





To correctly interpret the serological markers of Lyme disease, it is very important to determine the region's infection rate. The aim of this study was to ascertain the prevalence of specific antibodies against Borrelia burgdorferi in a rural district in northern Spain.
MethodsThe presence of IgG antibodies against B. burgdorferi was determined by qualitative enzyme immunoassay in the serum of 1432 people divided into 3 groups: 316 blood donors, 432 individuals who attended the hospital without infection and 684 for whom Lyme serology testing was specifically requested as part of a differential diagnosis. In the latter group, the presence or absence of an occupational risk factor was recorded.
ResultsAntibodies against B. burgdorferi were detected in 189 individuals (13.2%), 16 (5.1%) in the blood donors group, 62 (14.4%) in subjects who attended hospital without infection and 111 (16.2%) in subjects in whom a differential diagnosis of Lyme disease was requested (p<0.0001). In subjects with an occupational risk factor, the prevalence was 23.5%, peaking at 45.8% in men over 65 years.
ConclusionOur study showed a high prevalence of antibodies against B. burgdorferi and higher than that seen in other areas with similar characteristics in Spain. However, our results are similar to those published from other European regions. The prevalence in the blood donors group was lower than that observed in the other groups. Older age, the male gender and occupational risks were associated with a higher prevalence of Lyme disease.
Para la correcta interpretación de los marcadores serológicos de la enfermedad de Lyme es muy importante conocer la tasa de infección en el entorno. El objetivo de este estudio fue conocer la prevalencia de anticuerpos específicos frente a Borrelia burgdorferi en una comarca rural del norte de España.
MetodosSe investigó la presencia de anticuerpos IgG frente a B. burgdorferi mediante un método inmunoenzimático cualitativo en el suero de 1.432 personas divididas en 3grupos: 316 donantes de sangre, 432 individuos que acudieron al hospital sin causa infecciosa y 684 a los que se solicitó una serología de Lyme como parte del diagnóstico diferencial. En estos últimos se registró la presencia o ausencia de factor de riesgo ocupacional.
ResultadosSe detectaron anticuerpos frente a B. burgdorferi en 189 (13,2%) individuos: 16 (5,1%) donantes de sangre, 62 (14,4%) en personas que acudían al hospital sin causa infecciosa y 111 (16,2%) en personas con diagnóstico diferencial de enfermedad de Lyme (p<0,0001). En las personas con factor de riesgo ocupacional, la prevalencia fue del 23,5%, cifra que llegó al 45,8% en hombres mayores de 65 años.
ConclusionesLa prevalencia en este estudio es alta y superior a zonas con características similares de nuestro país, pero está en la media de lo publicado en otras regiones europeas. La prevalencia en donantes de sangre es menor que en los otros grupos estudiados. La edad avanzada, el sexo masculino y las prácticas de riesgo ocupacional se relacionan con una mayor prevalencia de enfermedad de Lyme.
Lyme disease is caused by the spirochete Borrelia burgdorferi sensu lato, which is transmitted to humans by the bite of ticks, mainly of the genus Ixodes. The most characteristic clinical manifestation of Lyme disease is migratory erythema, a skin lesion that normally occurs at the site of inoculation and resolves spontaneously. Without antibiotic treatment, the bacteria can reach other tissues and organs such as the heart, joints, nervous system and skin, and cause serious clinical manifestations.1 The spread of the bacteria to these places occurs mainly via the hematogenous route. Some studies have shown the presence of spirochetes in blood in patients with migratory erythema.2
Lyme disease is diagnosed in most laboratories by detecting specific antibodies. The high seroprevalence in some geographic regions complicates the interpretation of microbiological results, since individuals may present IgG antibodies that do not discriminate between active infection or resolved infection. On the other hand, the detection of IgM is only useful in the first months after infection and can cause confusion due to the numerous false positives and cross reactions.
Therefore, for the correct diagnosis of Lyme disease it is of great interest to know the infection rate by this microorganism in each community.
The objective of this work was to know the prevalence of specific antibodies against B. burgdorferi in a rural region of northern Spain in three populations with different exposures to the bacterial transmission vector.
MethodsDuring 2014 an antibody detection study against B. burgdorferi was conducted in health area II of the Principality of Asturias, a rural area located in the south west, with a population of 25,851 people over 16 years3 distributed across 5 council districts.
Some 1432 individuals were included in the study, with an age range between 16 and 93 years (mean age 52.8±6.5 years), of whom 656 were women (mean age 52±16.7 years) and 776 men (mean age 54±16.3 years).
The studied population was classified in three groups:
Group 1 (blood donors): 316 people who came to donate blood to any of the mobile donation units located in the area, who voluntarily agreed to participate in the study.
Group 2: 432 patients who went to one of the health centres in the health area with a process unrelated to an infectious cause and who had a serum sample ordered for biochemistry studies.
Group 3: 684 patients who went to the Carmen and Severo Ochoa Hospital or one of the health centres in the health area and for whom Lyme disease serology was ordered as part of the differential diagnosis of their disease. In this third group, the presence or absence of occupational risk factors was recorded and individuals were classified into 2 groups: 3a those without risk factor and 3b those that presented said risk factor.
The epidemiological characteristics of the people included in the study are shown in Table 1.
Characteristics of the population studied.
| Group | n | MA±SD [range] | Women | MA±SD [range] | Men | MA±SD [range] |
|---|---|---|---|---|---|---|
| Group 1 | 316 | 46±8.5 [18–70] | 131 | 45±11.8 [22–69] | 185 | 46±10.3 [18–70] |
| Group 2 | 432 | 54±14.1 [16–90] | 222 | 52±18.6 [16–90] | 210 | 55±16.6 [16–88] |
| Group 3 | 684 | 55±16.9 [16–93] | 303 | 56±16.3 [16–93] | 381 | 56±17.2 [16–93] |
| 3a (no ORF) | 420 | 52±17 [16–91] | 177 | 50±17 [16–91] | 243 | 54±16.8 [16–90] |
| 3b (ORF) | 264 | 59±15.8 [22–93] | 126 | 58±14 [31–91] | 138 | 60±17.3 [22–93] |
SD: standard deviation; MA: mean age; ORF: occupational risk factor.
The individuals studied were stratified in three age ranges: 16–45, 45–65 and over 65 years, for improved data analysis.
Blood samples were taken by venous puncture and processed according to the usual protocols. The serum was separated by centrifugation and stored at 4°C until processing. The determination of IgG antibodies against B. burgdorferi was done using an automated qualitative test (Vidas, bioMerieux) following the manufacturer's instructions for the development of the technique and the interpretation of the results.
Samples with positive or uncertain results were confirmed by immunoblot (Borrelia IgG IgM EcoLine, Sekisui Diagnostics).
The statistical analysis of the data obtained was prepared using the GraphPadInStat computer programme (version V2.04a). Student's t was used for continuous variables and the χ2 test or Fisher's exact test for discrete variables. A result was considered significant with p<0.05.
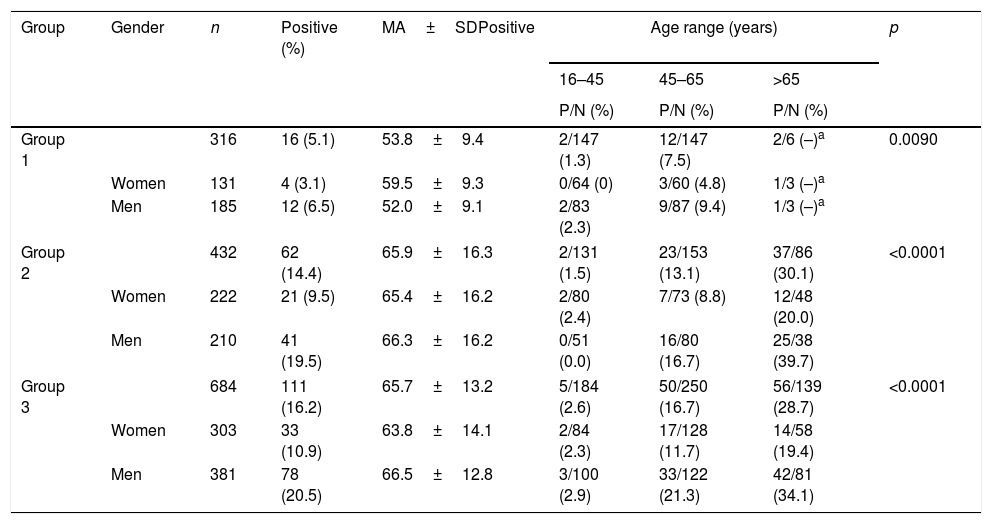
ResultsIgG antibodies against B.burgdorferi were detected in 189 (13.2%) individuals: 16 (5.1%) donors, 62 (14.4%) from group 2 and 111 (16.2%) from group 3 (p<0.0001). The most relevant results of the study are shown in Table 2.
Rate of individuals with antibodies against Borrelia burgdorferi by age and sex in each study group.
| Group | Gender | n | Positive (%) | MA±SDPositive | Age range (years) | p | ||
|---|---|---|---|---|---|---|---|---|
| 16–45 | 45–65 | >65 | ||||||
| P/N (%) | P/N (%) | P/N (%) | ||||||
| Group 1 | 316 | 16 (5.1) | 53.8±9.4 | 2/147 (1.3) | 12/147 (7.5) | 2/6 (–)a | 0.0090 | |
| Women | 131 | 4 (3.1) | 59.5±9.3 | 0/64 (0) | 3/60 (4.8) | 1/3 (–)a | ||
| Men | 185 | 12 (6.5) | 52.0±9.1 | 2/83 (2.3) | 9/87 (9.4) | 1/3 (–)a | ||
| Group 2 | 432 | 62 (14.4) | 65.9±16.3 | 2/131 (1.5) | 23/153 (13.1) | 37/86 (30.1) | <0.0001 | |
| Women | 222 | 21 (9.5) | 65.4±16.2 | 2/80 (2.4) | 7/73 (8.8) | 12/48 (20.0) | ||
| Men | 210 | 41 (19.5) | 66.3±16.2 | 0/51 (0.0) | 16/80 (16.7) | 25/38 (39.7) | ||
| Group 3 | 684 | 111 (16.2) | 65.7±13.2 | 5/184 (2.6) | 50/250 (16.7) | 56/139 (28.7) | <0.0001 | |
| Women | 303 | 33 (10.9) | 63.8±14.1 | 2/84 (2.3) | 17/128 (11.7) | 14/58 (19.4) | ||
| Men | 381 | 78 (20.5) | 66.5±12.8 | 3/100 (2.9) | 33/122 (21.3) | 42/81 (34.1) | ||
SD: standard deviation; MA: mean age; P/N: positive/negative.
In the donor group, antibodies against B.burgdorferi were detected in 4 women (3.1%) and in 12 men (6.5%) (p=0.17); in contrast, in group 2 the prevalence was 9.5% in women and 19.5% in men (p=0.044) and in group 3 it was 10.9% in women and 20.5% in men (p=0.0007).
In addition, in the donor group, the average age of women with antibodies was 59.5±9.3 years and in men it was 52±9.1 years (p<0.0001). In group 2, the age of women with antibodies was 65.4±16.2 and in men it was 66.3±16.2 years (p=0.83), while in group 3 it was 63.8±14.1 in women and 66.5±12.8 in men (p=0.009).
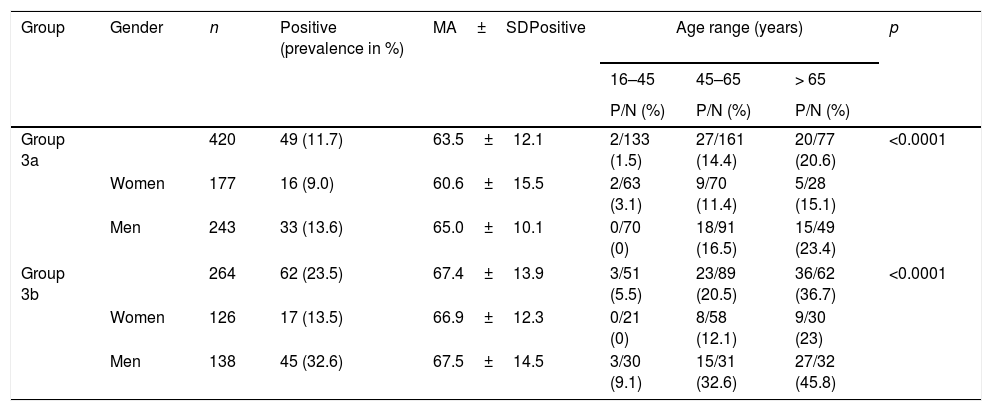
In group 3a, the prevalence was 9% in women and 13.6% in men (p=0.15) and the mean age of positive subjects was 60.6 years among the former and 65 for the latter (p=0.0005). In group 3b, the prevalence in women was 13.5% and in men it was 32.6% (p=0.00048). The mean age of positive subjects was 66.9 and 67.5 years, respectively (p=0.71).
The prevalence of 9.1% in young men (16-45 years) in group 3b is noteworthy.
Table 3 shows the data of individuals in group 3 according to the risk of contact with the vector due to their occupation (3b) or lack of risk (3a).
Results from the group 3 population by presence of occupational risk factors (3b) or no risk (3a).
| Group | Gender | n | Positive (prevalence in %) | MA±SDPositive | Age range (years) | p | ||
|---|---|---|---|---|---|---|---|---|
| 16–45 | 45–65 | > 65 | ||||||
| P/N (%) | P/N (%) | P/N (%) | ||||||
| Group 3a | 420 | 49 (11.7) | 63.5±12.1 | 2/133 (1.5) | 27/161 (14.4) | 20/77 (20.6) | <0.0001 | |
| Women | 177 | 16 (9.0) | 60.6±15.5 | 2/63 (3.1) | 9/70 (11.4) | 5/28 (15.1) | ||
| Men | 243 | 33 (13.6) | 65.0±10.1 | 0/70 (0) | 18/91 (16.5) | 15/49 (23.4) | ||
| Group 3b | 264 | 62 (23.5) | 67.4±13.9 | 3/51 (5.5) | 23/89 (20.5) | 36/62 (36.7) | <0.0001 | |
| Women | 126 | 17 (13.5) | 66.9±12.3 | 0/21 (0) | 8/58 (12.1) | 9/30 (23) | ||
| Men | 138 | 45 (32.6) | 67.5±14.5 | 3/30 (9.1) | 15/31 (32.6) | 27/32 (45.8) | ||
SD: standard deviation; MA: mean age; P/N: positive/negative.
The south western part of Asturias is a wooded and humid area that is 85% forested, where ticks abound.4 Most of them are of the genus Ixodes and it has been shown that many are carriers of the bacteria B. burgdorferi.5 The autonomous community of the Principality of Asturias is considered an area with endemic Lyme borreliosis.6 In a previous study of this area of Asturias7 Lyme disease incidence rates of 130 cases per 100,000 inhabitants were described. In addition, area II is the Asturian health area with the highest number of cases hospitalized for borreliosis.8 However, the actual extent of the infection is unknown at present In the present work, a significant number of patients have been analysed and an effort has been made to define different groups that allow a better evaluation of the status of infection due to B. burgdorferi.
The seroprevalence of 13.2% found is similar to that reported in Soria (13.1%)9 and exceeds that found in other areas of the country such as 4.4% in Navarra10 or 3.45% in Madrid.11
These low levels of infection are similar to those found in the blood donor group (5.1%). In Spain no seroprevalence studies of infection due to B. burgdorferi in donors have been published; studies in other countries report similar percentages: 4.2% in Scotland12 and 4.3% in Romania.13 These data may vary within a single country. Thus, in the north of Norway the prevalence is 0.48% and in the south 9.25%.14 In Belgium there are no differences between donors in rural and urban areas, with prevalences of 2.6 and 2.9%.15 Despite these percentages and the fact that a hematogenous spread of the bacteria occurs in the early stages of Lyme disease, no cases of transmission of Lyme disease through blood transfusions have been reported to date.16 The low seroprevalence of B. burgdorferi found in donors in this study may be due to their age, since only 8 donors were older than 65 years (the age group with the highest prevalence).
In the donor group there are no significant differences by sex, although it is observed that women become infected at a later age.
In the other groups analysed (those who went to the hospital without an infectious cause and the group that had symptoms compatible with Lyme disease), the detection of antibodies against the bacteria exceeds 14%. The high seroprevalence of Lyme disease makes the interpretation of serology results difficult, since we find patients with specific antibodies against B. burgdorferi with nonspecific symptoms in which we cannot specify whether it is a resolved infection or an active infection.
Previously it was noted that this prevalence was higher than areas with similar characteristics in our country, but it is average based on figures published in other European regions. Thus, in Germany a prevalence of 9.40% has been reported, in Belgium it is of the order of 21–23% and in Slovakia 25.3%, although it should be taken into account that this last study was conducted in people at risk due to their work or activity.17–19
It is logical to think that those populations in contact with a forested area and with occupations in that area would a higher infection rate. This is the case in this study, since within group 3 it was found that those people with a higher risk of tick bites due to their occupation and, therefore, with a higher risk of exposure to the vector, reached detection rates of antibodies against B. burgdorferi of up to 45% in older individuals. Moreover, in this group, 3b, the youngest had already reached 9% antibody rates. In Spain there are similar jobs in which there is a greater seroprevalence in people at risk due to their profession or geographical area of residence, with prevalences reaching up to 38% in farmers and forest rangers in La Rioja.20
The increase in the infection rate is closely related to the increased exposure to the vector. On this point, in addition to occupational risk, age may be another variable that increases that exposure.
This work shows a significant increase in the prevalence of antibodies with the patient's age and percentages close to 30% are reached in people over 65 years of age. This contrasts with other works10,11,21 in which no significant differences are found; however, the European studies mentioned in Germany and Belgium also show an increase in prevalence with age, reaching levels of 30% above the age of 65.
As in other studies, a greater seroprevalence is observed in men, especially in those over 45 years.17 This figure seems to be related to men's greater participation in outdoor activities.
A large part of the requests made to microbiology laboratories do not meet case definitions of Lyme disease. Thus, in a study in the Netherlands, only 9% of the patients studied met the clinical criteria.22 The diagnosis must be made in the presence of an adequate epidemiological environment and with the possibility of a tick bite.23 It is noteworthy that the prevalence among people in whom the reason for consultation was not related to infectious disease (group 2) is similar to the prevalence in those with a clinical picture compatible with Lyme disease (group 3). This can be explained by the broad spectrum of clinical manifestations produced by B. burgdorferi. It seems clear that the most important factor when deciding to request a Lyme disease study is the presence of a risk factor, especially in individuals under 65 years of age.
In summary, occupational risk practices in forested areas are related to a higher prevalence of Lyme disease. To date, men have been the most affected by this disease because they were engaged first with agricultural activity and in more forested areas and further away from urban areas. The change in work activity, with less agricultural activity, could lead to a decrease in this prevalence; however, the increase of outdoor recreational activities, involving men and women and at younger and younger ages, may counteract this decline. Studies in the coming years will indicate whether or not this change in activity reduces prevalence.
FundingThe study does not have a source of funding.
Conflicts of interestThe authors have no conflicts of interest to declare.
To Sofie Bosma for her collaboration in the translation of the text into English.
Please cite this article as: Barreiro-Hurlé L, Melón-García S, Seco-Bernal C, Muñoz-Turrillas C, Rodríguez-Pérez M. Seroprevalencia de enfermedad de Lyme en el suroccidente de Asturias. Enferm Infecc Microbiol Clin. 2020;38:155–158.
