






To analyze the relationship between serum levels of uric acid and the severity of coronary disease.
MethodsThis observational, descriptive and cross-sectional study included 77 patients previously selected using inclusion criteria, from September 2014 to May 2015. It was conducted in a third level regional hospital from Guayaquil, Ecuador. Patients enrolled in this study were older than 30 years with coronary disease undergoing coronary angiography, without prior diagnosis of any other condition that could influence in serum uric acid values.
Results(1) Direct relation between serum uric acid levels and the severity of coronary disease, with a 0.600 Spearman correlation coefficient (p<0.001); (2) other variables such as hypertension and medical history did not have an influence on the study's results; (3) serum uric acid levels didn’t show difference among the different groups (p˃0.05).
ConclusionsBased on the results, it was possible to conclude that there is a relation between serum uric acid level and the severity of coronary artery disease; this relation was independent of clinical diagnosis and hypertension. According to this, serum uric acid levels can be taken as a practical and inexpensive parameter related to the severity of coronary artery disease. As a primary preventive intervention, we recommend maintaining levels within normal parameters in patients with cardiovascular risk.
Analizar la relación entre los niveles séricos de ácido úrico y la severidad de la enfermedad coronaria. Métodos: Este estudio observacional, descriptivo y transversal incluyó 77 pacientes previamente seleccionados mediante criterios de inclusión, desde septiembre de 2014 a mayo de 2015. Se realizó en un hospital regional de tercer nivel de Guayaquil, Ecuador. Los pacientes incluidos en este estudio eran mayores de treinta años, con enfermedad coronaria sometidos a angiografía coronaria, sin diagnóstico previo de ninguna otra condición que pudiera influir en los valores de ácido úrico sérico.
Resultados1) Relación directa entre los niveles séricos de ácido úrico y la gravedad de la enfermedad coronaria, con un coeficiente de correlación de Spearman de 0.600 (p<0.001); 2) Otras variables como la hipertensión y el historial médico no influyeron en los resultados del estudio; 3) Los niveles séricos de ácido úrico no mostraron variabilidad entre los diferentes grupos (p˃0.05).
Conclusionesde acuerdo con los resultados, fue posible concluir que existe una relación entre el nivel sérico de ácido úrico y la severidad de la enfermedad coronaria; esta relación fue independiente del diagnóstico clínico y la hipertensión. De acuerdo con esto, los niveles séricos de ácido úrico se pueden tomar como un parámetro práctico y económico relacionado con la gravedad de la enfermedad arterial coronaria. Como intervención preventiva primaria, recomendamos mantener los niveles dentro de los parámetros normales en pacientes con riesgo cardiovascular.
Coronary artery disease (CAD) is a pathology that is characterized by an inadequate arterial blood supply to the heart muscle.1,2 The dysfunctional endothelium is the fundamental axis of many cardiovascular pathologies, it is induced by genetic, biochemical and hemodynamic defects, which in turn can be influenced by well-known risk factors, some of which can be modifiable and controllable, while others cannot. However nowadays there is an increasing interest on novel risk factors, like serum uric acid level, that can help to establish an early diagnosis or a better risk stratification.3–9
The association between serum levels of uric acid and cardiovascular disease is a topic that has been discussed for several years.10–12 Thus, there are many studies that have proven the relationship between hyperuricemia and some cardiovascular diseases.13–15
Uric acid is the final product of the catabolism of purine bases. Purines have both an endogenous origin (synthesis of purines and catabolism of nucleic acids) and exogenous origin (from the purine-rich diets).16 One of the explanations about the pathogenic role of uric acid in cardiovascular morbidity is from the formation of free radicals, platelet adhesiveness and aggregation, which are responsible for theformation of thrombi.17–19 In addition, high levels of uric acid are also related to endothelial dysfunction, antiproliferative effects, alteration in the production of nitric oxide, lipid peroxidation and smooth muscle proliferation.20–26
Hyperuricemia is frequently found in patients with coronary heart disease. Despite the evidence, there is still controversy in the relationship between hyperuricemia and CAD, especially when trying to establish this laboratory parameter as an independent risk factor for a coronary event. In fact, some epidemiological studies have described that the relationship between uric acid and CAD can be considered as an epiphenomenal and not causal element, since the uric acid correlates with some of the classic risk factors of CAD such as hypertension, male sex, diabetes mellitus, dyslipidemia, etc. However, recently a study by Gaubert et al. found the existence of a significant linear correlation between serum uric acid levels and endothelial dysfunction, even after having adjusted the analysis for confounding variables. 27
Additionally, the study conducted in China by Wu et al.,28 took 2142 healthy individuals older than 65 years and determined that high levels of UA are able to predict, independently, the risk of new events EAC events.
The evidence in favor of uric acid as an independent risk factor for CAD, and even as a predictor of severity, is gaining more weight due to the increasing number of publications that are corroborating this theory. However, the majority of association studies between uric acid and CAD have been carried out in non-Latin American populations (primarily American and Asian). For this reason, there is a need to carry out this type of analysis within a Latin population. Finally, the objective of this work is to establish the relationship between serum uric acid levels and the severity of CAD (measured by coronary angiography) in the Ecuadorian population.
MethodsStudy design and participantsThis was a 9-month observational, descriptive and cross-sectional study conducted in Dr. Teodoro Maldonado Carbo Hospital, Guayaquil, Ecuador. Patients enrolled in this study had to be older than 30 years old, any gender, with a recently diagnosis of coronary artery disease elective for cardiac catheterization, and without prior diagnosis of cardiovascular disease or any other condition or treatment that could alter serum uric acid values, such as chronic kidney disease, hepatic disease, or taking specific treatment that affects uric acid levels. The following data collection resources were used: questionnaires and information obtained from the medical history of each patient; laboratory tests for measurement of serum uric acid; cardiac catheterization to identify the degree of severity of CAD. Other patient information collected at baseline included prior diagnosis of hypertension or diabetes, previous history of hyperlipidemia, stroke, cardiac catheterization and family history of cardiovascular disease.
Written consent was obtained from each participant prior to their inclusion. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution's human research committee.
For laboratory test, all samples were taken in a fasting state, and were analyzed using the spectrophotometry method. For statistical analysis, the laboratory results of uric acid were grouped into:
For men
- •
Normal≤7
- •
Hyperuricemic>7
For women
- •
Normal≤6
- •
Hyperuricemic>6
Cardiac catheterization was performed by an interventional cardiologist. The results were taken from the hospital's S400 system. Regarding this point, the interventional cardiologist did not know the serum uric acid levels of the patients or the population to be studied, thus reducing the probability of bias. The angiographic grades for statistical analysis were grouped in five stages, approved by interventional cardiologists29:
- •
0: no obstruction
- •
I: obstruction ≥50% of 1 coronary vessel
- •
II: obstruction ≥50% of 2 coronary vessels
- •
III: obstruction ≥50% of 3 coronary vessels
- •
IV: obstruction ≥50% of the left coronary trunk
A descriptive analysis was performed using frequencies and percentages or medians with standard deviation (SD) as appropriate. The relation between serum uric acid levels and severity of CAD was evaluated based on the Spearman analysis. In addition, the Levene and Anova tests were used to compare means and variances for a single sample. A p<0.05 was considered statistically significant. The tabulation of the data, its analysis and the elaboration of tables and graphs was done with assistance of SPSS v21.0 2012 (SPSS Inc., Chicago, Illinois, USA) software.
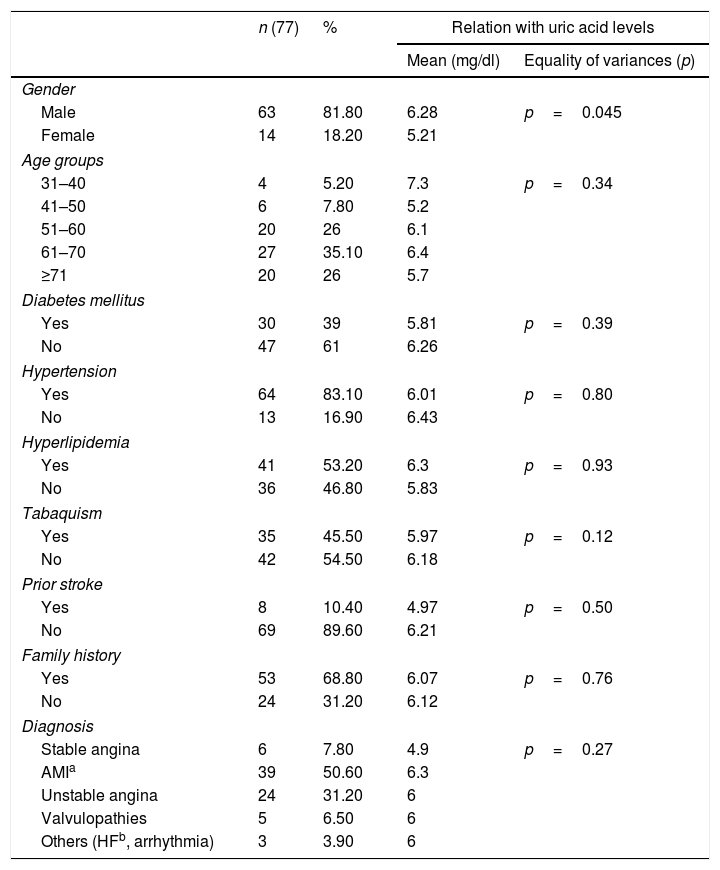
ResultsInitially, the sample consisted of 112 patients. When applying exclusion criteria, the study sample was established in 77 patients suitable for analysis. There was predominance of male gender: 63 (81.8%) vs 14 (18.2%). Regarding age groups, 61.1% of the patients were older than 60 years; 33.8% were between 40 and 60 years old, and only 5.2% of patients were under 40 years. Difference was found with respect to uric acid levels between genders (p=0.045), respect to age groups (p=0.34) no differences were found. Other participants data are showed in Table 1.
Clinical characteristics of patients and comparison with uric acid levels.
| n (77) | % | Relation with uric acid levels | ||
|---|---|---|---|---|
| Mean (mg/dl) | Equality of variances (p) | |||
| Gender | ||||
| Male | 63 | 81.80 | 6.28 | p=0.045 |
| Female | 14 | 18.20 | 5.21 | |
| Age groups | ||||
| 31–40 | 4 | 5.20 | 7.3 | p=0.34 |
| 41–50 | 6 | 7.80 | 5.2 | |
| 51–60 | 20 | 26 | 6.1 | |
| 61–70 | 27 | 35.10 | 6.4 | |
| ≥71 | 20 | 26 | 5.7 | |
| Diabetes mellitus | ||||
| Yes | 30 | 39 | 5.81 | p=0.39 |
| No | 47 | 61 | 6.26 | |
| Hypertension | ||||
| Yes | 64 | 83.10 | 6.01 | p=0.80 |
| No | 13 | 16.90 | 6.43 | |
| Hyperlipidemia | ||||
| Yes | 41 | 53.20 | 6.3 | p=0.93 |
| No | 36 | 46.80 | 5.83 | |
| Tabaquism | ||||
| Yes | 35 | 45.50 | 5.97 | p=0.12 |
| No | 42 | 54.50 | 6.18 | |
| Prior stroke | ||||
| Yes | 8 | 10.40 | 4.97 | p=0.50 |
| No | 69 | 89.60 | 6.21 | |
| Family history | ||||
| Yes | 53 | 68.80 | 6.07 | p=0.76 |
| No | 24 | 31.20 | 6.12 | |
| Diagnosis | ||||
| Stable angina | 6 | 7.80 | 4.9 | p=0.27 |
| AMIa | 39 | 50.60 | 6.3 | |
| Unstable angina | 24 | 31.20 | 6 | |
| Valvulopathies | 5 | 6.50 | 6 | |
| Others (HFb, arrhythmia) | 3 | 3.90 | 6 | |
From: Data of patients undergoing cardiac catheterization.
A significant number of patients were hypertensive (83.1%), the difference between the two groups was not significant (p=0.80) when they were related to uric acid levels. Diabetes mellitus affected more than half of the patients studied (61%), and also no difference was found between the groups when they were related to uric acid levels (p=0.39). In the same context, no significant difference was found in patients with a history of hyperlipidemia (53.2%, p=0.93). Finally, as one of the habits related to coronary disease, smoking was considered, found in 45.5% of patients, without significant difference when related to uric acid (p=0.12). When investigating family history of cardiovascular disease, we found that 68.8% of these patients had a first-degree relative with a condition of this type. However, the variance when related to uric acid levels was not significant (p>0.05).
According to the initial diagnosis or clinical presentation, 89.6% of the patients had a condition with some degree of coronary involvement (acute myocardial infarction 50.6%, unstable angina 31.2%, stable angina 7.8%). A small percentage suffered from valvular heart disease and other diseases (10.4%). When relating these conditions to the levels of uric acid obtained, there was no evidence of difference between the different groups (p=0.27) (Fig. 1).

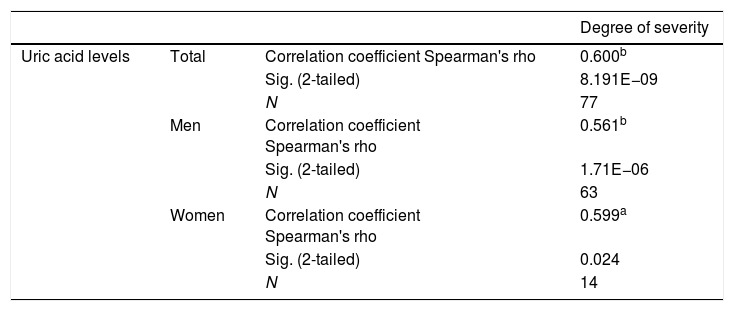
As mentioned, the serum uric acid values obtained were grouped into two groups for analysis. We observed that 24.7% of patients were hyperuricemic. Likewise, the findings obtained in coronary angiography were classified in five stages. Among the patients, 6.5% were in stage 0, 23.4% classified in stage I and 23.4% in stage II. Within stage III and IV, 27.3% and 19.5% of the patients were found, respectively. To determine the relationship between serum levels of uric acid and the severity of coronary disease, Rho de Spearman test was used for nonparametric tests. As shown in Table 2, a significant relation was obtained (p<0.01), with a correlation coefficient close to 1 (0.600). However it is well-known that sex may be a confounding variable, so the analysis was adjusted for sex, and the result showed that independent from this variable, the relation between the uric acid levels and the severity degree of CAD was maintained as shown in Fig. 1, and the correlation for men (0.561) and women (0.599) was significant. Fig. 2 shows the direct relation between serum levels of uric acid and the severity of coronary disease. In this graph it is observed that the higher the uric acid levels, the greater the severity of coronary disease for men or women.
Correlation between uric acid levels and severity of coronary disease.

In addition, to demonstrate that hypertension did not represent a confounding variable for the correlation of uric acid levels and degree of severity of coronary disease, these variables were plotted in pooled error bars. Thus, it was obtained that patients with a higher severity of coronary disease had higher levels of uric acid regardless of whether they were hypertensive or not. When applying the Levene test for comparison of variances in independent samples of arterial hypertension and uric acid levels, it was found that there is no statistical significance. Therefore, it is assumed that the difference in means between hypertensive and non-hypertensive patients is not significant.
Finally, it was demonstrated that the relationship found between uric acid levels and the severity of coronary disease was equal between different clinical conditions studied, and according to the Anova test to compare the means of a factor, no significant difference was found among the different groups (p=0.50).
DiscussionIn the present study we find that there is a positive relationship between serum uric acid levels and the severity of coronary disease. This relationship was significant through various correlation tests of a quantitative variable and an ordinal variables. It is possible to explain the results obtained by knowing the role played by uric acid as an oxidizing molecule: forming free radicals; stimulating platelet aggregation and thrombus formation, endothelial dysfunction, smooth muscle proliferation and alteration in the production of nitric oxide.30,31 All these are pathophysiological events that alter coronary arteries, thus aggravating the coronary artery disease. Unlike other studies32 in which uric acid levels are related to AMI, this research links the severity of coronary disease with uric acid levels in the context of the different cardiovascular diseases such as: stable and unstable angina, AMI, valvular diseases, cardiomyopathies and heart failure.
It was observed that the relationship obtained was independent of the patient's clinical condition, age or the presence of hypertensive disease. By using statistical tests, it was obtained in a significant way that the serum levels of uric acid did not differ between the groups. Thus, it is considered that these parameters were not confounding variables. These results were opposite to those reported in other clinical studies such as that of Conen and colleagues, a study in which variation of uric acid levels is found among the different variables such as diabetes, hypertension and dyslipidemia.33 However, one of the variables that should be studied in greater depth is gender. According to other studies, there is a stronger relationship between serum levels of uric acid and coronary heart disease in women.34 In this study, this theory could not be demonstrated because the female gender represented a small percentage of the population studied (18.2%) and, conversely, no variation was found between the male and female gender when assessing this relation.
ConclusionsThe present investigation has been devoted to the study of the relation of the serum levels of uric acid and severity of coronary disease. The objectives initially proposed were achieved: serum uric acid values in patients with coronary disease, establish the degree of severity of coronary disease from coronary angiography, and relation between serum uric acid levels and severity of coronary disease, the latter being independent of the clinical condition, associated comorbidities, demographic characteristics and patient habits.
Certain limitations are found in this study: the small population studied; the significant differences between some variables (e.g.: gender and hypertension) finding a higher percentage of male and hypertensive patients; the measurement of uric acid in a single sample, existing according to various studies a small variation in uric acid levels when measured repeatedly; and the non-follow-up of the patients studied, with future coronary arteriography to be performed. However, some remarkable strengths of the study are the use of a single measuring instrument for uric acid and severity of coronary disease variables, and measurement of laboratory variables in a fasting state, thus avoiding possible alterations with food intake.
Thus, considering that coronary disease is nowadays one of the main causes of morbidity and mortality worldwide, the serum measurement of uric acid, as a practical and economic laboratory data, can be assessed as a parameter related to the severity of coronary artery disease. Also, a decrease in serum uric acid values may be considered in patients with risk factors for cardiovascular disease, either through uricosuric drugs or low purine diet. We recommend (1) perform research with more population and study time. (2) Propose a research model that studies non-hypertensive patients, considering that in medical literature various studies show a close relation between uric acid levels and hypertensive disease. (3) Elaborate a research with predictive design, generating a model that allows the study of uric acid as a predictor of coronary severity.
FundingThe present investigation has not received any specific grant from agencies of the public, commercial, or non-profit sectors.
Conflicts of interestsThe authors state that there are no relevant conflicts of interest in this study.
The authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.