



To describe the management of atherogenic dyslipidemia (AD) in routine clinical practice in the Primary Care (PC) setting in Spain.
MethodsObservational, descriptive, cross-sectional study based on a structured questionnaire designed for this study and addressed to PC physicians. The questionnaire content was based on a literature review and was validated by 3 experts in AD.
ResultsA total of 1029 PC physicians participated in the study. 96.99% indicated that AD is determinant for cardiovascular risk, even if LDL-C levels are appropriate. 88.43% evaluated residual cardiovascular risk in their clinical practice, however, only 27.89% of them evaluated it in secondary prevention.
Regarding diagnosis, 82.22% reported that TC, TG, HDL-C and non-HDL-C are essential measures when evaluating AD. Almost all physicians reported that they can request fractionated cholesterol to assess HDL-C and LDL-C, however 3.69% could not.
Physicians (95.63%) considered that the first step in AD treatment should be diet, regular exercise, smoking cessation and pharmaceutical treatment, if necessary. 19.1% agreed partially or completely that gemfibrozil is the most suitable fibrate to associate with statins. 74.83% completely agreed that fenofibrate is the most suitable fibrate to combine with statins.
ConclusionsPhysicians have access to general Spanish guidelines and recommendations associated with AD management, however, it is necessary to continue rising awareness about the importance of early detection and optimal control of AD to reduce patients’ cardiovascular risk.
Describir el manejo de la dislipemia aterogénica (DA) en la práctica clínica, en el ámbito de la atención primaria (AP) en España.
MétodosEstudio observacional, descriptivo y transversal, por medio de un cuestionario ad-hoc estructurado, dirigido a médicos de AP. El contenido del cuestionario se basó en una revisión de la literatura y fue validado por 3 expertos en DA.
ResultadosParticiparon en el estudio 1.029 médicos de AP. El 96,99% coincidió en que la DA constituye un factor determinante del riesgo cardiovascular aunque los niveles de cLDL sean adecuados. Un 88,43% indicó que evaluaba el riesgo residual cardiovascular en su práctica clínica habitual, aunque un 27,89% lo evaluaba solo en prevención secundaria.
Un 82,22% consideró que para la valoración de un paciente con DA es imprescindible conocer el colesterol total, los triglicéridos, el cHDL, el cLDL y el no-cHDL. La mayoría indicó que podía solicitar fraccionamiento del colesterol total para valorar el cHDL y el cLDL, de forma rutinaria sin restricciones, pero el 3,69% indicó que no.
Un 95,63% consideró que el primer paso en el tratamiento implica un control de la dieta, ejercicio físico, abandono del tabaco y si se precisa, tratamiento farmacológico. Un 19,1% estaba parcial o completamente de acuerdo en que el gemfibrozilo es el fibrato más adecuado para asociar con estatinas. El 74,83% estaba completamente de acuerdo en que el fenofibrato es el fibrato más apropiado para combinar con estatinas.
ConclusionesLos médicos tienen acceso a las guías y recomendaciones clínicas sobre el manejo de la DA, pero es necesario continuar concienciando de la importancia de su detección precoz y control óptimo para limitar su riesgo cardiovascular.
Atherogenic dyslipidemia (AD) is a disorder of lipid and lipoprotein metabolism. It characteristically presents with an increase of total triglyceride (TG) plasma levels, a decrease in the concentration of cholesterol transported by high-density lipoproteins (HDL-C), and an increase in small, dense low-density lipoprotein (LDL) particles, with or without a moderate increase in LDL-C.1,2 These alterations are usually accompanied by an increase in non-HDL-C and as a result, an increase in apolipoprotein B (ApoB).2
This type of dyslipidemia is associated with increased cardiovascular risk and contributes significantly to increasing the residual vascular risk of lipid origin.1–3 It is a very common lipoprotein phenotype and is associated with diseases such as coronary heart disease, insulin resistance, metabolic syndrome, type-2 diabetes mellitus (DM) or obesity, among others.1,2,4 It might be expected that the prevalence of AD would have an upward trend in parallel with DM or obesity, but in general AD tends to be underdiagnosed and consequently undertreated in clinical practice.1,2,5,6
According to data from the ENRICA study (2008–2010), 50.5% of the adult Spanish population, with no significant differences between genders, had hypercholesterolemia and 44.9% high LDL-C. Among the individuals who had high LDL-C, only 53.6% were aware of it. Less than half of them (44.1%) were being treated with lipid-lowering drugs, and of these, 55.7% were controlled.7 Based on these data, it can be seen that only 13% of individuals with hypercholesterolemia were controlled.7 In line with this study, the EDICONDIS-ULISEA study revealed that only 1 in every 6 patients with AD achieved the treatment targets for HDL-C and TGs and that approximately 20% of the patients who reached these objectives received specific pharmacological treatment for AD or any of its components.6,8 Furthermore, the EUROASPIRE III study showed that only 30.6% of patients at high cardiovascular risk treated with lipid-lowering drugs were adequately controlled.9
Clinical practice guidelines and recommendations have been developed and published with the aim of improving healthcare of patients with AD. At European level, the Guidelines of the European Society of Cardiology and the European Atherosclerosis Society (ESC/EAS),10,11 have been published. In Spain, the Multidisciplinary Expert Consensus Documents on AD4,5,12 and the Clinical Guidelines for the detection, diagnosis and treatment of AD in Primary Care2 have been issued. Regarding treatment, they recommend changes in lifestyle (healthy diet, physical activity, smoking cessation and moderating alcohol consumption) and additional pharmacological treatment when necessary. The drugs of choice established by these guidelines are statins and fibrates, opting for one drug or the other depending on patients’ clinical characteristics. If the lipid profile of the patient is not adequately controlled, the combination of a statin-fibrate treatment should be considered, with fenofibrate being the fibrate of choice.2,4,5
Knowing about patient management in routine clinical practice from the point of view of the Primary Care physician can provide key information to improve the early diagnosis, diagnostic assessment, treatment approach and clinical follow-up of patients in the Spanish healthcare system. Therefore, the aim of this study was to describe the management of the patient with AD in routine Primary Care clinical practice.
Materials and methodsStudy design and populationAn observational, descriptive, cross-sectional study was conducted by means of an ad-hoc online questionnaire addressed to Primary Care physicians. The fieldwork took place between 21 April and 29 July 2016. At the time of their participation, the physicians had practiced their profession for at least 5 years and were working in the Spanish health system. The participants answered the questionnaire based on their routine clinical practice and did not receive a previous specific course related to AD before answering it.
The minimum sample size (1009 Primary Care physicians) was estimated based on the assumption of maximum variability, the number of Primary Care physicians practicing their profession in the Spanish public health system in 2015 (37,648),13 a 99% confidence level and a precision error of 4%.
Questionnaire designA specific electronic structured questionnaire was developed for data collection (Table 1 in Appendix A. Supplementary data). The content of the questionnaire was based on information collected by means of a review of the literature on the management of and approach to AD in routine clinical practice. The questionnaire was validated by three experts in the management of AD.
The questionnaire consisted of 23 items across 4 sections: (1) residual cardiovascular risk (3 items); (2) general aspects of AD (4 items); (3) diagnosis of AD (5 items); and (4) treatment of AD (11 items) (Appendix A. Supplementary data). The questions were formulated with closed polytomous or categorized responses. Seven questions required responses via a Likert scale with values of 1–4 (not useful-very useful) or 1–5 (completely disagree-completely agree). The socio-demographic variables of the participants (age, gender, years of profession, personal history of AD, province in which they practiced their profession, and the area where their health center was located [rural (<5000 inhabitants), semi-urban (5000–19,999 inhabitants), or urban (≥20,000 inhabitants)] were also collected.
Statistical analysisThe statistical analysis was performed using the STATA version 14 statistical package. Frequency tables were used to detect anomalies in the introduction of each of the study variables and contingency tables to detect repeated or inconsistent cases. In all statistical tests, a value of p<0.05 was considered significant. Relative and absolute frequencies were calculated for qualitative variables. For quantitative variables, means, standard deviations and the distribution of percentiles were estimated. Regarding the questions whose responses were scored by means of a Likert scale, relative and absolute frequencies and 95% confidence intervals were calculated.
Ethical considerationsThe study was approved by the Clinical Research Ethics Committee of Hospital Universitario Puerta de Hierro, Majadahonda, Madrid. All participants received information relevant to the study and gave their consent to participate in it.
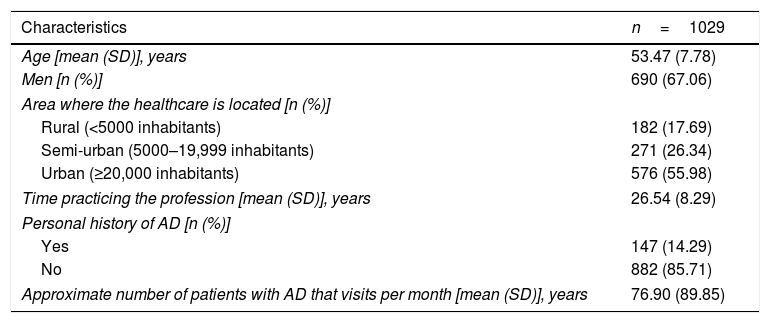
ResultsDescription of participantsA total of 1029 Primary Care physicians (67.06% men) participated in the study. The average age of the participants was 53.48 (SD: 7.78) years and the average number years of professional activity was 26.54 (SD: 8.29). Physicians from all Spanish autonomous regions participated, with Andalusia, the Valencian Community and the Community of Madrid being the most represented (15.5%, 13.9% and 10.1%, respectively). Most participants were physicians in healthcare centers located in urban areas (55.9%), followed by semi-urban areas (26.4%) and rural areas (17.7%). The participants attended to a mean of 79.9 (SD: 89.85) patients with AD per month. The socio-demographic characteristics of participants are shown in Table 1.
Socio-demographic characteristics of participants.
| Characteristics | n=1029 |
|---|---|
| Age [mean (SD)], years | 53.47 (7.78) |
| Men [n (%)] | 690 (67.06) |
| Area where the healthcare is located [n (%)] | |
| Rural (<5000 inhabitants) | 182 (17.69) |
| Semi-urban (5000–19,999 inhabitants) | 271 (26.34) |
| Urban (≥20,000 inhabitants) | 576 (55.98) |
| Time practicing the profession [mean (SD)], years | 26.54 (8.29) |
| Personal history of AD [n (%)] | |
| Yes | 147 (14.29) |
| No | 882 (85.71) |
| Approximate number of patients with AD that visits per month [mean (SD)], years | 76.90 (89.85) |
AD, atherogenic dyslipidemia; SD, standard deviation.
Most participants (88.43%) evaluated residual cardiovascular risk in their routine clinical practice. However, 27.89% of them evaluated it only in patients in secondary prevention.
Regarding the concept of lipid-origin residual cardiovascular risk, 63.5% of participants answered that it is the risk that remains after treating a patient with statins and achieving LDL-C targets. Less than half of the participants (35.76%) answered that it is the risk that remains after controlling all modifiable risk factors. Most participants (96.02%) associated the residual risk of lipid origin to AD, compared to 2.24% participants who associated the residual risk of lipid origin to obesity, 1.17% to age, and 0.58% to high blood pressure (Table 2 in Appendix A. Supplementary data).
Atherogenic dyslipidemiaFour questions were formulated about general aspects of AD and the clinical practice associated with the disorder (Table 3 in Appendix A. Supplementary data).
Most participants (76.68%) considered that AD is characterized by a decrease in HDL-C, an increase in TGs and an increase of small, dense LDL-C particles. Nearly all (96.99%) of the participating physicians agreed that AD is a determinant of cardiovascular risk despite adequate LDL-C levels. Most participants (93.0%) stated that early-onset coronary heart disease, metabolic syndrome and type-2 diabetes mellitus were AD-associated phenotypes. Lastly, 87.56% of participants indicated that in their routine clinical practice they specifically evaluate AD in patients because it increases cardiovascular risk.
Diagnosis of atherogenic dyslipidemiaFive questions were formulated concerning the diagnosis of AD (Table 4 in Appendix A. Supplementary data). Most physicians (82.22%) considered that for AD assessment it is essential to know the following components of the lipid profile: total cholesterol (TC), TGs, HDL-C, LDL-C, and non-HDL-C (Table 4A in Appendix A. Supplementary data).
The participants indicated the usefulness of the atherogenic indices by means of a 4-point Likert scale (1: not useful; 2: of little use; 3: useful; 4: very useful). The ratios considered most useful (very useful/useful) were (in order): TC/HDL-C (36.83%; 49.47%), LDL-C/HDL-C (39.36%; 45.68%), TGs/HDL-C (24.20%; 45.09%), non-HDL-C/HDL-C (12.93%; 46.94%), ApoB/ApoA1 (16.23%; 43.15%), and LDL-C/ApoB (13.70%; 42.18%) (Table 4B in Appendix A. Supplementary data).
Participants also reported the frequency with which they used lipoprotein indices in their clinical practice by means of a 5-point Likert scale (1: never; 2: almost never; 3: sometimes; 4: often; 5 very often). The most commonly used indices were the TC/HDL-C index (used often by 29.35% of participants and very often by 23.71%) and the LDL-C/HDL-C index (used often by 28.57% of participants and very often by 20.99%). Conversely, regarding the indices that the participants never used, 60.35% and 59.96% of participants indicated that they never used the LDL-C/ApoB or ApoB/ApoA1 indices, respectively (Table 4B in Appendix A. Supplementary data).
Finally, the participants reported if they could request the fractions of total cholesterol to assess HDL-C and LDL-C, in their clinical practice. 93.68% replied: “yes, routinely and without restrictions”, compared to 3.69% who answered “no” and 1.17% who answered that they could only request them by referring the patient (Table 4A in Appendix A. Supplementary data).
Treatment of atherogenic dyslipidemiaThe questionnaire included 11 questions related to the treatment of AD, of which 4 were answered by means of a Likert scale (Table 5 in Appendix A. Supplementary data).
First, the participants responded to two questions related to the initial treatment approach to AD. Almost all the participants (95.63%) considered that the first step involves diet, regular physical exercise, smoking cessation and, if necessary, pharmacological treatment. Regarding the approach of a patient with obesity-associated AD, 73.96% of participants would insist that the patient should modify his/her lifestyle and evaluate the use of pharmacological treatment. Almost one fourth of the participants (23.03%) would treat the patient together with nursing staff, 2.62% would refer the patient to the endocrinologist, and 0.39% would refer the patient to nursing staff.
Regarding the pharmacological treatment of AD, 69.97% indicated that the treatment must include a statin and a fibrate from the beginning; 19.14% considered that a patient with AD should be treated with a high-dose statin and, once the target LDL-C is achieved, the addition of another drug should be evaluated. Furthermore, 10.79% considered that a fibrate must be administered and if the therapeutic objectives are not achieved, a statin should be considered. Finally, only 0.10% of participants indicated that a statin and nicotinic acid should be administered.
Concerning the co-administration of fibrates and statins, the participants reported by means of 5-point Likert scale (1: completely disagree; 2: partially disagree; 3: indifferent; 4: partially agree; 5: completely agree) if they agreed or disagreed with 4 statements. Three fourths (74.83%) of participants completely agreed that fenofibrate is the most suitable fibrate to combine with statins, compared with 1.75% who completely disagreed.
Regarding statins, the participants also indicated their degree of agreement or disagreement with 4 statements. Most (91.54%) indicated that they completely or partially agreed that “the residual risk associated with high TGs and/or low HDL-C is not eliminated with statinsalone”. Almost half of the participants (47.81%) indicated that they completely or partially agreed with the statement “statins eliminate all residual cardiovascular risk if target LDL-C levels areachieved”. 30.41% of participants completely or partially disagreed that “if correctly undertaken, diet and quitting smoking are generally sufficient to eliminate the residualrisk”. Finally, 18.86% of participants completely or partially disagreed that “pravastatin has an active hepatic metabolism and should not be used in polypharmacy”.
With regard to the treatment to address low HDL-C, the participating physicians indicated the usefulness of 4 proposed treatments (fibrates, statins, omega-3 or nicotinic acid). More than half of participants (67.74%) reported that fibrates were useful or very useful; 65.21% considered omega-3 to be useful or very useful; 64.53% considered that statins were useful or very useful; and finally, 29.45% replied that nicotinic acid was useful or very useful.
Via a Likert scale, participants indicated their degree of agreement according to three statements related to the cardiovascular risk associated with TGs. Some participants (34.99%) completely agreed that TGs are an independent cardiovascular risk factor; 47.62% that TGs are a cardiovascular risk factor when they are associated with other abnormal lipid parameters; and finally, 5.15% that TGs are not a cardiovascular risk “perse”.
Additionally, 94.36% of participants indicated that the following statements were correct: “overall control of the lipid profile in a patient with AD usually needs combined lipid-lowering treatment”; “administering fibrates to patients with type 2 diabetes mellitus reduces macro and microvascular complications, if they already present”; and “the ACCORD study showed that treating AD in diabetic patients conferred a benefit in cardiovascular prevention”.
Finally, the participants indicated which of the following questions was not correct: “controlling overall lipid profile in patients with AD quite often needs combined lipid-lowering treatment”; “fenofibrate is the drug of choice for combination with statins”; “gemfibrozil is the drug with less potential for interactions when used in combination with statins”; “fibrates are the treatment of choice for treating hypertriglyceridemia”. Most (80.95%) indicated that the statement concerning gemfibrozil was not correct.
Clinical casesThree clinical cases were included in the questionnaire, one in the AD diagnosis section and two in the treatment section.
In a 58-year-old man with a diagnosis of metabolic syndrome, what would be the target for lipid control? (Possible choices: LDL-C, non-HDL-C, TGs, and HDL-C).
About half (55.49%) of the participants indicated that the treatment target for this patient would be LDL-C, compared to 20%, 15% and 9.14% who indicated that the treatment target would be non-HDL-C, TGs, and HDL-C, respectively.
How would you manage a patient with slightly elevated LDL-C, low HDL-C, and TGs over 150mg/dl, who cannot achieve lipid control with a statin? (Possible choices: double the dose of statins; add ezetimibe; add nicotinic acid; add a fibrate; add exchange resins).
This clinical case was answered by means of a 5-point Likert scale (1: completely disagree; 2; partially disagree: 3; indifferent: 4; partially disagree: 5; completely agree). A high percentage of participants (90.08%) responded that they completely or partially agreed with treating the patient by adding a fibrate to the statin in order to achieve adequate control.
A 67-year-old man with acute coronary syndrome without ST elevation (NSTE-ACS), DM2, and obesity, receiving treatment with atorvastatin 80mg, has the following lipid profile: LDL-C 66mg/dl, TGs 260mg/dl, and HDL-C 36mg/dl. Please indicate how you would manage this patient. (Possible responses: the objectives have been achieved, so the residual cardiovascular risk has been reduced; the patient has no residual risk and does not need treatment; the patient has AD and a fibrate should be added; a fibrate must never be associated with a statin at these doses).
Most participants (94.46%) indicated that the patient had AD and therefore a fibrate should be added.
DiscussionThe study presented was conducted in order to reflect and describe the management of AD in routine clinical practice. Knowing how it is approached in the field of Primary Care can provide key information to highlight which points require strengthening in order to optimize the management of the disorder.
The study has focused on Primary Care physicians, since they represent the first line of healthcare and are therefore key players in the early detection. The participants involved physicians working in rural, semi-urban and urban areas from all the Spanish autonomous communities. It should be noted that the participants’ professional experience exceeded an average of 25 years (SD: 8.29), and so they are presumably familiar with the management of these patients.
The results of this study reveal that healthcare professionals have access to general recommendations associated with AD management. As could be expected, they are aware of the risk that AD implies for patient's health, as it is associated with a high cardiovascular risk and lipid-origin residual risk.
In terms of detection and diagnosis, most professionals agreed with the published recommendations. The guidelines recommend screening or opportunistic detection for men≥40 years of age, women≥50 years of age, and patients with diseases that predispose to AD. In these patients it is advisable to perform a complete lipid profile and calculate non-HDL-C.10 In line with these recommendations, most participants considered that a complete lipid profile screening was essential to evaluate AD in a patient, by means of TC, TGs, HDL-C, LDL-C, and non-HDL-C. While the proportion is low, it should be highlighted that 3.69% of participants (n=38) indicated that they did not have access to request fractionated TC at their health center. These physicians practiced their profession in 11 different autonomous communities, which shows that this limitation to access to a diagnosis or early detection is not limited to any geographical area. Moreover, it can be noted that the study questionnaire did not include questions evaluating specifically the use of apolipoprotein B (ApoB). Apolipoprotein B is a good predictor of cardiovascular risk; however, it is not routinely used in the Spanish PC setting. Primary care physicians use non-HDL-C since it is a reliable marker, easy to calculate, and does not require additional costs because it can be determined from a standard lipid profile.2–4 This is in line with a report from a consensus meeting of European experts in cardiovascular disease and lipids on November 2014 who stated that achieving target non-HDL-C levels should be key focus of cardiovascular risk management in patients with AD, and that non-HDL-C provides a highly stable measure of cardiovascular risk over time and provides a very good approximation of ApoB levels.14 It is also worth mentioning that the participants use lipoprotein ratios in clinical practice to predict cardiovascular disease in patients with AD, as recommended in the Spanish Clinical Guideline for Detection, Diagnosis and Treatment of AD in Primary Care.2
The overall treatment approach to control AD reported by participants mostly matches the therapeutic algorithms published to date. Thus, most of the guidelines and recommendations consider that lifestyle changes are a key strategy in the treatment of AD,2,11,12 and the study participants also considered this as being so. Regarding the pharmacological approach, the guidelines recommend that the drugs of first choice should be statins, although they are not always able to reduce all cases of AD-associated risk.2,11,15,16 If the patient with AD does not achieve the treatment target with statins, a fibrate should be added, and fenofibrate is the drug of choice.12 This could explain the high percentage of participants (70%) who answered that a patient with AD should be treated with a statin and a fibrate from the start, since the question did not specify lipid levels or another clinical variable. Furthermore, a consensus document on the management of AD of the Spanish Society of Atherosclerosis, published on 2017 recommends the use of statins or statins and fenofibrate according to the cardiovascular risk and the levels of non-HDL-C.17 Patients with high cardiovascular risk and non-HDL ≥130mg/dl should be treated with statins and if the TG and HDL-C objectives are not achieved, a fenofibrate should be added to the therapy.17 This document also recommends that patients with a very high cardiovascular risk or with diabetes and non-HDL-C≥100mg/dl should be treated with a statin and a fenofibrate.17 Therefore, physicians could have assumed that the patient had a high or very high cardiovascular risk. Triple therapy adding nicotinic acid can sometimes be required (although its frequent adverse effects limit its use)12 and at the time at which the study was conducted it was not marketed and could only be obtained as a pharmacy preparation. While it has been published that gemfibrozil is the fibrate with greatest potential for interactions and its association with statins is contraindicated,12 a considerable percentage of participants (around 20%) indicated that they partially or completely agree (16.23% and 2.92%, respectively) that it is suitable to associate with statins.
It could be interesting to correlate in further studies the current consumption of lipid-lowering drugs in Spain with the published recommendations and the study results. The Spanish Agency for Medicines and Medical Devices published a report about the consumption of lipid-lowering drugs in Spain, however, it only included the years from 2000 to 2012.18 During this period, lipid-lowering drugs increased a 442%, being statins the most consumed lipid-lowering drugs (89.3%) in 2012. The consumption of statins increased a 522.6% and fibrates increased a 65%, mainly due to an increase of the consumption of fenofibrates (200%).18
Regarding the clinical cases posed in the questionnaire, it is important to highlight the heterogeneity in the response relating to the lipid target of a patient diagnosed with metabolic syndrome. About half of the participants responded that it would be LDL-C, and the remaining participants answered non-HDL-C (20%), TGs (15%), and HDL-C (9.14%). This discrepancy may be due to the absence of a response that covers the four options or a lack of a single criterion.
Notably, in the treatment approach and follow-up of the patients it is important to distinguish the clinical profile of each of them since AD is associated with various diseases. Hence, some responses will vary in the clinical practice when dealing with each patient on an individual basis.
Concerning the limitations of the study, the questionnaire has not been able to address all aspects related to the management and control of the disorder due to its complexity. One of them is the management of patients with diabetes and their treatment approach. Furthermore, the questionnaire did not include specific questions regarding the control of LDL-C levels or other risk factors since the study tried to focus on how PC physicians proceed once LDL-C objective is achieved. It should also be mentioned that the study did not include questions about the criteria for referring AD patients to specialized units. Neither have data been recorded about the management of treatment adherence or the treatment compliance, which is one of the keys to achieving optimal lipid control.2 Additionally, the study includes only Spanish PC physicians therefore the study results must be interpreted in their context, however, it encourages the need to implement effective measures to improve the management of patients with AD. Lastly, participants were informed at the beginning of the questionnaire that the study was founded by the sponsor, response bias was not expected due to this issue, but it cannot be discarded.
ConclusionsIt can be concluded that, despite the publication of clinical practice guidelines and recommendations, the awareness of healthcare professionals must continue to be raised as regards the importance of early detection and optimal control of the disease to limit its cardiovascular risk. It is important to establish strategies to increase knowledge of AD among health professionals. Likewise, there is a need for a greater number of observational studies that indicate if there are discrepancies between the published recommendations and the daily clinical practice of professionals.
Financial supportThe study has been sponsored by Mylan—Spain.
Conflict of interestMylan EPD funded the development of this manuscript. The authors have no conflict of interest other than the funding of this study. The study participants were informed before answering the questionnaire, that the study was funded by Mylan EPD and that their answers were confidential.
The authors would like to thank Mariona Leria (responsible for pharmacovigilance at Mylan in Spain) and Ana López (assistant of Medical Department at Mylan in Spain) for their assistance and collaboration in the study.