, so the children end up getting less attention. As a result, the children become sick and even require hospitalization.
It is apparent from this study that mothers are in a productive age group that tends to have more motivation and curiosity. These data can be seen as indicating a good opportunity to motivate mothers to join education programs; thus, the goals of health promotion regarding their children’s conditions can be achieved optimally. A high degree of curiosity, explained as an example of internal motivation, might be a strong influence, as it comes from within18.
According to the bivariate analysis, the intervention of the FEM through family education has an impact on making families become empowered. A significant difference can be seen between the two groups related to the satisfaction score. These results also show that health care services, particularly nursing care, have quite similar patterns in these three district hospitals.Education, as a part of family empowerment intervention, is believed to be able to improve families’ knowledge. The improvement of knowledge therefore empowers families to take care of their children. To become empowered, individuals need the type of apprehension that will build their confidence to do things in accordance with their role as a parent during their children’s hospitalization19. Confidence can be built by practicing frequently, particularly regarding how to take care of children12.
Nursing care intervention might be related to satisfaction20. The satisfaction of families dealing with the hospitalization of their children can be derived from supportive behavior from health care teams, including not being threatening, providing information about the patient’s medical condition, and involving the family in decision-making.
Length of stay is believed to be one of the most significant indicators of the health services quality, as it can have a huge impact on families’ economic statuses. From this study, it can be found that FEM intervention has a significantly positive correlation with length of stay, as the length of stay difference between both groups was almost one day. However, the limitation of the study was the time difficulty in conducting the empowerment intervention. In conclusion, FEM intervention has a positive impact on families, as it could increase both the satisfaction and empowerment of the family. Other important indicator of the success of this FEM is its ability to decrease the length of stay of the patients21.
