




There is an alarming increase in the number of patients with type 2 diabetes mellitus (T2DM). This increase is causing personal, family, social, economic, and political problems. The aim of this article is to ascertain the side effects of treatments, the complications suffered by patients, and the practices to improve management of this disease from the viewpoint of the experience of patients and health care management.
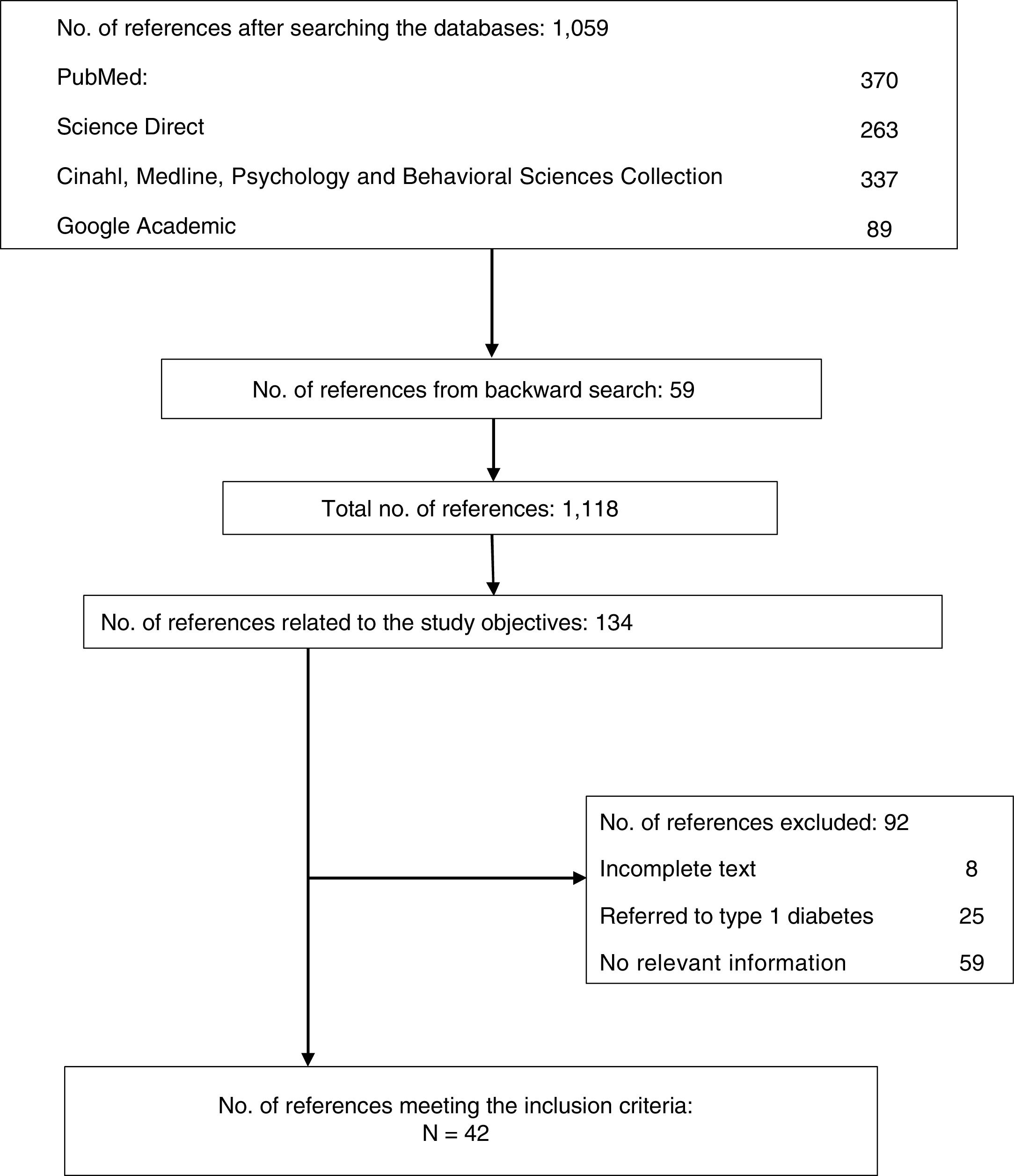
Material and methodsA narrative review was conducted of studies on T2DM published in English and Spanish indexed in PubMed, Science Direct, Cinahl, MedLine, Psychology and Behavioral Sciences Collection, and Google academic. A total of 1118 articles were found, 42 of which referred to the objectives of the review and met the inclusion criteria.
ResultsThe side effects and complications experienced by patients and their perception that they do not receive adequate information, together with poor satisfaction, lead to non-adherence to treatment, which impairs patient health and increases health care costs. The proposals in the reviewed studies guide the actions to improve treatment adherence and, thus, quality of life of patients, to decrease side effects and mortality and, therefore, the costs associated to T2DM through: 1) quick and easy access to medical care, 2) quality health education, and 3) participation of patients in the decisions about their treatment and in self-management of their disease to make minimum changes in their lifestyles.
El número de enfermos de diabetes Tipo 2 está creciendo de forma alarmante. Este aumento está causando problemas personales, familiares, sociales, económicos y políticos. El objetivo de este artículo es conocer los efectos secundarios de los tratamientos, complicaciones que sufren los pacientes y prácticas para mejorar la gestión de esta enfermedad desde el punto de vista de la vivencia del individuo y de la gestión de la atención sanitaria.
Material y métodosSe realizó una revisión narrativa de los estudios sobre la diabetes Tipo 2 publicados en inglés y en español indexados en PubMed, Science Direct, Cinahl, MedLine, Psychology and Behavioral Sciences Collection y Google académico. Se identificaron 1.118 artículos, de los cuales 42 se referían a los objetivos de la revisión y cumplían los criterios de inclusión.
ResultadosLos efectos secundarios y complicaciones que sufren los pacientes y la percepción de recibir escasa información, repercuten en una falta de adherencia al tratamiento. Esto implica una disminución de la salud de los pacientes y un aumento de los costes sanitarios. Las propuestas de los estudios revisados encaminan las acciones para mejorar la adherencia al tratamiento y así mejorar la calidad de vida del paciente, disminuir los efectos secundarios, mortalidad y, por tanto, los costes asociados a esta enfermedad a través de: 1) tener un acceso a la atención médica rápida y fácil, 2) una educación de calidad y 3) permitir que el paciente participe en las decisiones de su tratamiento y autogestione su enfermedad para realizar los mínimos cambio en su estilo de vida.
According to the World Health Organization (WHO) in 2014, a full 9 % of all adults in the world had diabetes. Far from decreasing, this disease is increasing at a worrying rate.1 The WHO predicts that diabetes will be the seventh most common cause of death in 2030.2 In 2012, a total of 1.5 million people died from the disease.2 Among the more developed countries, Spain has one of the highest increments of diabetes mellitus.3 In this country, 13.8 % of the population has type 2 diabetes, i.e., 5.3 million Spaniards over 18 years of age. An increase in the disease has been evidenced in recent decades due to a rise in the number of obese and sedentary individuals and the presence of a carbohydrate-rich diet.4,5
Diabetes is therefore considered to be one of the main public health problems worldwide.6,7 Managing the disease on a personal, family, social, economic and political level has become a genuine challenge for individuals and governments.8 On a personal level, the presence of diabetes requires a constant physical and emotional effort that appears to be one of major causes of patient non-adherence to treatment.9,10 At an economic level, in the United States, type 2 diabetes accounted for more than 10 % of the total healthcare expenditure in 2007. On the other hand, loss of productivity due to sick leave or reduced work performance, accidents or disability constitutes an added cost.6,7,11
In order to propose measures to palliate the consequences and improve the management of the disease, we need to know how the treatments affect patients, what the most common complications are, and what improvements are being implemented. No reviews covering these points are available to date. The objectives of the present study were to obtain information on type 2 diabetes referred to: a) the consequences of current diabetes management; and b) current practices to improve management of the situation.
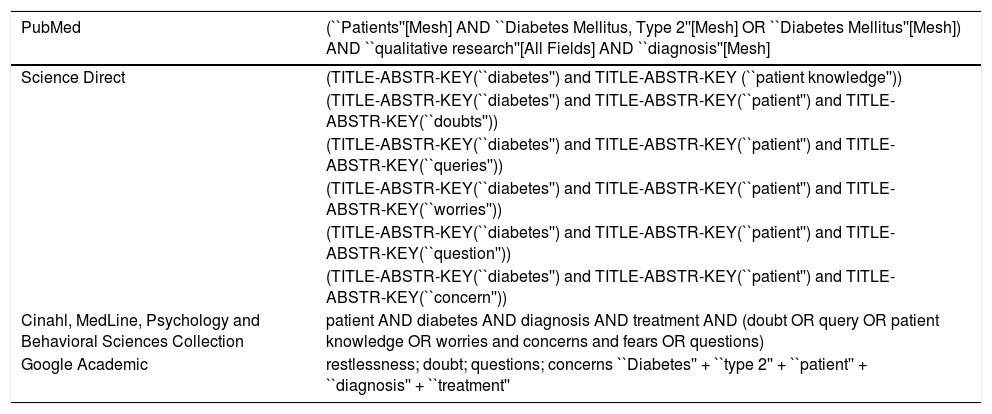
Material and methodsA narrative review of the scientific literature was made following the criteria of the PRISMA statement12 regarding eligibility criteria, information sources, searches, study selection, data compilation and data listing. The following databases were searched: PubMed, Science Direct, Cinahl, Medline, Psychology and Behavioral Sciences Collection, and Google Academic. The searches were performed using the same terms, but adapted to the concrete requirements of each database (Table 1). In addition, publications were obtained by backward search considering the articles retrieved.
Search strategies in the different databases according to the PRISMA statement.
| PubMed | (``Patients''[Mesh] AND ``Diabetes Mellitus, Type 2''[Mesh] OR ``Diabetes Mellitus''[Mesh]) AND ``qualitative research''[All Fields] AND ``diagnosis''[Mesh] |
|---|---|
| Science Direct | (TITLE-ABSTR-KEY(``diabetes'') and TITLE-ABSTR-KEY (``patient knowledge'')) |
| (TITLE-ABSTR-KEY(``diabetes'') and TITLE-ABSTR-KEY(``patient'') and TITLE-ABSTR-KEY(``doubts'')) | |
| (TITLE-ABSTR-KEY(``diabetes'') and TITLE-ABSTR-KEY(``patient'') and TITLE-ABSTR-KEY(``queries'')) | |
| (TITLE-ABSTR-KEY(``diabetes'') and TITLE-ABSTR-KEY(``patient'') and TITLE-ABSTR-KEY(``worries'')) | |
| (TITLE-ABSTR-KEY(``diabetes'') and TITLE-ABSTR-KEY(``patient'') and TITLE-ABSTR-KEY(``question'')) | |
| (TITLE-ABSTR-KEY(``diabetes'') and TITLE-ABSTR-KEY(``patient'') and TITLE-ABSTR-KEY(``concern'')) | |
| Cinahl, MedLine, Psychology and Behavioral Sciences Collection | patient AND diabetes AND diagnosis AND treatment AND (doubt OR query OR patient knowledge OR worries and concerns and fears OR questions) |
| Google Academic | restlessness; doubt; questions; concerns ``Diabetes'' + ``type 2'' + ``patient'' + ``diagnosis'' + ``treatment'' |
The study inclusion criteria were: a) publications addressing the issues raised in the objectives of this study; b) publications in English or Spanish, c) studies conducted in Western cultural contexts; and d) publications referred to adult patients with type 2 diabetes.
Of the 1059 articles retrieved, a first screening by title and abstract was performed to select those articles that were related to the study objectives. In addition, the reference lists of the selected articles were reviewed with a view to selecting further publications related to the study objectives. This resulted in the addition of a further 59 articles. Of all the initial references (n = 1118), we evaluated those related to the study objectives and which moreover met the established inclusion criteria, with the final identification of 42 publications. These articles were filed in electronic format. Fig. 1 shows the flowchart of the search process. Table 2 shows the characteristics of the articles included in the study, such as design, patient type, study setting and sample size.

Summary of the reviewed articles (n = 42).
| Authors | Objective | Methodological design | Study setting | Type of participant | Sample size | Age | Validity/reliability |
|---|---|---|---|---|---|---|---|
| Barlow et al., 2002 | Provide an overview of the self-management approaches for people with chronic conditions | Qualitative observational study | United Kingdom | Patients with chronic diseases | N/A | >75a | No information |
| Beverly et al., 2011 | Explore physician awareness and the responses to the social and emotional difficulties of T2DM patients | Phenomenological qualitative study | Boston primary and specialized care | Intentional sampling of endocrinologists and general practitioners with at least 5 % of their practice dedicated to T2DM patients | n = 19 | N/A | Triangulation of data sources, methods and investigators |
| Semi-structured interviews applying thematic analysis | |||||||
| Bolaños and Sarría-Santamera, 2003 | Investigate the perception which people with T2DM have about the disease and about the relationship with the primary care healthcare professionals | Phenomenological qualitative study | Centro de salud barrio del Pilar (Madrid) | Adults with T2DM | n = 15 | From 45 to 65 years | Decision making process screening |
| Open interviews | |||||||
| Bonal and Cascaret, 2009 | Review of the concept of self-management as a cornerstone in the care of patients with chronic diseases, in view of confusion and indistinct reference to the term as self-care, self-control, self-handling, self-treatment or self-help. Assess aspects related to the interchangeable phrases: chronic patient education, self-management education, and self-management support | Descriptive literature review | N/A | N/A | N/A | N/A | N/A |
| Cabrera et al., 2009 | Know the lifestyle of people with diabetes in the Canary Islands and their adherence to treatment, as well as the prevalence of unknown T2DM | A cross-sectional, analytical, quantitative observational study | Canary Islands | General population selected in the CDC cohort (Cardiovascular, Diabetes, Cancer) | n = 6729 | From 18 to 75 years | No information |
| Cano et al., 2013 | Describe the prevalence of blood glucose self-monitoring in subjects with T2DM not treated with insulin. Analyse factors associated with its use | A cross-sectional, analytical, quantitative observational study | 83 primary care consultations in the Valencian Community (Spain) | Diagnosed with T2DM before 2009, seen in the general practice clinic for any reason | n = 573 | >30a | No information |
| Cervantes-Villagrana and Presno-Bernal, 2013 | Review physiological processes that are altered in diabetes | Descriptive literature review | N/A | N/A | N/A | N/A | N/A |
| D'Eramo-Melkus and Demas, 1989 | Examine patient and physician perceptions of the diabetes treatment goals agreed between them | Cross-sectional, quantitative descriptive study | Health system in the United States | Patients with obesity who do not receive insulin therapy and are under medical control | n = 54 | From 21 to 65 years | No information |
| Survey | |||||||
| Diego and Amado-Guirado, 2015 | Review of the role of the patient and healthcare professionals in managing the disease and its treatments | Narrative literature review | N/A | N/A | N/A | N/A | N/A |
| Dilla et al., 2009 | Analyse the clinical and economic consequences of non-compliance and its causes | Narrative literature review | N/A | N/A | N/A | N/A | N/A |
| Identify strategies for improvement | |||||||
| Durand et al., 2016 | Develop and test the usefulness, acceptability and accessibility of a decision-making aid with pictorial/graphic material aimed at women of low socioeconomic level diagnosed with early-stage breast cancer | Qualitative study with theoretical sampling | Phases 1 and 2: Upper Valley in New Hampshire (USA), rural and urban area | Phase 1: clinical and academic | Phase 1: 18 academicians | Phase 2: >40a | Reliability: 2 investigators independently coded transcripts and discussed discrepancies among the evaluators |
| Phases 1 and 2: participatory research with "thinking out loud" protocols | Phase 3: Chelsea (Massachusetts, USA), rural area | Phase 2: women of low economic status regardless of breast cancer history | Phase 2: 23 | F3: mean 56.8 years | |||
| Phase 3: semi-structured interviews | Phase 3: women of low economic status and a recent diagnosis of breast cancer | Phase 3: 10 | |||||
| Eborall et al., 2007 | Study of factors that contribute to anxiety during the diabetes screening process and analyse expectations and reactions to the screening process among patients with positive, negative and intermediate results | Qualitative study: longitudinal prospective design | 7 primary care centres included in the ADDITION trial (Cambridge) in Eastern England | Patients participating in different stages of a T2DM detection program | n = 23 | From 50 to 69 years | No information |
| Interview | |||||||
| Elwyn et al., 2013 | Describe the exploratory use of short-term decision support tools for patients, called "option networks" | A cross-sectional, descriptive, qualitative observational study | N/A | N/A | N/A | N/A | N/A |
| Study using projected option networks and interviews with clinical teams | |||||||
| Eroğlu et al., 2014 | Define the adaptive response of diabetic patients to their condition and identify the topics where educational intervention is needed according to the patients | Cross-sectional, quantitative descriptive study | State hospitals, polyclinics with endocrinology and internal medicine clinics in Turkey | Volunteers with diabetes attending an educational program in diabetes. The majority were women, married, with primary schooling, housewives | n = 170 | From 53 to 70 years | No information |
| Questionnaire administered in face-to-face interviews | |||||||
| Formosa et al., 2012 | Challenge current approaches to education on diabetes and highlight how education might be extended to produce more effective outcomes | Evaluative literature review | N/A | N/A | N/A | N/A | N/A |
| Funnell, 2006 | Identify attitudes, wants and needs of people with diabetes and physicians to improve disease care | Descriptive literature review | 13 countries | 250 general practitioners, specialists and nurses | n = 750 | No information | |
| 500 patients with diabetes | |||||||
| Gil-Guillén et al., 2012 | Analyse strategies to improve compliance with prescribed therapies in diabetes | Descriptive literature review | N/A | N/A | N/A | N/A | N/A |
| Gil-Velázquez et al., 2013 | Standardize the process of care provided in medical units for T2DM | Descriptive literature review | Health system of Mexico | N/A | N/A | N/A | N/A |
| Hart and Collazo, 1998 | Review and analyse information on costs of diagnosis and treatment of diabetes in the world | A cross-sectional, descriptive, quantitative observational study | N/A | N/A | N/A | N/A | N/A |
| Heisler et al., 2003 | Assess whether physician-patient collaboration improves self-care by promoting greater agreement on treatments and goals | A cross-sectional, descriptive, quantitative observational study | Michigan military medical centre and university hospital | 127 pairs of patients with T2DM and their primary care physicians. People with medication and one hospital admission or 2 outpatient visits related to diabetes code | n = 127 | >30a | Affirmed validity |
| Survey | |||||||
| Hewitt et al., 2011 | Examine knowledge and management of diabetes among elderly people | Correlating, quantitative observational study | Primary care in the United Kingdom | Persons diagnosed with T2DM in the list of users of centres, and not residing in nursing homes | n = 1047 | >75a | Validated and widely used Carts index |
| Jadad et al., 2010 | General understanding of multiple chronic diseases | A cross-sectional, descriptive, qualitative observational study | Spain | Chronic patients | N/A | N/A | N/A |
| Lawton et al., 2003 | Determine the impact of intensive blood glucose control on the development of complications in patients with T2DM | Longitudinal exploratory qualitative study | Northampton General Hospital, England | Patients with T2DM | n = 10 | From 25 to 65 years | No information |
| Lecube et al., 2016 | Consolidate obesity as a disease | Qualitative clinical research study | Spain | People with obesity | Epidemiological: 21.6 % of the population | N/A | N/A |
| Ledón-Llanes, 2011 | Explore life dynamics of people with chronic diseases and understand how the role players participate in their health processes in the different spaces of social expression | Systematic review | Institutionalized health processes, primarily in urban areas | With non-transmissible chronic diseases: endocrine, oncological, cardiovascular and renal | N/A | N/A | N/A |
| Marante et al., 2011 | Identify the level of patient knowledge about aspects of diabetes education: educational level, family history of diabetes, and time since disease onset | Cross-sectional qualitative descriptive study | 3 consulting rooms in the San Felipe III neighbourhood (parish church of San Francisco), Havana (Cuba) | Patients diagnosed with DM | n = 88 | >35a | No information |
| Identify most common disease complications in the surveyed patients | |||||||
| Marrin et al., 2013 | Description of underlying principles and presentation of protocol for the development of short support tools: “Option Grid” | Explanatory qualitative observational study | Medical visits | Patients in clinic | N/A | N/A | N/A |
| Meng et al., 2017 | Estimate effects of factors related to disease treatment in patients with T2DM | Retrospective, qualitative observational study | Patient claims database | Patients with T2DM on medication | n = 141,409 | ≤18a | Validity: goodness of fit analysis, replication of model fit in validation sample |
| Mestre, 2014 | Explain the functioning, characteristics, strategies, outcomes and purpose of the Catalonia Expert Patient Program | Explanatory qualitative study: program presentation | Catalonia | Chronic patients | N/A | N/A | Affirmed validity |
| Montori et al., 2006 | Analyse applicability of the Charles et al. methodology. STDM (shared treatment decision-making) model in the context of chronic care, largely dependent on patient self-management | Systematic review and discussion | N/A | Patients with chronic diseases | N/A | N/A | N/A |
| Mosnier-Pudar et al., 2009 | Describe T2DM from the patient perspective | A cross-sectional, descriptive, quantitative observational study. | Survey institute, TNS Healthcare-Sofres | French population age ≥45 years | n = 14,201 (1092 patients with T2DM) | >45a | Affirmed validity and reliability |
| Mullan et al., 2009 | Randomized drug choice pilot study | Quantitative-qualitative observational study: surveys and video analysis | 11 primary care and family medicine centres within the Mayo Clinic Health System and Olmsted Medical Center (Southeast Minnesota) | Eligible professionals: physicians, physician assistants, and nurses dealing with diabetes. Eligible patients: adults diagnosed with T2DM >1 year and with scheduled appointment | n = 40 clinicians and 85 patients | Affirmed validity | |
| Noda-Milla et al., 2008 | Measure the level of knowledge about T2DM in patients | Qualitative observational study: individual interviews | Peru (Lima): Hospital Nacional Arzobispo Loayza and Hospital Nacional Cayetano Heredia | Patients with diabetes and aged >35 years, hospitalized due to disease decompensation | n = 31 | > 35 years. Mean = 59 | No information |
| Nicolucci et al., 2013 | Assess psychosocial outcomes in people with diabetes in different countries for comparative assessment | A survey-based, cross-sectional, quantitative descriptive study | 17 countries | Diabetics. Type 1 and 2 diabetic population | n = 8596 (1368 type 1 and 7228 type 2) | ≥30a | Validity and reliability: with experimental test and Cronbach |
| Ollero-Baturone et al., 2014 | Review the impact of chronic diseases on social determinants, way of becoming ill, models for managing chronic diseases and proposals for the future | Review/reflection article | Andalusia | N/A | N/A | ||
| Parry et al., 2004 | Examine how the diagnosis is perceived by a sample of newly diagnosed T2DM patients | Phenomenological qualitative study: interviews | Lothian (Scotland). Poor and prosperous rural and urban areas | Newly diagnosed T2DM patients: 19 women, 21 men | n = 40 | Mean = 48 years | No information |
| Peel et al., 2004 | Explore emotional reactions of patients to diagnosis, and their views on information supplied at diagnosis | Phenomenological qualitative study: interviews | Lothian (Scotland). Poor and prosperous rural and urban areas | Newly diagnosed T2DM patients: 19 women, 21 men | n = 40 | From 21 to 77 years. Mean = 48 | No information |
| Mean age: 48a | |||||||
| Pérez and Prados, 2014 | Analyse the economic burdens of chronic diseases | Cross-sectional qualitative descriptive study | N/A | Chronic disease | N/A | N/A | N/A |
| Powell et al., 2015 | Assess the new role of healthcare professionals as collaborators of patients and their relatives in diabetes management | Descriptive literature review | N/A | N/A | N/A | N/A | N/A |
| Ritholz et al., 2014 | Explore perceptions of barriers and facilitators of communication in relation to diabetes self-care during medical appointments | Phenomenological qualitative study: semi-structured guided interviews | Boston | 1) Endocrinologists and primary care physicians with at least 5 % of patients with T2DM | n = 19 physicians and 34 patients | From 30 to 70 years | Validity: triangulation of data sources, methods and investigators |
| 2) Patients with T2DM without severe mental problems or cognitive or visual impairment and HbA1c < 130 mmol/mol (14.0%) | Reliability: use of audit trail, which recorded research decisions and processes | ||||||
| Velázquez-Mendoza and Balcázar-Nava, 2012 | Analyse personal experiences and impact of the disease on different life domains in people diagnosed with T2DM | Phenomenological qualitative study: interviews | Home address | DM2 patients | n = 6 | ≥18a | No information |
| Zeballos-Palacios et al., 2014 | Describe the role of shared decision-making in chronic disease management | Descriptive literature review | Peru | N/A | N/A | N/A | N/A |
Information regarding the study objectives was compiled from each article. The data referred to each of the objectives were recorded, and we then focused on preparation and organisation of the information. The data were organized according to common topics allowing development and coherence of the retrieved information.
Specifically, information was recorded referred to the following: a) the reactions to the diagnosis: how patients perceive their quality of life with regard to the disease, both physically and emotionally; what concerns they have throughout the course of the disease; the level of patient satisfaction after the diagnosis; and b) the practices adopted to improve the current situation: types of interventions, procedures and results obtained.
ResultsConsequences derived from current diabetes managementThis section describes the results obtained from the review of studies on how patients perceive and manage their quality of life with regard to the disease, both physically and emotionally. The following 6 sections are highlighted.
Reactions to the diagnosisMost of the reviewed studies report that patients experience anxiety on receiving confirmation of the disease.13–17 Feelings of shock, guilt, anger, frustration, depression, helplessness and rejection were also reported.9,15 These reactions were due to the fact that the chronic disease was perceived as being serious, catastrophic, conflictive and threatening.9,17 Some patients expressed concern about dying in an unpleasant and dramatic manner.18 These feelings were accompanied by physical and emotional discomfort, worry and a sense of loss of control.9 This feeling of loss of control worsened in the presence of family overprotection, since the latter increased patient deficiency and limited personal autonomy — thereby limiting the chances of leading a normal life.9 Lastly, the reviewed articles revealed a strong fear and rejection of the possibility of having to be treated with insulin. This was perceived as being the last and most serious stage in the disease process.19
In other reviewed studies, the most common reaction was to minimize the importance of the problem.20 Denial is another way of coping: acting as if the disease does not exist, thinking that it will disappear, that it will have no consequences, or that it is not so serious because there are no symptoms.9
Stress and guilt associated to difficulties or reluctance to change, were related to poorer coping with the disease. In contrast, confidence, help with change, and attention to psychosocial factors would facilitate the disease coping process.20
Satisfaction with treatmentMosnier-Pudar et al. reported high treatment satisfaction (score 8/10),13 though this was not so manifest in the explanations of the patients when their opinions were explored more in depth.9,17,21 A factor found to increase satisfaction is when the physician explains the possible consequences and treatments quickly, easily, clearly and assertively so that the patients can better understand the changes to be made in their lives.17 In contrast, waiting for an appointment was problematic, particularly in those patients that perceived diabetes as being something serious.17 In the study published by Nicolucci et al.,21 approximately 40 % of the participants reported that their medication interfered with their ability to lead a normal life. On the other hand, Velázquez-Mendoza and Balcázar-Nava found that most patients admitted that they do not fully adhere to the diet instructions. Indeed, some patients viewed the diet as something that may harm them rather than be of any help.9
In terms of satisfaction with the information received, the review found that patients consider a lack of information and support by the healthcare professionals at the time of diagnosis to be a problem.14 They underscored the importance for the diabetes management plan to be consistent and realistic with their personal setting, life circumstances and abilities to find a balance between the limitations imposed by the disease and their desire to stay motivated. The most significant complaints found in the study were not having sufficiently detailed explanations about at least one aspect of the disease (85 %), the potential impact of diabetes upon health (43 %), the origin of the disease (40 %) and lifestyle changes (33 % in general, 26 % referred to information on diet and 14 % on exercise).14 In addition, the studies found continuity and the time spent with the physician to be key elements for improving patient satisfaction.17,22,23
Cost and adherence to treatmentDiabetes is one of the most expensive diseases because of its associated mortality, disability and the very important costs generated by its complications and treatments.4,7,24 The emotional and social costs of the disease are difficult to quantify, but the economic costs represent a very important burden for the different countries.24 Diabetic patients use 2–5 times more healthcare resources than the nondiabetic population.25 There is a direct relationship between non-adherence to the treatment objectives and worsening of health in these patients.24 This situation results in more visits to the outpatient clinic and emergency care, and an increase in hospital admissions. In the United States, it is estimated that incorrect medication use has a cost of about 100 billion USD a year.24
Regarding adherence, the studies reflect that approximately 50 % of the patients claim to adhere to the prescribed treatment.26,27 Stress and guilt are related to difficulties or reluctance, and therefore to reduced adherence.20 Funnell found that only 16 % of the patients reported having fully adhered to all the recommendations of the professionals.15 The physicians went even further, reporting that only 3 % of the patients were fully adherent to their recommendations.15 A lack of adherence has a range of consequences, particularly of a clinical and economic nature.20 In studies of young people using insulin, adherence to therapy was found to be greater.19,28 Thirty-nine percent of the young people performed daily blood glucose tests, and 56 % did so on a weekly basis or less. Among those using insulin, the proportion and frequency of glucose testing was higher: 70 % of the people checked their blood glucose, 64 % did so about once a day, and 36 % weekly or less.28
Adherence is also related to good physician-patient communication.17,29,30 Lack of communication about emotional aspects and practical management of the disease has a negative impact upon treatment compliance. Such non-compliance is closely related to physician neglect to explain the purpose of the treatment.29,30 With a view to improving treatment adherence and compliance, Dilla et al. and Gil-Guillén et al. described different strategies, such as improved knowledge of the disease among the professionals and the simplification of treatment in order to minimize the negative effects and costs for the patient, and thus promote changes in beliefs.24,31 On the part of the patient, adherence would improve if treatment were combined with other daily activities to increase emotional well-being.24,31 Lastly, family and social support is essential to secure good adherence.24,31
Common complicationsThe complications of the disease are divided into immediate (acute) complications, such as recurrent infections, depression and severe hypoglycemia, and long-term (chronic) complications9 such as macrovascular (11 %), microvascular (10 %), neuropathic (33 %), infectious (36 %) and other problems (9 %).32 The most common acute complication found in our review was hypoglycemia, reported in 56 % of the patients.21 Of the 29 % of patients who had been hospitalized because of hypoglycemia, only 13 % knew it to be a complication of the treatment.33 The patients who managed their diabetes with insulin correctly identified the steps to follow in the event of hypoglycemia.28 The United Kingdom Prospective Diabetes Study (UKPDS) confirmed that improved glucose and blood pressure control reduces diabetic complications.18
As regards annual controls to prevent potential complications, the studies generally showed them to be made quite regularly.15,21,28 Seventy-eight percent of the diabetic patients reported having an eye exam in the past year28; between 80 %15 and 50 %21 had a podiatric evaluation; and 31 % had seen a dietician.28 However, only one-third were evaluated for psychological well-being.21
Consequences of the diseaseThe reviewed studies documented potential patient concerns about their health and lifestyle changes — mainly diet and physical activity — and the impairment of social relations.9,16,21 Having different eating habits means that the relationship of diabetic patients with other people changes because they cannot go to the same places without damaging their health, and this may even result in the loss of friendships.9 Thirty-nine percent of the patients reported that their treatment interfered with their normal life.21 In turn, 23 % complained of weight gain since the start of current therapy, with a mean increase of 7.3 kg.13
Regarding the barriers which patients face, the studies cited technical language, the number and combinations of drugs prescribed, physicians lacking the right skills, with no time or no tools (e.g., help in decision making) to effectively and efficiently care for them, and a lack of incentives to invest time and effort to implicate patients in choosing the most appropriate treatment.23,34 The most common occupational complications were absenteeism from work to visit the primary care centre due to an acute problem or complications of diabetes.9 These complications may make it impossible for patients to do their work, with the subsequent possible change in employment or early retirement due to disability.9,27
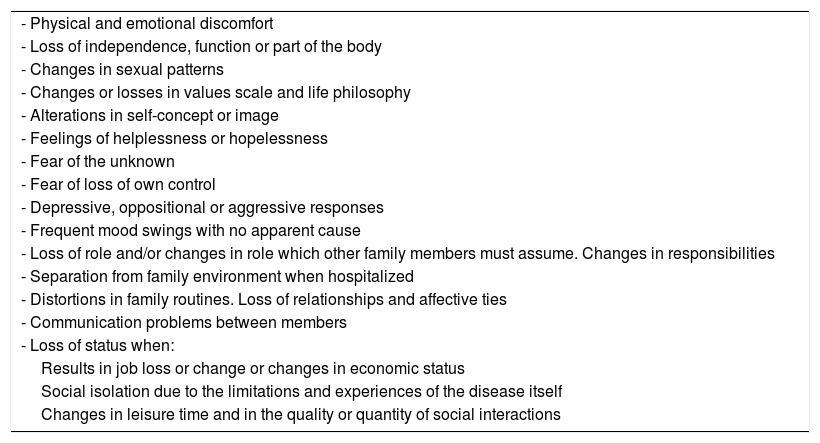
Quality of life: emotional problems and concernsThe reviewed studies showed patients to be largely concerned about how the disease will affect their quality of life (Table 3), and its emotional consequences. The most relevant problems cited by the different authors were concerns about the development of serious complications, feelings of guilt, anxiety about food,15,20,30 and fear of progression of the illness in the future.9,18 These concerns persist throughout the disease process, particularly in patients treated with insulin and those most implicated in management of the disease.9,15,29 Forty-one percent of the patients continued to experience important discomfort, but only 10 % received specific psychological management for such discomfort.15 These concerns also appeared in studies exploring the opinion of the medical professionals.16,29
Most relevant personal problems referred to loss of quality of life.
| - Physical and emotional discomfort |
| - Loss of independence, function or part of the body |
| - Changes in sexual patterns |
| - Changes or losses in values scale and life philosophy |
| - Alterations in self-concept or image |
| - Feelings of helplessness or hopelessness |
| - Fear of the unknown |
| - Fear of loss of own control |
| - Depressive, oppositional or aggressive responses |
| - Frequent mood swings with no apparent cause |
| - Loss of role and/or changes in role which other family members must assume. Changes in responsibilities |
| - Separation from family environment when hospitalized |
| - Distortions in family routines. Loss of relationships and affective ties |
| - Communication problems between members |
| - Loss of status when: |
| Results in job loss or change or changes in economic status |
| Social isolation due to the limitations and experiences of the disease itself |
| Changes in leisure time and in the quality or quantity of social interactions |
Source: Velázquez-Mendoza and Balcázar Nava.9
In this section we have focused on the practices currently used to improve management of the disease, particularly on the part of the patient and the healthcare professionals. The most important aspects are: 1) the promotion of patient self-management; 2) patient education; and 3) relationships with the healthcare professionals.
Promotion of patient self-managementSelf-management is defined as individual competence developed by patients through increased knowledge of their disease and the advice of their physician to improve the management of symptoms, treatment, physical and psychosocial consequences and lifestyle changes inherent to a chronic disease, with the aim of minimizing the effects of the illness.35
Data have been found showing patient self-management to be low, particularly referred to diet and exercise. This is attributable in part to the psychosocial problems which the disease causes,15 though the data improve when the patient switches medication to insulin and becomes more aware of the seriousness of the disease.13 Physicians acknowledge that patients are concerned and that these issues interfere with their self-management efforts.15,22
The studies identify the following elements as being important in order to optimize diabetes self-management: diet, physical exercise, self-medication, blood glucose monitoring, and annual and regular podological and eye controls.28,36,37 Patient-targeted interventions (coaching to induce the patient to ask questions and participate in decisions), improvements in quality of life and in the physiological markers of disease control, the exchange of information in the clinic regarding personal and social matters, and the patient values and preferences, may be of crucial importance for the patients and clinicians implicated in dealing with the disease.36,37 Self-management is seen to be most common among younger individuals with a higher educational level.16,20,23
Self-care is another particularly relevant element in research. This consists of actions performed by patients for the benefit of their own health, without formal medical supervision.38 The degree to which individuals follow appropriate self-care behavior is conditioned by their health beliefs.37 In the studies included in the present review, patients specifically appreciated direct and non-accusatory communication from the physician when talking about their poor self-care.22,30 Thirty percent of the patients were reluctant to discuss their self-care behaviours with the physician out of fear of being judged, not wanting to defraud the physician, or feelings of guilt and shame.30 In fact, the physicians reported the discussion of self-care to be associated with greater agreement on treatment strategies and goals, resulting in improved self-care and greater self-management of diabetes.15,21,22,37
Patient educationIn the articles analysed, we found patients to have a lack of information and education. Adequate education is essential to control the disease and reduce complications, especially in relation to lifestyle changes with a low-fat, low-calorie diet and physical exercise for at least 150 min a week.39 In order of importance, education comprises: information on the prevention of complications, long-term chronic complications, the relationship between diabetes and exercise, hypoglycemia and hyperglycemia, diet, treatment purposes and methods, blood glucose monitoring, sexual activities during diabetes, side effects of medicines, working life, forms of protection against diabetes, recent changes in treatment, insulin pumps and ways to improve quality of life.27
Participation rates in educational programs range from 68 %27 to 49 %.21 Hospital education sessions were appreciated because they covered aspects of diabetes management which the patients had not thought about before.17 The studies found the demand for diabetes education to increase in patients with longer evolving disease,23,32,36,39 and in the presence of a history of disease in a first-degree relative.32 More active and participatory educational interventions (cognitive-behavioural and behaviour modifying interviews) involving greater patient collaboration have been shown to be more effective than the provision of passive information, with improved glycemic control.36,37,39 A significant finding is that the longer the duration of education, the greater the desire to further increase it.27 Therefore, people with diabetes should be offered continuous, protocolized and systematized education, with clear objectives, at the time of diagnosis and during the course of the disease.22,31,39 Most successful patient education programs tend to involve frequent contact and reinforcement.17,31,36
Relationships with the healthcare professionalsIn almost all the reviewed articles, the patients rated the quality of their relations with the health professionals as good; up to 89 % had a positive opinion in this regard.15 At the same time, they complained of a lack of specific and individualized attention, close communication, and support for participation in their treatment. In other words, they described one-way interventions where the professional is an authoritarian figure, penalizing behaviour not compliant with the instructions received, particularly among younger patients and subjects with a higher educational level.19,20 Complaints and discomfort have been expressed.30 The patients feel that they are made to feel guilty about their situation, and this can cause them to lie, not admit difficulties, or abandon the professional or healthcare system.20,30 Another study found a certain negative bias on the part of physicians towards overweight patients, considering them as "non-compliers" — with the resulting shame reaction in some patients because of being overweight.30 A shift from the traditional biomedical model of care towards a biopsychosocial model would result in positive changes.37 Such a bidirectional model is very much demanded by patients.20,36,40 Despite confirmation of the success of this type of model, it is difficult to put it into practice in the clinic. The National Patient Safety Foundation reports that there are quite a few barriers to starting this kind of initiative. Such barriers include a desire for autonomy, a lack of physician experience and leadership,23,41 or limited visiting time.42
Trust and confidence are also addressed in the studies in reference to the professional-patient relationship.20,30,36 The elements considered essential and motivating in interaction with the healthcare professionals are essentially of a human nature: feeling listened to, being cared for, understanding, acceptance and being able to express personal discomfort.30 Patients want to know the truth about their health status and the possible therapies or recommendations, and also wish to express their point of view and needs.14,17,20 The reviewed studies describe a need for the relationship to be based on a therapeutic alliance: a collaboration agreement or pact between the professional and the patient.20 The studies underscore that understanding and exploration of physician-patient communication should include specific communication tasks and behaviours, and interpersonal/relational skills, with a view to establishing a relationship based on trust and confidence.17,30 Patients also recognize that without medical help in modifying lifestyles, such modification could be detrimental rather than beneficial.14,17
On the other hand, the publications indicate that physicians recognize the emotional difficulties of patients: the great emotional burden at work, perceived limitations in their life, fear of the consequences of the disease, social difficulties, and major priorities such as sick spouses, work, school, or simply not being able to check blood glucose.16 It is also noted that physicians, on their part, report experiencing stress and anxiety because of the need to adhere to the time limitations of a standard medical visit, and feel that they lack the experience to better support their patients. Some physicians also report problems detecting the emotional difficulties of their patients.16,30 In fact, nurses were better aware of the patient psychosocial problems, and used psychological strategies more often than physicians who were rated as having more limited skills.30
DiscussionThe consequences that most concern patients are those referred to changes in their health and lifestyle, particularly diet, exercise and social relations.16,21,26 Physical discomfort and possible dependence can lead to occupational, social and family detachment and, consequently, to a change in values scale and feelings of helplessness, anxiety, guilt, fear and depression.9,15,18,20,29,30 The professionals also consider these same concerns to be important.16,29 On the other hand, the reviewed studies confirm that the costs of diabetes are the highest among the chronic diseases, due to the high prevalence of temporary disability, mortality, complications and expensive treatments.6,7,25 These costs are largely attributable to non-adherence, with a resulting increase in the number of outpatient visits, emergency care and hospital admissions.3,24,26 Another way in which costs can be reduced at healthcare level is by supporting multidisciplinary teams with increased coordination and efficacy, including mental health resources.41
Poor adherence is strongly related to the cost of the disease. Many studies have confirmed the benefits in the clinic of communication, information and the negotiation of treatments that best adapt to the physical and emotional conditions of the patient, in order to ensure maximum adherence to therapy, with empowerment and the generation of confidence. Reinforcement based on the goals reached is also important, taking care not to judge patients for their failures, minimizing the costs and negative effects for the patient, and increasing emotional well-being.31,34 Many of these studies identify areas with room for improvement, such as poor support and information on the possible consequences and treatments, or the time spent with patients and their continuity with the physician.17,22,23
Three important bases have been found in the literature for improving the management of therapy: self-management, education, and the physician-patient relationship.
With regard to self-management, the most significant aspects are self-medication, the monitoring of glucose,23,28 care of diet and exercise, and reporting for regular checkups.28 Self-management was seen to be most common among younger individuals with a higher educational level.20,23 The physicians are of the opinion that with increased discussion about areas of self-care, with increased agreement on the objectives that empower the patients and improve their quality of life, it would be possible to achieve greater self-efficacy in diabetes care and greater patient implication in self-management.22,36,37
With regard to education, there was unanimity in the articles in underscoring that information is essential to control the disease and reduce its complications.39 The demand for education is continuous in patients,31,39 especially in those who have been ill for the longest time32,39 and who have received more education.27 The most widely accepted modality is active and participatory education.37,39 The most demanded topics are the prevention of complications, the relationship between diabetes and exercise, hypo- and hyperglycemia, diet, treatment purpose and methods, blood glucose monitoring, sexual activities, side effects of medication, working life, forms of protection against diabetes, and ways to improve quality of life.27
In the doctor-patient relationship, confidence and the therapeutic alliance are key elements.20,30,36 The most positively valued aspects are: feeling listened to, feeling cared for, understanding, acceptance, and being able to express personal discomfort.30 The trend is therefore towards a more biopsychosocial model in which the patient plays a more active role, and attention is focused on the needs of the patient and not only on isolated healing of the disease.8,20,36,37,40 Many studies show that consensus on treatment lessens patient anxiety and makes patients feel more confident and with a sensation of greater control of their disease.43–45 Despite these advantages, it is difficult to implement initiatives of this kind in the clinic, due to the limited time that can be dedicated to each patient.23,42
The present study has limitations. In compiling the articles for review, there may have been selection bias (non-randomization), performance bias (attention differences) and detection bias (differences in outcome assessment), due to the type of design, population diversity, and the methodology used. This represents a significant limitation of the study, because in the presence of many primary articles with methodological deficiencies or weak designs, the conclusions will prove questionable even when the results are comparable. Nevertheless, our review has examined the best evidence available to date on the study subject. Its contribution thus focuses on the compilation and organization of such data with a view to improving future lines of research, and to alert to the need for solid research designs in order to address the issues which our review has found to be important.
Another limitation of the review would be the fact that since the included studies mainly involved qualitative designs and small samples, they could be biased with regard to their capacity to represent their respective populations. However, this narrative review does not intend to draw conclusions at population level, but rather to organize the information available to date and to point out the areas with room for improvement in relation to our study subject. Although the sample sizes of the studies are small, given the number of articles included (n = 42), we believe that the information obtained is both useful and valuable. In any case, the described potential biases will facilitate reader assessment of the present study.
ConclusionsPatients experience the diagnosis of diabetes with a strong emotional response. Treatment involves efforts and sacrifice, with no immediately visible benefits. Patients run into lifestyle, psychological, and environmental barriers that complicate adherence to therapy. A lack of adherence implies worsened patient health and an increase in healthcare costs.
To achieve adequate adherence, we must focus on ensuring maximum patient self-management of the disease. Patients would greatly improve their quality of life, and the healthcare, economic and social costs would decrease considerably as a result. A rapid and effective relationship with the health services, and quality education, would facilitate management of the disease.
Rapid and easy access to medical care, with close, open and fluid physician-patient communication, i.e., shifting towards a more biopsychosocial model of care, would promote a positive change towards a relationship based on a therapeutic alliance, with collaboration between the patient and physician, and an open and patient-centred care practice.
The other cornerstone of self-management is education. Active and participatory education would offer patients the information needed for good understanding of their disease, thereby allowing them to manage it autonomously and to make adequate decisions about resources.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Nombela Manzaneque N, Pérez-Arechaederra D, Montalbán Caperos JM. Efectos secundarios y prácticas para mejorar la gestión de la diabetes tipo 2 desde el punto de vista de la vivencia del individuo y de la gestión de la atención sanitaria. Revisión narrativa. Endocrinol Diabetes Nutr. 2019. https://doi.org/10.1016/j.endinu.2019.05.010