






TB is one of the most deathly infections worldwide, affecting disproportionally people living with HIV (PLHIV). Furthermore, HIV co-infection is related to worse outcomes for TB patients, including lower treatment success.
MethodsUsing surveillance records of all TB cases notified in Barcelona city from 2001 to 2021, we analyzed TB treatment success according to HIV status. Additionally, we explored potential social and health related and factors associated to unsuccessful treatment in PLHIV, using multiple regression analyses.
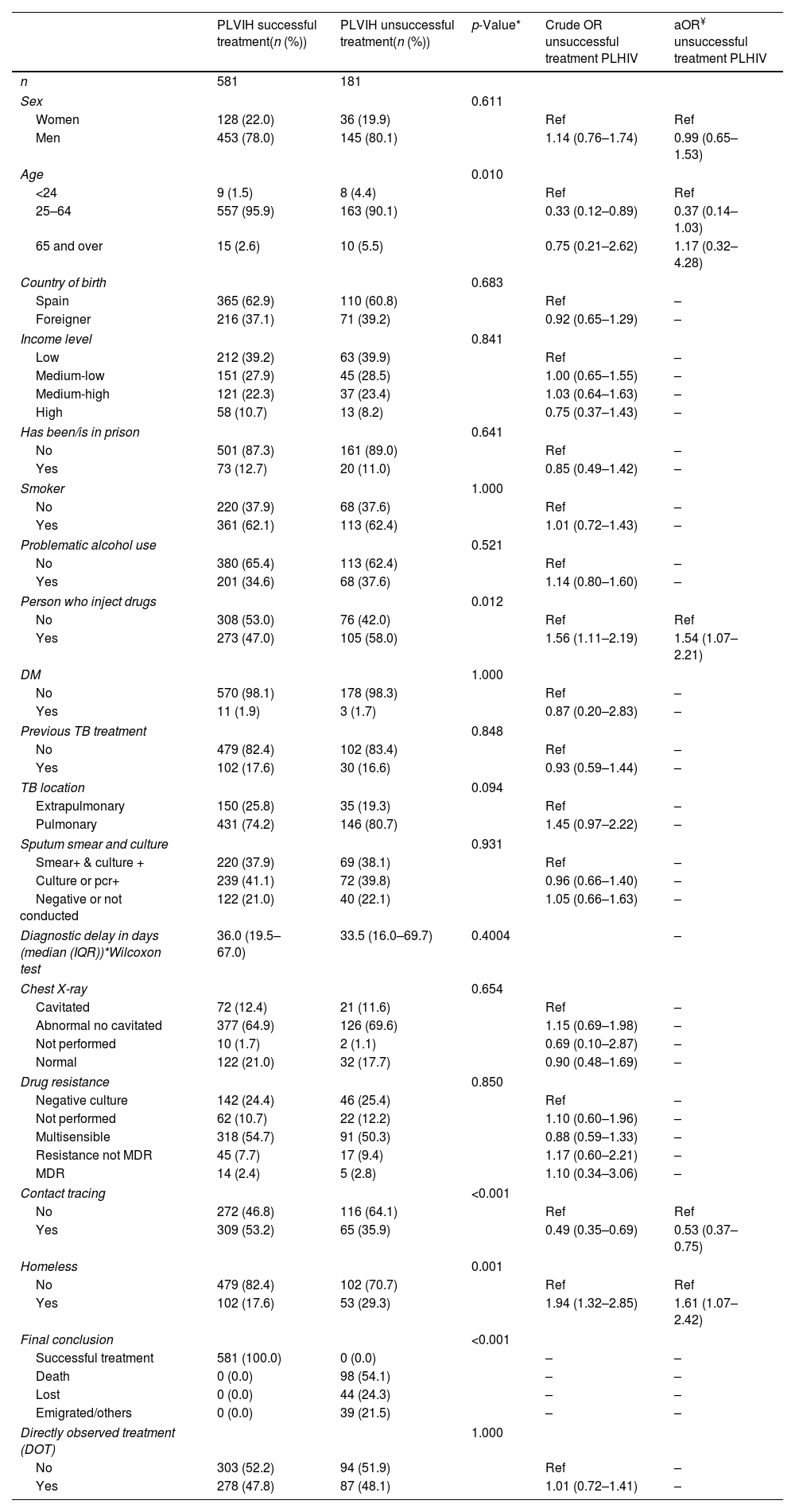
ResultsOut of the 8406 new TB cases diagnosed during the study period, 9% were co-infected with HIV. According to our regression models, PLHIV were more frequently men, users of injected drugs (aOR=45.81; 95% CI (33.10–64.26)), had previously been treated for TB (aOR=1.77; 95% CI (1.30–2.40)) and had a lower rate of contact tracing (aOR=0.51; 95% CI (0.40–0.64)). Among PLHIV, unsuccessful treatment was related to the use of injected drugs and homelessness, but it was lower for those who had undergone contact tracing.
ConclusionPLHIV have higher odds of unsuccessful TB treatment, especially those who are homeless and use injected drugs. Contact tracing improved treatment success, calling for further efforts and resources to correctly follow-up on these patients, with the goal of increasing treatment success.
La tuberculosis (TB) es una de las infecciones más mortales en todo el mundo, afectando de manera desproporcionada a las personas que viven con VIH (PVVIH). Además, la coinfección por VIH está relacionada con peores resultados para los pacientes con TB, incluyendo una menor tasa de éxito en el tratamiento.
MétodosUtilizando registros de vigilancia de todos los casos de TB notificados en la ciudad de Barcelona desde 2001 hasta 2021, analizamos el éxito del tratamiento de TB según el estado de VIH. Adicionalmente, exploramos factores sociales y relacionados con la salud asociados al tratamiento no exitoso en PVVIH, utilizando análisis de regresión múltiple.
ResultadosDe los 8,406 nuevos casos de TB diagnosticados durante el periodo del estudio, el 9% estaban coinfectados con VIH. Según nuestros modelos de regresión, las PVVIH eran más frecuentemente hombres, usuarios de drogas inyectadas (aOR=45.81; 95% IC (33.10-64.26)), habían sido tratados previamente por TB (aOR=1.77; 95% CI (1.30-2.40)) y tenían una tasa de rastreo de contactos más baja (aOR=0.51; 95% CI (0.40-0.64)). Entre las PVVIH, el tratamiento no exitoso estaba relacionado con el uso de drogas inyectadas y la falta de hogar, pero era menor para aquellos que habían sido objeto de rastreo de contactos.
ConclusiónLas PVVIH tienen mayores probabilidades de un tratamiento no exitoso de TB, especialmente aquellos que son personas sin hogar y que usan drogas inyectadas. El rastreo de contactos mejoró el éxito del tratamiento, lo que requiere más esfuerzos y recursos para dar un seguimiento adecuado a estos pacientes, con el objetivo de aumentar el éxito en el tratamiento.
Article
Socio de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica
![]()
Para acceder a la revista
Es necesario que lo haga desde la zona privada de la web de la SEIMC, clique aquí
Para realizar los cursos formativos
La actividad estará abierta para socios de la SEIMC. IMPORTANTE, recuerde que requiere registro previo gratuito. Empezar aquí
