


A caecal appendix within an inguinal hernia, with or without appendicitis, is defined as Amyand's hernia. In 1% of inguinal hernias an appendix without inflammation can be found, however, the prevalence of appendicitis in a hernia sac is only 0.08–0.13%.
Clinical caseMale of 43 years old began two days before admission with pain in the right inguinal region. He was scheduled for surgery due to a complication of a right inguinal hernia. The surgical findings were Amyand's hernia, necrotic spermatic cord, and perforated appendix. Surgical repair was performed with a favourable outcome, and he was discharged on the fourth postoperative day.
DiscussionMost of Amyand's hernia exhibit characteristics of incarcerated or strangulated inguinal hernia. Even acute appendicitis or perforated appendix within the hernia sac does not reflect specific symptoms or signs, therefore, a preoperative clinical diagnosis of Amyand's hernia is difficult to achieve. In our case, the patient had perforated appendicitis, developing necrosis of the spermatic cord. Orchiectomy, appendectomy, and inguinal hernia repair was performed without placing mesh. Due to the controversy on the use of mesh in contaminated abdominal wall defects, it was not indicated here, due to the high risk of wound infection and appendicular fistula.
ConclusionAn extremely rare condition is presented, with a surgical choice that led to a favourable outcome.
Un apéndice cecal dentro de una hernia inguinal, con o sin apendicitis se define como hernia de Amyand. En el 1% de las hernias inguinales se puede encontrar un apéndice sin inflamación; sin embargo, la presencia de apendicitis dentro de un saco herniario se encuentra únicamente en el 0.08–0.13%.
Caso clínicoVarón de 43 años de edad, inicia padecimiento 2 días previos a su ingreso presentando dolor en región inguinal derecha. Se programa para plastia inguinal derecha por hernia inguinal complicada, encontrándose en hallazgos transoperatorios: hernia de Amyand, con cordón espermático necrosado y, apéndice perforado. Se realiza corrección quirúrgica, con evolución clínica y con egreso hospitalario, al cuarto día del postoperatorio.
DiscusiónLa mayoría presentan características de hernia inguinal incarcerada o estrangulada e incluso, una apendicitis aguda o perforación del apéndice dentro del saco herniario que no refleja sintomatología o signos específicos; debido a esto es complicado alcanzar un diagnóstico clínico de hernia de Amyand en el preoperatorio. En nuestro caso, el paciente presentó apendicitis perforada, con necrosis del cordón espermático, por lo que se le realizó: orquiectomía, apendicectomía y, reparación primaria de la hernia inguinal sin colocar malla, puesto que existe controversia de su uso en defectos de pared abdominal contaminada, por el riesgo de infección de la herida y, de fístula del muñón apendicular.
ConclusiónPresentamos una afección en una variedad extremadamente rara, con tratamiento quirúrgico y evolución favorable.
A caecal appendix inside an inguinal hernia, with or without appendicitis is defined as Amyand's hernia. According to Thomas et al. finding an non-inflamed caecal appendix inside the peritoneal sac of an indirect inguinal hernia was first described by Garangeot in 1731.1 Claudius Amyand, performed the first successful appendicectomy in 1735 on an 11-year old patient presenting with an inflamed appendix, perforated inside an inguinal hernia sac.2,3
A non-inflamed appendix can be found in 1% of all inguinal hernias. However, the presence of appendicitis inside a hernia sac is only found in 0.08%.4
Clinical caseA 43 years-old male patient who had begun to present pain in the right inguinal region 2 days prior to his admission, and the presence of an inguinal hernia on the same side. He attended the emergency department, and was assessed by the general surgery unit who indicated surgical intervention owing to the preoperative diagnosis of complicated right inguinal hernia.
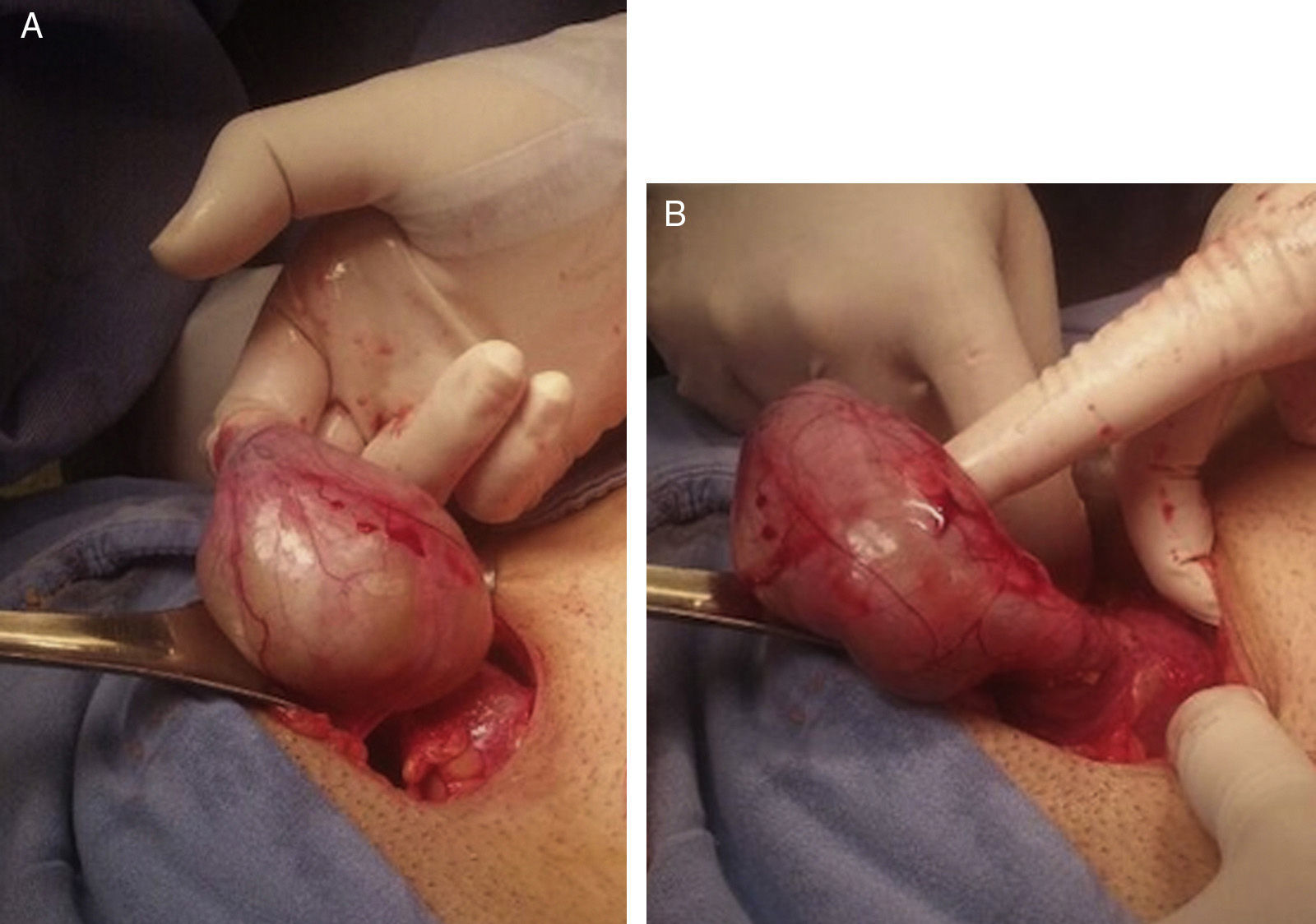
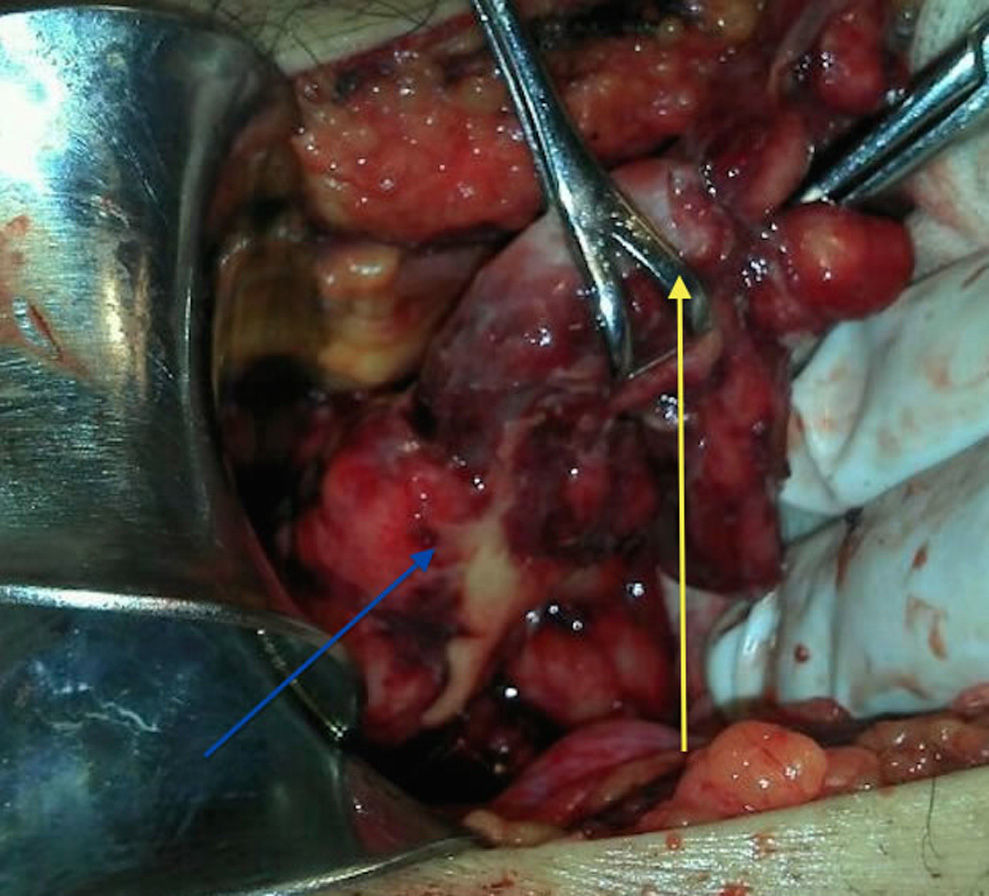
A surgical procedure was carried out using an approach for an inguinal hernia and the perforated caecal appendix was identified at its tip with abundant pus and necrosis of the spermatic cord, therefore a right orchidectomy, appendicectomy and plasty of the defect in the inguinal canal using Shouldice's technique not using mesh, closing the skin with separate stitches and leaving a Penrose-type drain (Figs. 1A and B, and 2).
 Presence of the caecal appendix inside the hernia sac.")
.")
The patient progressed well, the Amyand's hernia was resolved with surgical treatment and the patient was discharged on the fourth post-operative day, without complications.
DiscussionThe probability of a person suffering acute apendicitis is 8%, the incidence of non-inflamed appendix inside an inguinal hernia is around 1%. However, the incidence of acute appendicitis inside the hernia sac is even less common, and occurs in approximately 0.08–0.13%.4,5 Most reported cases present characteristics of incarcerated or strangulated inguinal hernia. Even an acute appendicitis or perforated appendix inside the hernia sac does not show specific signs and symptoms. For these reasons it is difficult to reach a clinical diagnosis of Amyand's hernia preoperatively.3 Diagnosis takes place during the transoperative period, when surgical exploration is undertaken due to clinical signs of a complicated inguinal hernia.
Surgical treatment is based on the characteristics that this disease presents, Losanoff and Basson propose a classification of 4 types in which they outline the treatment for each:
- –
Type 1: normal appendix inside an inguinal hernia; surgical treatment consists of: reduction of the hernia, repair with mesh and appendicectomy in young patients.
- –
Type 2: acute appendicitis inside an inguinal hernia, with no abdominal sepsis; surgical treatment should be appendicectomy through the hernia and primary repair with no mesh.
- –
Type 3: acute appendicitis inside an inguinal hernia, abdominal wall or peritoneal sepsis; surgical treatment consists of: laparotomy, appendicectomy, and primary repair of the hernia with no mesh.
- –
Type 4: acute appendicitis inside an inguinal hernia, associated or otherwise with abdominal disease; in this type surgical treatment should be for the hernia as in types 1–3 and, if there is abdominal disease it is essential to investigate the aetiology and only thus will it be possible to determine appropriate surgical treatment.6
In our case, the patient presented clinical signs compatible with a complicated inguinal hernia, this was why an approach for inguinal plasty was used, and as it was accompanied by complicated appendicitis it was decided to use the same incision to resolve it. A plasty without mesh was undertaken using Shoudice's technique, as the presents of purulent material might compromise the mesh (there is still controversy as to its use), due to the potential risk of wound infection and formation of a fistula of the appendix stump.6–8
ConclusionTreatment of Amyand's hernia should be on an individual basis as it depends on the condition of the caecal appendix, in order to avoid the high risk of infection when it is repaired.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: García-Cano E, Martínez-Gasperin J, Rosales-Pelaez C, Hernández-Zamora V, Montiel-Jarquín JA, Franco-Cravioto F. Hernia de Amyand y apendicitis complicada; presentación de un caso y elección de tratamiento quirúrgico. Cirugía y Cirujanos. 2016;84:54–57.