




Background: Intestinal duplication cysts are rare abnormalities that occur primarily during the perinatal period and may cause problems for feeding and/or breathing. Sublingual intestinal duplication cysts can present either gastrointestinal epithelium or respiratory or both; the latter two cases are called choristomas.
Case report: We describe a 10-month-old infant who presented a sublingual cystic mass at birth. Total successful transoral resection and reconstruction of the tongue was performed in planes. The surgical specimen was a brown cystic structure of mucoid content with dimensions of 23 x 17 x 11 mm. The cyst lining consists of gastric mucosa with foveolar epithelium and glands composed of parietal and chief cells.
Conclusions: The intestinal duplication cyst is an extremely rare entity. The surgical approach is effective and curative with minimal morbidity and mortality and without recurrence in follow-up.
Introducción: Los quistes de duplicación intestinal son anormalidades poco frecuentes que se presentan principalmente en el período perinatal, y pueden causar problemas respiratorios y para la alimentación. Los quistes sublinguales de duplicación intestinal pueden presentar solo epitelio del aparato digestivo, del respiratorio o de ambos. En los dos últimos casos se denominan coristomas.
Caso clínico: Se describe un caso de un paciente de 10 meses de edad que presentó una masa quística sublingual desde el nacimiento. Se realizó la resección total con abordaje transoral y la reconstrucción de la lengua en planos. La pieza quirúrgica resultó una estructura quística de contenido mucoide, de 23 x 17 x 11 mm y color marrón. El revestimiento del quiste estaba formado por mucosa gástrica, con epitelio foveolar y glándulas formadas por células parietales y principales.
Conclusiones: El quiste de duplicación intestinal es una entidad extremadamente rara. El abordaje quirúrgico es eficaz y curativo con mínima morbilidad y mortalidad, sin recurrencia en su seguimiento.
1. Introduction
Enteric duplication cysts are mainly found in the small intestine.1 Their frequency of presentation in the anterior tongue occurs in only 0.3% of cases.2 They are a challenging issue for the pediatrician and the surgeon as the majority of the lesions are found on the ventral part of the anterior tongue and extend towards the floor of the mouth.
The cysts can be detected before or after birth.3 Some causes are asymptomatic;4others present difficulty breathing and require emergency surgical intervention.5 For this reason it is necessary to carry out the diagnosis during the prenatal examination, which allows for preparation of the personnel and team necessary for the adequate management of the newborn during labor. Because of the possibility of airway obstruction during labor, preparation for an immediate tracheotomy is very important when oral intubation is impossible6 or when an intrapartum ex-utero surgery is required (EXIT).7
Some patients do not have respiratory difficulty despite the size of the mass in the anterior tongue when the diameter varies between 1.05-2.04 cm.8 Other cysts can measure up to 6.5 cm in diameter and, because of their size, are considered to be giant. They can cause feeding difficulties and partial airway obstruction during sleep.9
The case we report had many aspects of the diagnosis and surgical treatment of this unusual lesion. A review of the literature was also carried out in regard to the differential diagnosis and histopathological findings.
2. Clinical case
We present the case of a male infant with the following history. He was the product of a first pregnancy of a 21-year-old mother. Because of changes in fetal heart rhythm, a cesarean section was scheduled at 30 weeks gestation. At birth the baby cried and breathed. Apgar was 6-7, weight 1470 g and length 41 cm. The infant remained hospitalized for 1 month. He was discharged with a weight of 1940 g and length of 46 cm. The infant was breast fed.
On his first examination at 1 month of age, he weighed 2100 g with a length of 46 cm. There was a painless, hard cystic inflammation found that occupied the left side of the tongue ∼2 cm in diameter. A right hydrocele and bilateral inguinal hernia were also found. Surgery of the lingual cyst was suggested, but the family decided to wait. At 4 months of age a bilateral inguinal hernioplasty was done at another institution. From 6 months of age the patient presented difficulty in accepting a bottle and cried frequently. He returned at 9 months of age with weight of 8 kg and length of 68 cm. The tumor had increased ∼2.3 cm in diameter. At 10 months and under general anesthesia with tracheal intubation, total cyst resection was carried out (Fig. 1). The cyst was ovoid, irregular in shape with a diameter of 2.3 cm. Tongue reconstruction in planes was done with absorbable material. The result was very satisfactory and there was minimal bleeding (<5 cc). The postoperative course was excellent. From the following day oral feeding was begun as tolerated, first with glucose solution and then with milk formula. He was discharged at 28 h of the surgical intervention.
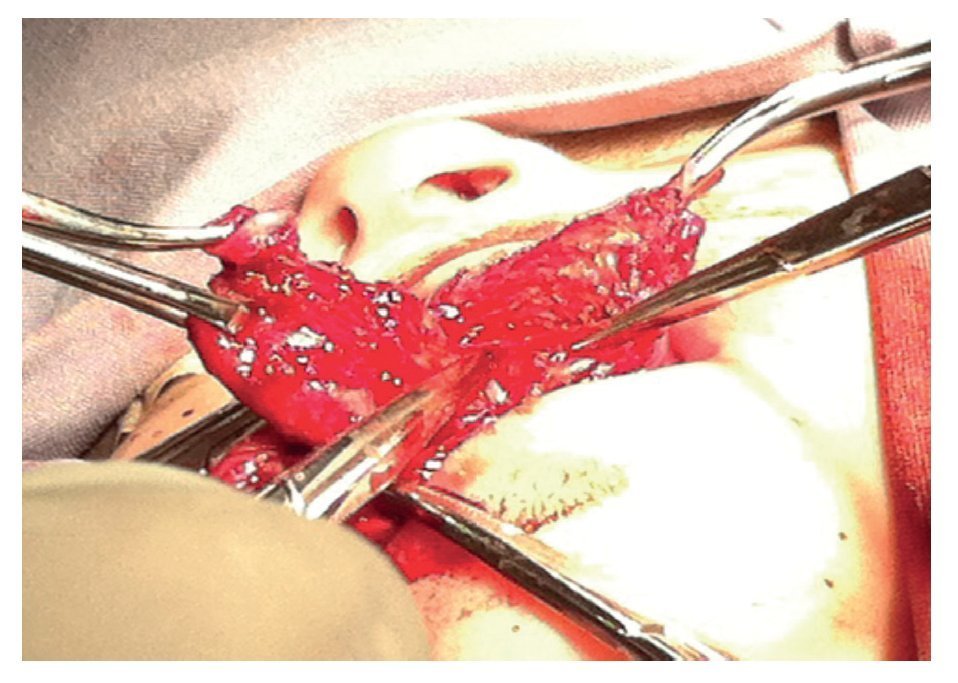
Figura 1 Intraoperative dissection showing a well-defined ovoid, cystic mass, irregular in shape and with a diameter of 2.3 cm in the floor of the mouth.
The surgical specimen was a cystic structure of 2.3 x 1.7 x 1.1 cm with an irregular surface and brown color. On serial cuts a 0.8-cm cavity was noted with wall thickness of 0.3 cm. The epithelial lining consisted of gastric mucosa with foveolar epithelium and glands lined by parietal and main cells. The surrounding stroma showed some mature lymphocytes. This epithelium alternated with mature stratified simple squamous epithelium and mucoserous glands. The wall was composed of circular and longitudinal smooth muscle. The histopathological report was cystic duplication of the anterior intestine (Fig. 2).
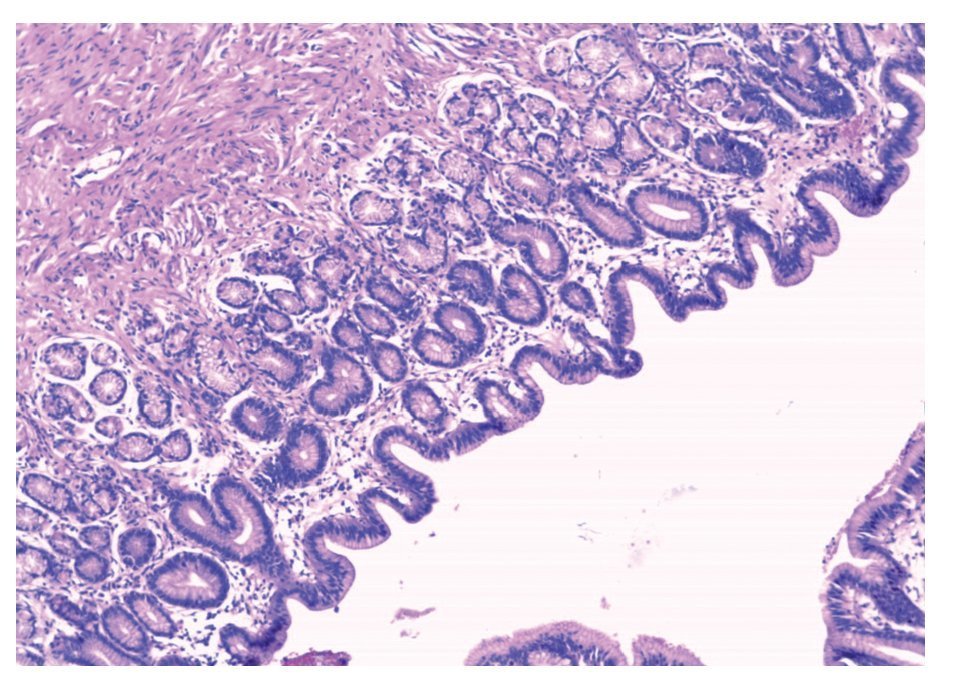
Figura 2 Cystic wall where gastric mucosa is observed with glands lined by parietal and chief cells (HE, 10x).
The patient was examined 1 week later. Suction and swallowing were adequate and painless. The aesthetic appearance was satisfactory. The patient is currently 13 months of age and his growth and development are age appropriate.
3. Discussion
When faced with a newborn with the presence of a mass in the anterior two-thirds of the tongue, various possible differential diagnoses must be taken into consideration such as a ranula, lymphangioma, hemangioma, dermoid cyst, epidermoid cyst, neurofibroma, teratoma, thyroglossal duct cyst, muco cele, lymphoepithelial cyst, cystic hygromas or lingual choris toma.10-14 Choristoma, unlike the anterior intestinal duplication, is lined by epithelium from the gastrointestinal and respiratory tracts, such as in the cases reported by Burkat et al.15 Lingual cysts can present themselves throughout the length of the gastrointestinal tract from the esophagus to the colon16 and in other organs such as the gallbladder, pancreas, lungs, larynx and bladder.17 Enteric duplication cysts are rare in the tongue, and its lumen can rarely communicate with the lumen of the gastrointestinal tract. They frequently exist as separate cysts or tubular lesions that resemble a segment of normal intestine.
Diagnostic criteria have been described for enteric duplication cysts that include the presence of a smooth muscle cover, the cyst as an addition to part of the gastrointestinal tract and the presence of mucosal lining of the gastrointestinal tract, which is a gastric variety.18 This heterotopic gastric mucosa can become ulcerated in some cases and, in other cases, more than one type of mucosa is found, such as in this case.
These cysts are a heterogeneous group of lesions that share morphological findings, perhaps with a different pathogenesis.2 It is believed that these cysts arise from endodermic cells that become trapped during fusion of the lateral lingual protuberance (from distal lingual bud) and the lateral tuberculum impar (medial lingual bud) in an embryo of 3.4 mm.2,9,19 They are cells derived from the stomodeum20 or ectodermic invagination of the embryo, from where the mouth and pharynx are formed. These pluripotent cells can differentiate into various types of epithelium including gastric, intestinal, colon, or even respiratory.21 The approach of study in children with a lingual mass includes ultrasound, computed tomography and nuclear magnetic resonance.22 Treatment consists of complete surgical resection.4 Only one report in the literature describes recurrence where an incomplete resection of the cyst had been carried out.
In the differential diagnosis of a lingual cystic mass, in each child an anterior enteric duplication cyst should be taken into consideration and early surgical approach is important to avoid future alterations in feeding, which could result in lack of weight gain and height as well as other possible respiratory disorders. Duplication of foregut cyst should be considered and early surgical approach is very important to avoid future feeding alterations, which may result in lack of increase in weight and height as well as possible respiratory disorders.
Conflict of interest
The authors declare no conflict of interest of any nature.
Received 8 April 2014;
accepted 15 April 2014
* Corresponding author.
E-mail: memomilan@yahoo.com.mx (J.G. MiIán-Montenegro).