







Although former studies indicated that Asturias (Spain) is an iodine-sufficient region, preliminary data suggest this trend may be changing.
ObjectiveTo determine the prevalence of iodine deficiency in pregnant women in Asturias.
Material and methodsWe designed an observational, prospective, multicenter study. The urinary iodine concentration (UIC) of 371 pregnant women was analyzed between November 2021 and March 2023. Participants were recruited from the three central areas of the Principality of Asturias (Areas III, IV, and V). The project received approval from the Research Ethics Committee of the Principality of Asturias (RECPA).
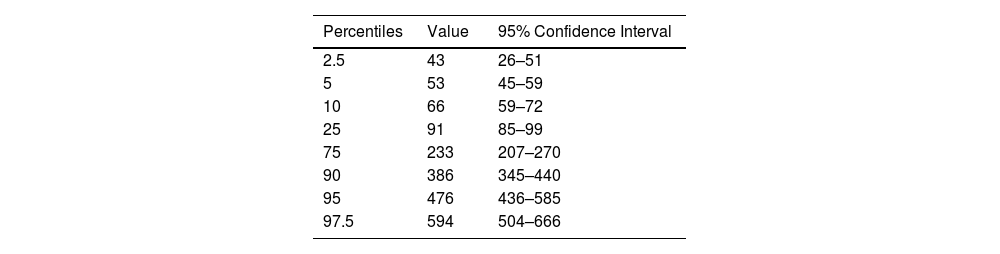
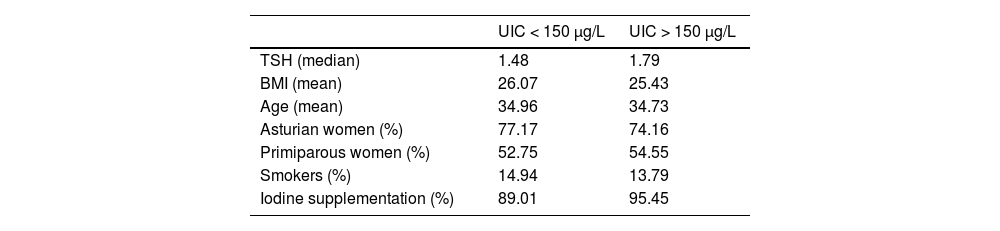
ResultsA total of 52% of pregnant women had urinary iodine levels indicative of iodine deficiency (< 150 μg/L). The average UIC in our cohort was 146 μg/L. We compared thyroid-stimulating hormone (TSH) levels between pregnant women with iodine deficiency and those with sufficient iodine, but found no statistically significant differences in TSH levels between the two groups. We also couldn't establish statistically significant links between iodine deficiency status and body mass index (BMI), number of previous births, nationality, or age. Furthermore, iodine deficiency did not show a significant link to obstetric complications such such as hypertension during pregnancy or premature birth.
ConclusionsThese findings support the hypothesis of an increase in iodine deficiency during the first trimester of pregnancy in our population. This highlights the urgent need to review our supplementation strategies and nutritional education programs.
Según estudios previos, Asturias es una región con suficiencia de yodo, pero datos preliminares sugieren un cambio de tendencia.
ObjetivoDeterminar la prevalencia de yododeficiencia en gestantes de Asturias.
Materiales y métodosSe diseñó un estudio observacional, prospectivo y multicéntrico. Se analizó la concentración urinaria de yodo (CUI) de 371 gestantes entre noviembre del 2021 y marzo del 2023. La captación se realizó en las tres áreas centrales del Principado de Asturias: III, IV y V. El proyecto fue aprobado por el Comité de Ética de Investigación del Principado de Asturias (CEImPA).
ResultadosEl 52% de las gestantes presentó niveles de yoduria indicativos de yododeficiencia (<150 μg/L). La mediana de la CUI en nuestra cohorte fue de 146 μg/L. La hormona estimulante del tiroides (TSH) fue comparada entre los dos grupos de gestantes, aquellas con déficit de yodo y las que tenían suficiente cantidad de yodo, sin encontrar diferencias estadísticamente significativas entre las medias de la TSH en ambos grupos. Tampoco se han podido establecer asociaciones estadísticamente significativas entre el estado de yododeficiencia y el índice de masa corporal (IMC), la paridad, la nacionalidad o la edad. Así mismo, el déficit de yodo no tuvo una asociación significativa con complicaciones obstétricas tales como los estados hipertensivos del embarazo o la prematuridad.
ConclusionesEstos hallazgos respaldan la hipótesis de un aumento de la yododeficiencia en el primer trimestre del embarazo en nuestra población, lo que resalta la urgencia de revisar las estrategias de suplementación y los programas de educación nutricional.
