






Dengue is one of the principal vector-transmitted diseases leading to important public health problems in Mexico and Latin America. On the American continent this disease has been reported mostly in adults, which contrasts with Asian countries where pediatric dengue is more prominent. During the last decade a shift towards pediatric dengue has been reported in various countries of the American continent. This review, elaborated from data published by the Mexican Ministry of Health, focuses on dengue in Mexico during the last three decades, showing that during the last decade dengue fever and dengue hemorrhagic fever has begun to shift towards a juvenile and pediatric population.
El dengue es una de las principales enfermedades transmitidas por vector. En la última década se convirtió en uno de los problemas de salud pública más importantes de México y América Latina. En el continente americano el dengue es considerado predominantemente un padecimiento de adultos, lo cual contrasta con los reportes de países asiáticos que consideran el dengue como una enfermedad principalmente pediátrica. Durante la última década se ha reportado el incremento de dengue juvenil y pediátrico en varios países de América. En la presente revisión, elaborada a partir de datos publicados por la Secretaría de Salud, se analiza la tendencia de aumento en la incidencia de dengue en la población juvenil e infantil de México durante los últimos 10 años.
1. Introduction
During the last decades, dengue fever (DF) and hemorrhagic dengue fever (HDF) affected mostly adults of reproductive age in endemic areas of the Americas. In contrast, in Asia they have been considered as pediatric diseases that primarily affect children <15 years of age.1-3 In Mexico, as in the rest of the Americas, dengue has been reported in persons of all ages, yet during the last 10 years the risk of dengue has increased especially in children and juveniles.
Dengue is an acute febrile disease caused by the dengue virus (DENV). This virus belongs to the genus Flavivirus and consists of four serotypes (DENV-1 to DENV-4) that regularly circulate in endemic and hyperendemic tropical areas.4,5 It is transmitted by the mosquito Aedes aegypti. Currently, it is the most important vector-borne disease worldwide in terms of morbidity, mortality and economic importance.6,7 According to the WHO, nearly half of the population in the tropics is at risk, the most affected regions being those with the greatest needs of basic health services.8
In recent years, the incidence of dengue has alarmingly increased worldwide. It is estimated that in the present decade there have been 50 million annual cases of DF, of which 500,000 are HDF with greater involvement of the adult population.8 The incidence of dengue is similar in Southeast Asia and tropical America with the presence of all four viral serotypes. The serotypes have an Asian origin, yet they are endemic on both continents, showing marked differences in the severity of the disease and the population at risk between the two continents.9,10 In a study by Halstead in 2006 where epidemic quinquennial periods of dengue were compared in both regions, it was reported that 1.16 million cases of HDF occurred in southeast Asia primarily in children, whereas in the Americas there were 2.8 million cases of dengue, especially in adults, and only 65,000 cases of HDF. However, in the last 10 years there has been an increase in morbidity and mortality from dengue in children and juveniles in some American countries.11 Dengue in children and juveniles is particularly risky because of the clinical features and early complications associated with a rapid and fulminant disease evolution with involvement of organs such as the myocardium and liver, leading to a fatal outcome.12
2. Dengue as a problem of children in America
During the past 10 years, countries in Central and South America, where the disease had been endemic for three decades, have reported a changing pattern of the population at risk for dengue.11 During the epidemics of 2000 and 2002 in El Salvador, it was found that mainly children between 3 and 4 years of age had an increased risk of HDF and dengue shock syndrome (DSS) in addition to increased morbidity and mortality.13 Similar situations were observed in a study conducted in Nicaragua in 2001, where cases of DF and HDF were reported mainly in infants of 4-9 months and children of 5-9 years of age and where second dengue infections increased the risk of severity in children.14 In Costa Rica, in 2007, 50% of deaths from HDF/DSS occurred in children <3 years of age (4 cases).15 In Brazil, the rate of hospitalizations for HDF in children <15 years of age increased from 9.5% in 1998 to 46.2% in 2007 and 2008.16 In an epidemic outbreak in Rio de Janeiro, 88% of HDF deaths occurred in children <15 years of age.17
Similarly, in 2010 the University of San Carlos in Guatemala reported that 36.67% of the cases with HDF occurred in patients between 11 and 20 years of age.18 In Colombia an increased mortality from dengue was recently reported in children aged 1-5 years as compared to infants <1 year and children >5 years of age.19
Mexico has been no exception. In 2002, Navarrete et al. reported for the first time an increasing trend of fever in children and juveniles that were attended at the Mexican Institute of Social Security (IMSS).20 This background prompted us to review and analyze the population affected by dengue in Mexico during the past three decades, based on data published by the Ministry of Health (CENAPRECE).
3. Dengue in Mexico
Upon its reintroduction to Mexico in 1978, after having been eradicated for 12 years, dengue became a public health problem predominantly in the adult population, with the population at risk lacking basic health services.6,8,21 From 1980 to 2011, three periods of the disease have been registered, each lasting approximately 10 years, with a major outbreak occurring in each decade. During the decade of 1990-1999, the highest incidence rate was in the population aged 25-44 years, showing an average annual rate of 30.7 deaths,* whereas in the decade 2000-2009 the highest incidence rate shifted to the population aged 15-24 years, with an average annual rate of 51.31 deaths.* During the latest period (2000-2010) the incidence of HDF increased dramatically and a change in the population at risk became evident, showing a health problem affecting mainly children and youths.
In Figure 1, the annual incidence of DF is shown in the Mexican population according to age groups in the last two decades, 1990-1999 and 2000-2010. It can be observed that during the first decade, the highest incidence of dengue cases corresponded to the adult (24-44 years) and older (45-64 years) population (Fig. 1A), whereas during the last decade, specifically after 2005, the incidence of DF increased in the juvenile population (15-24 years) and children (5-14 years), a phenomenon that has persisted until 2010 (Fig. 1B). Beginning in 2002, the incidence of HDF increased dramatically, with an average annual rate of 17.31 in the juvenile population, a change that has become more evident during the past 5 years. During 2007 and 2008 the highest incidence was recorded in juveniles followed by children (29* and 21*, respectively), according to the infantil population (12.6* and 8.7*, respectively) (Fig. 2).
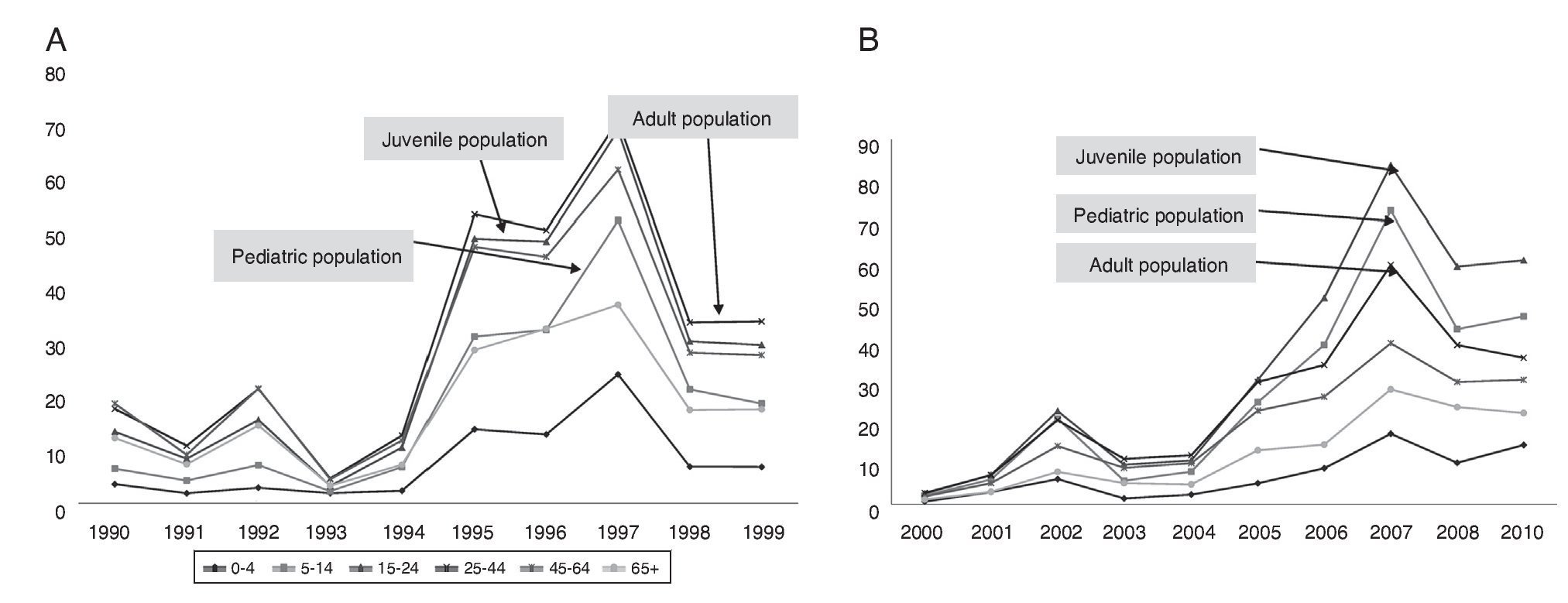
Figure 1 Annual incidence of dengue fever (DF) in the Mexican population by age range. (A) 1990-1999. (B) 2000-2010 (year 2009 is not included because of a discrepancy in the number of cases in epidemiological bulletins). Source: CENAPRECE/Morbidity Yearbooks 1990-2009.
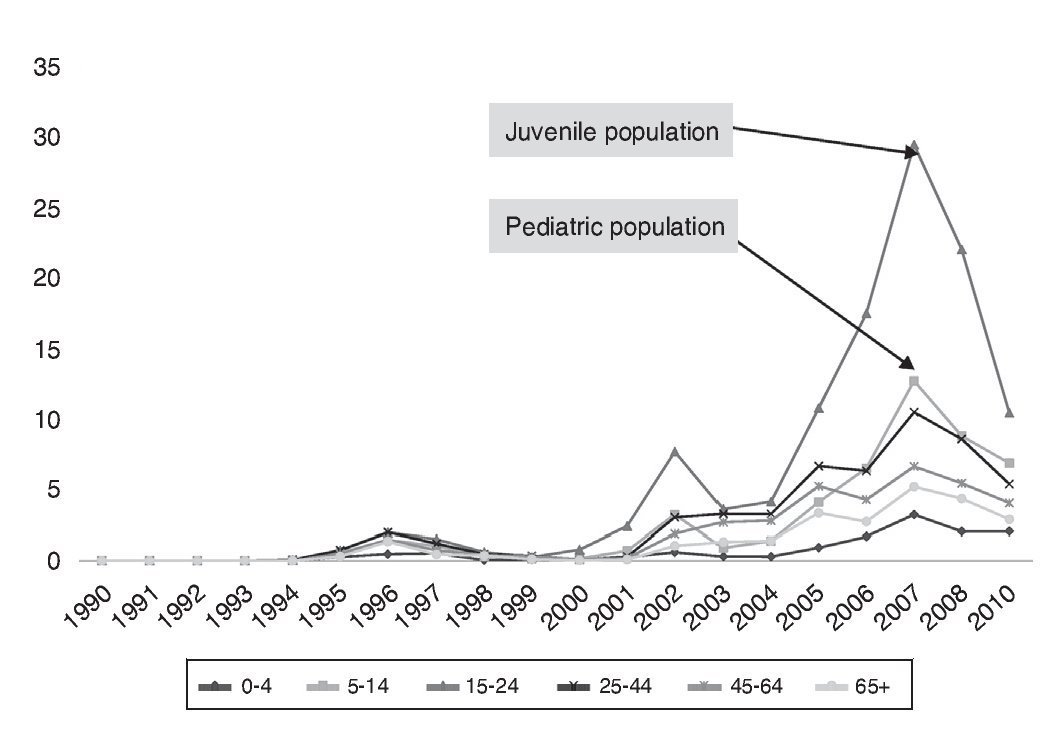
Figure 2 Annual incidence of hemorrhagic dengue fever (HDF) in the Mexican population by age range for the period 1990-2010 (year 2009 is not included because of a discrepancy in the number of cases in epidemiological bulletins). Source: CENAPRECE/Morbidity Yearbooks 1990-2009.
This trend of change in the population at risk is uniform in all states reporting dengue. Figure 3 shows nine of the 22 states of Mexico with the highest incidence of DF and HDF reported between the years 2000 and 2010. An increase is observed in the number of dengue cases in children followed by the juvenile population, albeit a higher incidence was recorded in the latter. Specifically the states of Colima, Guerrero, Michoacán and Oaxaca showed more cases and increased risk of DF (Fig. 3A) and HDF (Fig. 3B) in children.
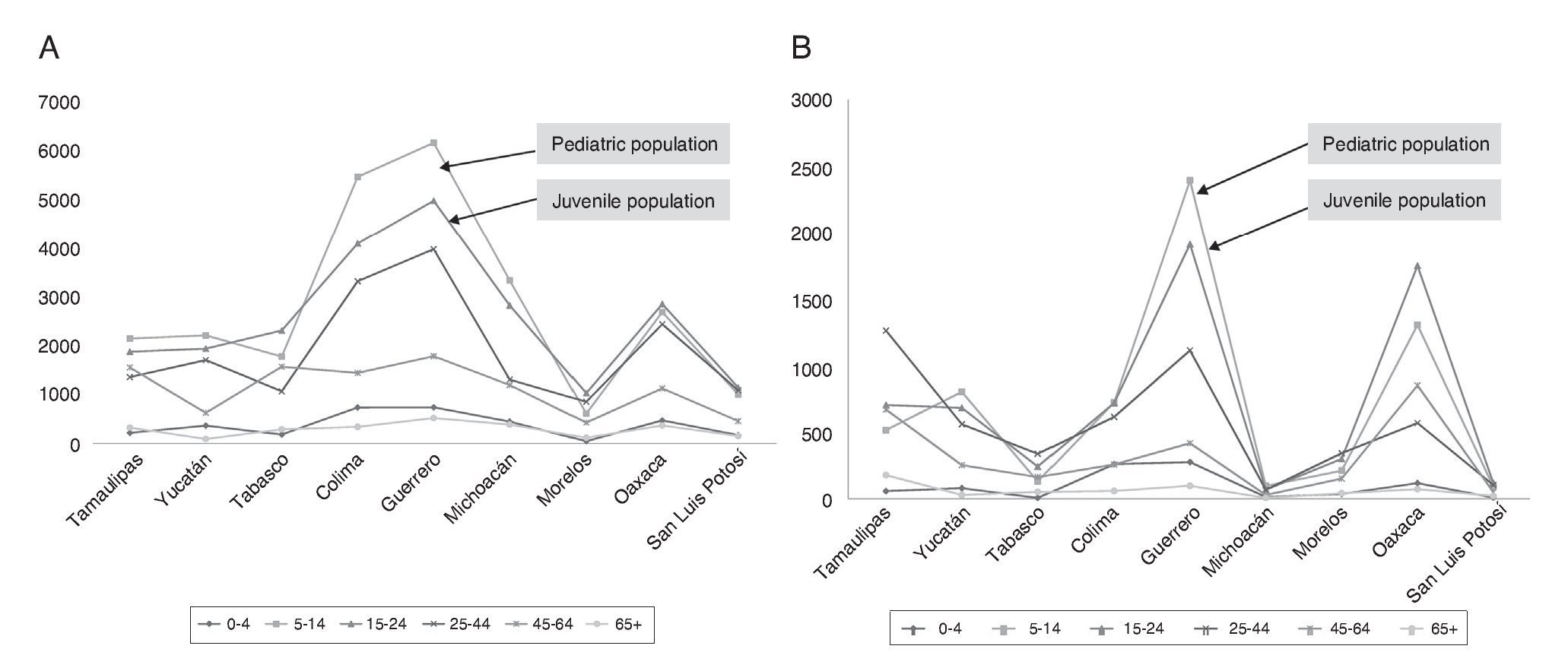
Figure 3 States in Mexico with the highest number of dengue cases in children and juveniles during the period 2000-2010. (A) Total number of cases of dengue fever (DF). (B) Total cases of hemorrhagic dengue fever (HDF) (year 2009 is not included because of a discrepancy in the number of cas es in epidemiological bulletins). Source: CENAPRECE/Morbidity Yearbooks 1990-2009.
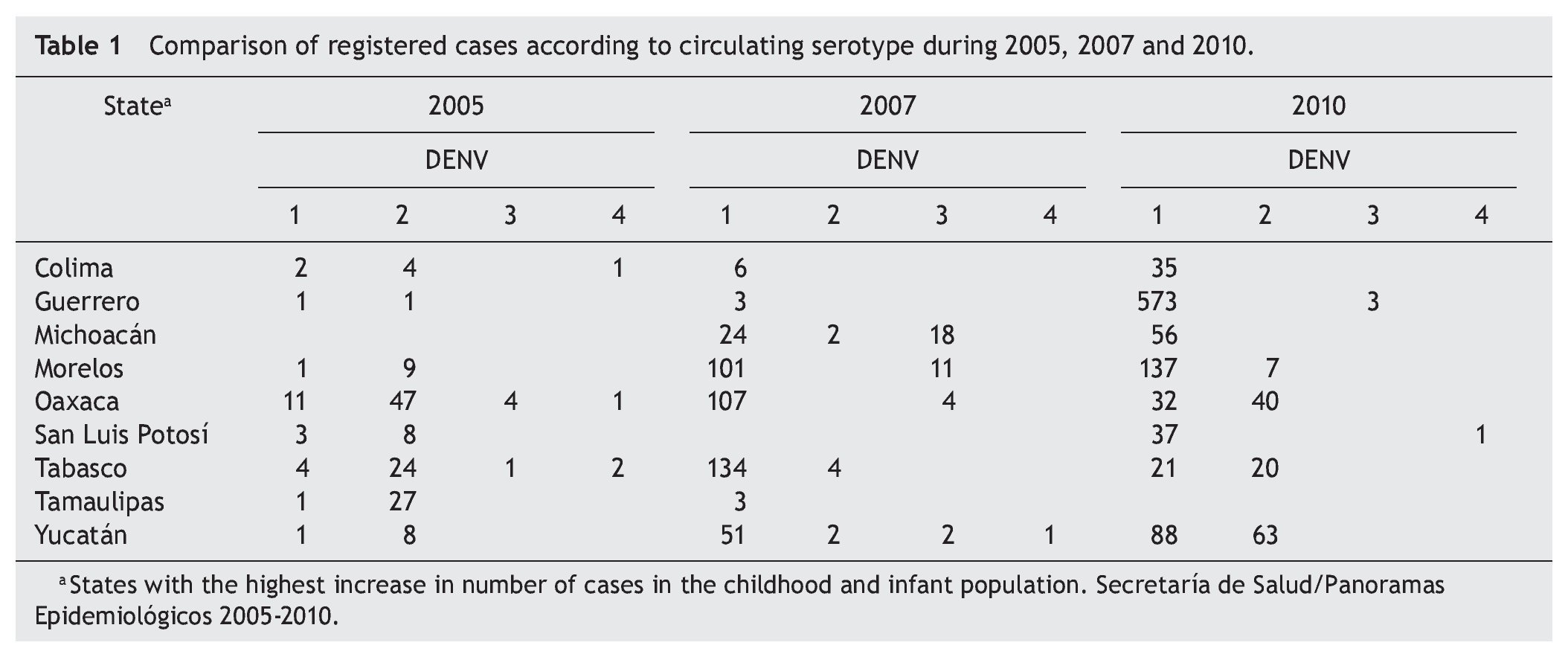
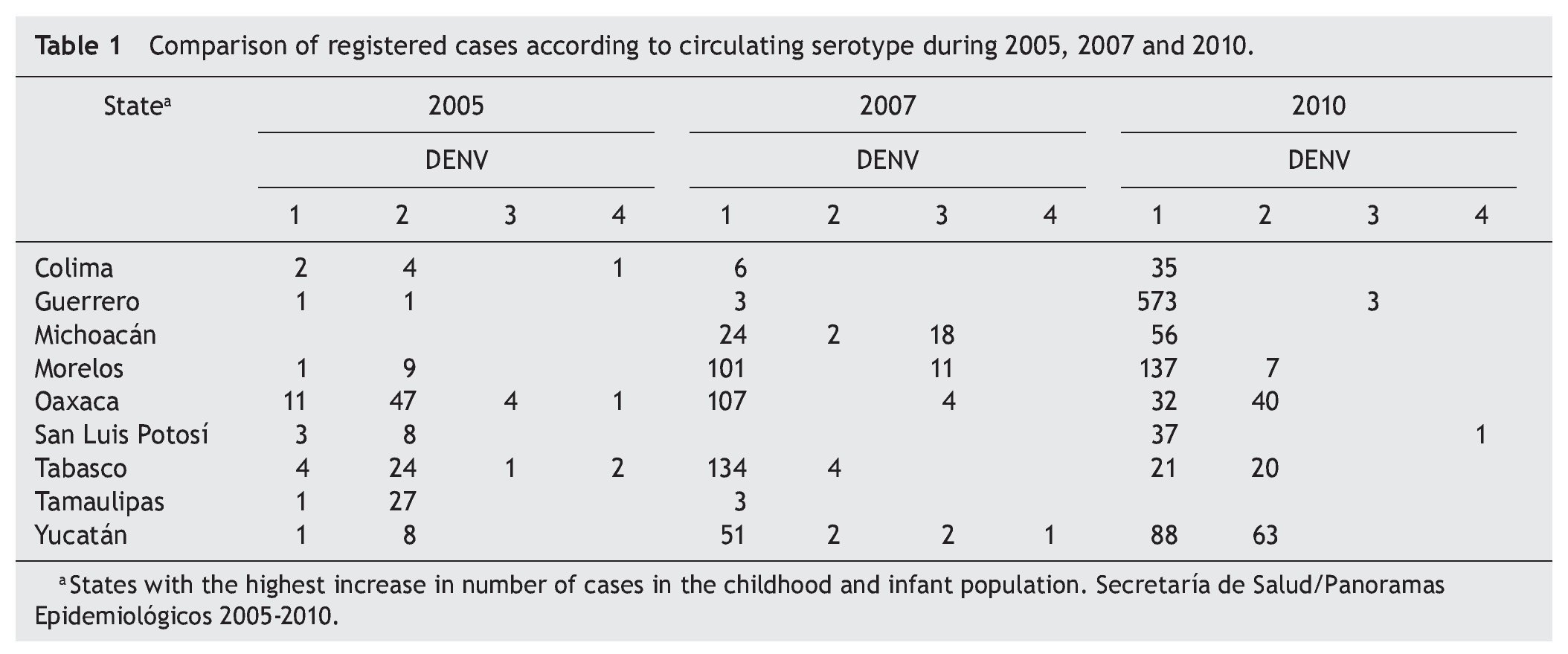
In recent years, a feature observed in the Mexican states that reported dengue is the increased circulation, disappearance and reintroduction of certain dengue virus serotypes, which has revealed an association between circulating serotypes and outbreaks. Table 1 shows a comparison between the number of recorded cases and the circulating dengue virus serotypes in the nine states that reported an increase in the number of juveniles and children during the years of highest incidence of dengue (2005, 2007 and 2010). A displacement of DENV-2 by DENV-1 was observed during the years 2007 and 2010. Although each of the outbreaks was associated with different serotypes, the cause of the increasing trend of the disease in juveniles and children remains unresolved.
An attempt was made to correlate the change in the epidemiological trend of dengue with the replacement of the native American viral populations by other more virulent ones, following a similar pattern of epidemics observed for decades in Southeast Asia. So far, however, no conclusive evidence has been found.22-24 Figure 4 shows the movement, displacement, replacement and reintroduction of serotypes that occurred in Mexico between 1995 and 2011.
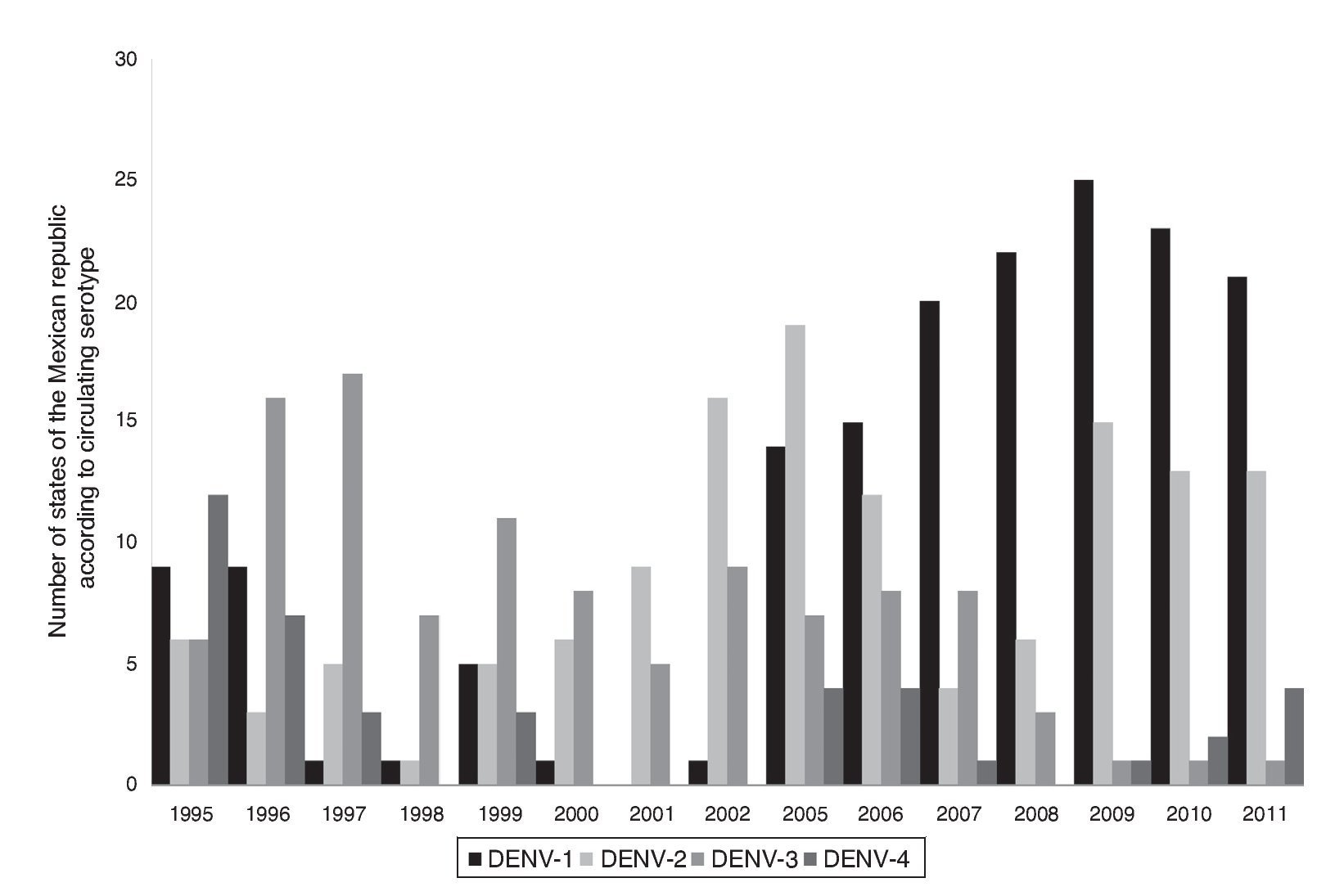
Figure 4 Number Annual circulation virus serotypes in Mexico from 1995 to 2011. Source: Ministry of Health (Mexico).
Studies performed in Central American countries have assessed potential variables that could explain the change of the population at risk. In El Salvador the nutritional status was analyzed as a possible risk factor for dengue, yet no significant relationship was found.25 However, in Venezuela and Brazil the climate variability was found to be an important element in dengue epidemiology.26-28
It is noteworthy that whereas in the Americas an increase of dengue is being observed in children and juveniles, the opposite phenomenon is occurring in Asian countries such as Taiwan, Bangkok and Vietnam, where dengue has shifted from being a pediatric illness to a disease more frequent in young adults.29-33
This analysis has allowed us to observe an epidemiological shift in DF and HDF occurring in Mexico during the last 10 years, which is in accordance with the increased incidence of the disease reported in children and youths in recent years in other Latin American countries. Among the risk factors that have been proposed are the following: environmental factors such as climate variability, circulation of different serotypes, genetics of viral populations and genetic characteristics of the population. The increase of HDF and DF in juveniles and children is particularly alarming because of the fulminant evolution associated with early complications. Data found in this study reflect the need for close monitoring and a multifactorial analysis to identify risk factors that are driving this age shift in the affected population of Mexico.
Conflict of interest
The authors declare no conflict of interest of any nature.
* Per 100,000 population.
Received 16 January 2014;
accepted 27 March 2014
* Corresponding author.
E-mail: becker@unam.mx (I. Becker).