





A survey conducted by the European Board of Ophthalmology (EBO) revealed significant differences in the surgical training of the ophthalmology residents in Europe, including a disparity between the sexes and a variation in the experience on cataract surgery (CC) between them. This study is about the Spanish sub-cohort of the survey, and its objective is to present and analyse the peculiarities of ophthalmology training in Spain within the European context, as well as discussing ways to harmonise and improve that training throughout the EU.
MethodsWe analyse data of the Spanish participants in the EBO exams, defining subgroups by the Autonomous Communities existing in Spain.
Results93 of 135 requested participants (68.9%) responded. A 60.2% passed the EBO exam between 2021 and 2022, being mostly women (65.59%) aged 31 years old on average. The 91.4% were right-handed, coming from 13 of the 17 Spanish autonomous communities, although mostly from the Community of Valencia, Madrid and Catalonia. Respectively, 16.1%, 3.2% and 8.7% of the respondents said they have completed 10 or more training sessions on animal eyes, synthetic eyes and through the virtual reality simulator. This training was correlated with greater self-confidence in the management of a posterior capsular tear during surgery (p .025). All respondents manifested to have already performed stages of the CC. The average number of operations reported was 181.6 with regional disparities. A significant difference is observed between the sexes against women (−28.3%, p 0.03).
DiscussionOphthalmologists in Spain, much more than other European countries, have greater opportunities for surgical training, with surgical procedures during the residency, that nearly triples those made by the others. Spanish women refer, like their European colleagues, to be in disadvantage in learning opportunities about cataract surgery. The Simulation Based Medical Education (SBME) allows to respond to the training deficit and complements the training on the patient. Although we demonstrate a significant correlation between the number of procedures carried out and self-confidence to operate simple cases, the SBME would be a complementary tool in self-confidence in front of a complication like capsular rupture.
ConclusionSpain massively adopts the model named by us "surgery for all”, despite the underrepresentation of women in this area, emphasising a need for cultural change that the SBME could facilitate.
Una encuesta del European Board of Ophthalmology (EBO) reveló diferencias significativas en la formación quirúrgica de los residentes en oftalmología en Europa, incluyendo una disparidad entre los sexos y variaciones en la experiencia en cirugía de catarata (CC) entre ellos. Este estudio es sobre la muestra española de la encuesta, su objetivo es presentar y analizar las peculiaridades de la formación oftalmológica en España dentro del contexto europeo, así como discutir formas de armonizar y mejorar esa formación en toda UE.
MétodosAnalizamos datos de participantes españoles en los exámenes del EBO, definiendo subgrupos por Comunidades Autónomas.
Resultados93 de 135 encuestados (68,9%) respondieron el cuestionario. El 60,2% había hecho el examen EBO entre 2021−2022, siendo la mayoría mujeres (65,59%) con edad media de 31 años. El 91,4% eran diestros, procedentes de 13 de las 17 comunidades autónomas españolas, aunque mayoritariamente de la Comunidad Valenciana, Comunidad de Madrid y Cataluña. El 16,1%, el 3,2% y el 8,7% de los encuestados dijeron haber realizado 10 o más sesiones de formación sobre ojos de animales, ojos sintéticos y con simulador de realidad virtual respectivamente. Esta formación se correlacionó con una mayor autoconfianza en la solución de rotura capsular posterior durante la cirugía (p .025). Todos los encuestados afirmaron haber realizado ya etapas de la CC. El número medio de operaciones reportado fue de 181,6 con disparidades regionales. Se observa una diferencia significativa entre los sexos en contra de las mujeres (−28.3%, p 0.03).
DiscusiónLos oftalmólogos en España, mucho más que en otros países europeos, tienen mayores oportunidades de formación quirúrgica con un número de cirugías durante la residencia que casi triplica la de los otros. Las mujeres españolas refieren, al igual que sus colegas de otros países de la UE, estar en desventaja en oportunidades de aprendizaje de la cirugía de cataratas. La Simulation Based Medical Education (SBME) permite responder al déficit de formación y complementa la formación sobre pacientes. Aunque demostramos correlación significativa entre el número de procedimientos realizados y la confianza en sí mismo para operar casos simples, la SBME sería una herramienta complementaria en la autoconfianza ante el enfoque de complicaciones como la rotura capsular.
ConclusiónEspaña adopta masivamente el modelo que hemos llamado de “cirugía para todos”, a pesar de la subrepresentación de las mujeres en este ámbito, subrayando una necesidad de cambio cultural que la SBME podría facilitar.
Ophthalmology is a medical-surgical specialty in constant evolution. Cataract is the most performed ophthalmologic intervention in Spain and in the world and requires not only skills but also progressive and constant knowledge. Phacoemulsification has become the technique par excellence in recent decades.1
Several surveys highlighted differences within the European Union in terms of surgical training.2,3 In a context, therefore, of great disparities between member countries of the European Union of Medical Specialists (UEMS), a telematic survey of the European Board of Ophthalmology (EBO) conducted between 2018 and 2022, addressed to young participants of the EBO examination, received replies from 821 colleagues. Its purpose was to assess the quality of their surgical training, as well as their personal impression of the implementation of their training since its inception.2
Some results were very revealing: there was a clear gender difference, with women having performed significantly fewer procedures and reporting less confidence in themselves than their male colleagues. While the average European resident had performed 80.7 complete procedures by the end of their training, a significant number of them (210, 25%) said they had never performed a single cataract surgery step on patients. This diversity reveals two antagonistic models of surgical training: one following the west and south of the continent, where future specialists are trained in cataract surgery, and a model from the north and east of the continent, where surgical training is performed after residency. The results of data collection at the European level have recently been published, but no detailed regional analysis has yet been done within each country.2
Our study details the results of the Spanish sample and places the national experience in this broad European context. The aim of this work was to analyze and comprehensively present the Spanish results of the European survey, to highlight the particularities of the autonomous regions and also to contribute to the discourse of progress and uniformity in ophthalmologic training throughout Europe.
MethodsCreation and dissemination of the questionnaire and collection of dataThis was a survey on the topic of "Cataract surgery training and learning among European residents," entailing 23 anonymous questions divided into five sections. The query, addressed to EBO diploma examination candidates from the past five years (2018–2022), was distributed electronically via SurveyMonkey (San Mateo, California, USA). Invitations were sent out by the EBO executive in May 2022 and the survey ended in July 2022. Identification of participants was limited to their city and country, and the study was approved by the ethics committee of the French Society of Ophthalmology (IRB 00008855 Société Française d'Ophtalmologie IRB#1).
Spanish data collectionFor the statistical analysis, the Spanish data collection was divided into subgroups, corresponding to the autonomous regions of Spain.
Statistical analysisDescriptive statistical analysis of the quantitative variables was performed using measures of position and dispersion for each variable. The normality of the data was contrasted using the Shapiro–Wilk test and a Q-Q or quantile-quantile plot. Categorical variables have been described by indicating the number and proportion of each category. Contingency tables have been included for the description of the joint distribution.
The independence of the binary variables was tested using Fisher's test and when the variables had more than two categories we used the chi-square test. Since we had a large number of contrasts, we applied a Benjamini–Hochberg multiple comparisons correction, with a false rejection rate of 0.05 (post hoc tests). Comparison of the means of quantitative variables, which can be considered normal, was performed with a Student's t test, with possibly different variances (Welch's test). When normality cannot be assumed, the nonparametric Mann-Whitney–Wilcoxon test was used. We also corrected p-values for multiple comparisons using the Holm–Bonferroni method, with a false rejection rate of 0.05. Dependence between quantitative variables was assessed with Spearman's rank correlation coefficient ρ (ro) and we contrasted whether it can be considered null. Multivariable analyses were performed using sex, skill, surgical experience outside the EU, duration of specialist training and year of residency as explicit variables. A value of p < 0.05 indicated statistical significance. The statistical study was performed with the R v 4.2.1 program (R. Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org) with all the necessary packages for performing the different analyses.
ResultsCharacteristics of the intervieweesThe survey was sent to 135 ophthalmologists who indicated that they had completed residency training in Spain and met the inclusion criteria; namely, having participated in the EBO exam between 2018 and 2022.
The specific aim was to detect the self-confidence of the participants to operate cataracts as the first surgeon, perform complex surgery, solve a capsular rupture and perform a corneal suture. It was recorded using a Likert scale, graduated from 0 (no confidence) to 10 (confidence). A total of 93 responses were received from Spain. The response rate was 68.9%. Just under two-thirds (60.2%) had passed the EBO exam in the period 2021−2022, the remaining 37 had passed in 2018−2019. The characteristics of the participants are summarized in Table 1.
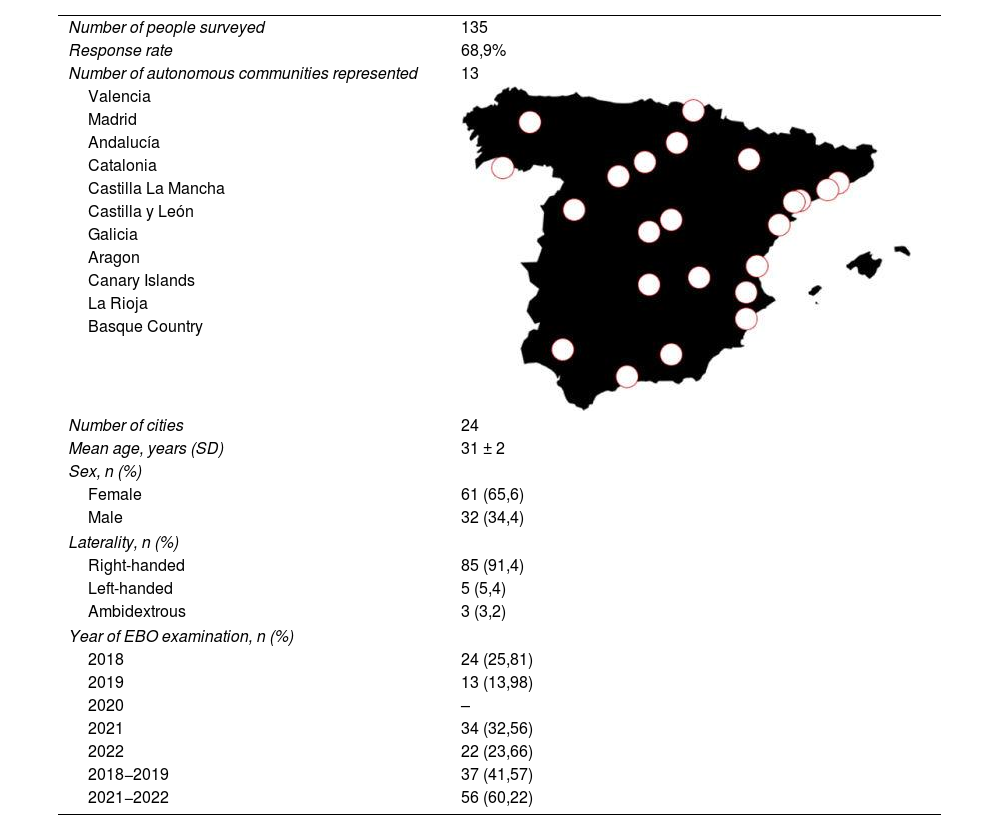
Demographic characteristics of study participants.
| Number of people surveyed | 135 |
| Response rate | 68,9% |
| Number of autonomous communities represented | 13 |
| Valencia | |
| Madrid | |
| Andalucía | |
| Catalonia | |
| Castilla La Mancha | |
| Castilla y León | |
| Galicia | |
| Aragon | |
| Canary Islands | |
| La Rioja | |
| Basque Country | |
| Number of cities | 24 |
| Mean age, years (SD) | 31 ± 2 |
| Sex, n (%) | |
| Female | 61 (65,6) |
| Male | 32 (34,4) |
| Laterality, n (%) | |
| Right-handed | 85 (91,4) |
| Left-handed | 5 (5,4) |
| Ambidextrous | 3 (3,2) |
| Year of EBO examination, n (%) | |
| 2018 | 24 (25,81) |
| 2019 | 13 (13,98) |
| 2020 | – |
| 2021 | 34 (32,56) |
| 2022 | 22 (23,66) |
| 2018−2019 | 37 (41,57) |
| 2021−2022 | 56 (60,22) |

This table is an overview of the demographic characteristics of the Spanish sample participants. It includes representatives from 24 cities in 13 of the 17 autonomous regions. Three cities from three communities (Valencia, Madrid and Barcelona) account for 64.5% of the sample studied. The typical participant is a 31-year-old right-handed woman who passed the exam between 2021 and 2022.
Most of the responses were provided by women: 65.59% (N = 61). The mean age of the participants was 31 ± 2 years. The majority, (91.4%) were right-handed and only three reported being ambidextrous (3.23%). The duration of the residency was four years in all cases, as is legally established for MIR training in Spain.
Twenty-four cities from 13 of Spain's 17 autonomous communities and two autonomous cities are represented. Three autonomous communities, in this order, accounted for more than half of the responses (64.5%): the Community of Valencia, the Community of Madrid and Catalonia. In 16 (17.2%) cases the place of training was not answered.
Cataract surgical trainingThe percentages of responses acknowledging 10 or more training sessions in animal eyes (wetlab), synthetic (drylab) and virtual reality simulator (VRS) were 16%, 3.2% and 8.7%, respectively. There was no geographic relationship between those who reported more than 10 simulation sessions (with any simulation system). We calculated whether there was a significant difference in self-confidence between participants who followed 10 or more animal eye training sessions and those who did not. We show that the referred self-confidence to manage a posterior capsular rupture was significantly higher in the group of the former with 10 or more animal eye training sessions (8 versus 6, p = 0.025).
All participants claimed to have performed cataract surgical steps on patients during their residency and in the first three years. The first surgical steps were performed by the vast majority of R1 (67.7%). Twenty-eight percent would have been performed by R2 and 4.3% by R3.
The usual technique among those who learned to operate on cataract patients was phacoemulsification (98.9%), followed anecdotally by manual small incision extraction (MSICS, 1.1%). No participant reported learning extracapsular cataract surgery (ECCE).
Of the total number of respondents, only three (3.2%) had performed cataract surgery on patients outside the European Union during their residence. The countries visited were Haiti, Kenya or Senegal. This experience had no significant influence on their self-confidence to be a first surgeon, to operate on difficult cases or to handle capsular ruptures.
The phacoemulsification steps performed under the supervision of an experienced surgeon, those that were reported as more complicated and those that remained equally as more difficult at the end of the residency, are represented in Fig. 1. These maneuvers, more difficult at the beginning and at the end of the residency in the Spanish sample, do not differ much from the European consensus referring to nuclear fracture (cracking) and capsulorhexis. Between the beginning and the end of the MIR, the change in the self-perception of difficulty goes from 64 to 26 respondents in nuclear fracture, and from 6 to 21 in capsulorhexis, which constitutes a variation in the confidence factor from 2.4 to 2.9 or, in other words, the participants who report having difficulties at the end of the residency are divided by three. In other respects, we also found similar data to the European cohort with initial training in corneal incision and IOL implantation associated with viscoelastic extraction.
 First step of phacoemulsification to be learned. Incisions (main and paracentesis) are the most commonly cited, followed by lens implantation and viscoelastic removal. (B) Most difficult maneuver to learn. At the beginning of the residency, cracking was the most frequently cited. At the end of the residency, while both maneuvers are always perceived as complicated, the number of participants citing them is divided by three.")
(A) First step of phacoemulsification to be learned. Incisions (main and paracentesis) are the most commonly cited, followed by lens implantation and viscoelastic removal. (B) Most difficult maneuver to learn. At the beginning of the residency, cracking was the most frequently cited. At the end of the residency, while both maneuvers are always perceived as complicated, the number of participants citing them is divided by three.
Table 2 summarizes, for each of the autonomous communities, the number of interventions partially or completely performed before finishing the specialty, as well as self-confidence in the performance of different procedures. It shows that the most populated autonomous communities are by far the most represented in our study sample, with the marked exception of Andalusia. The mean number of partial or complete procedures reported was 151.2 and 181.6, respectively, much higher than the European average, which places Spain among the five countries with the highest number of cataract surgery training during residency in Europe. Furthermore, the results reveal a high confidence in the performance of ordinary cataract surgery (mean score of 7.5/10), which contrasts with lower scores in confidence in the performance of complex surgeries (6.0), in the resolution of complications (6.0) and in the performance of corneal suturing3,4; even so, Spaniards are above the European average in the confidence indexes (2.4–4.2).
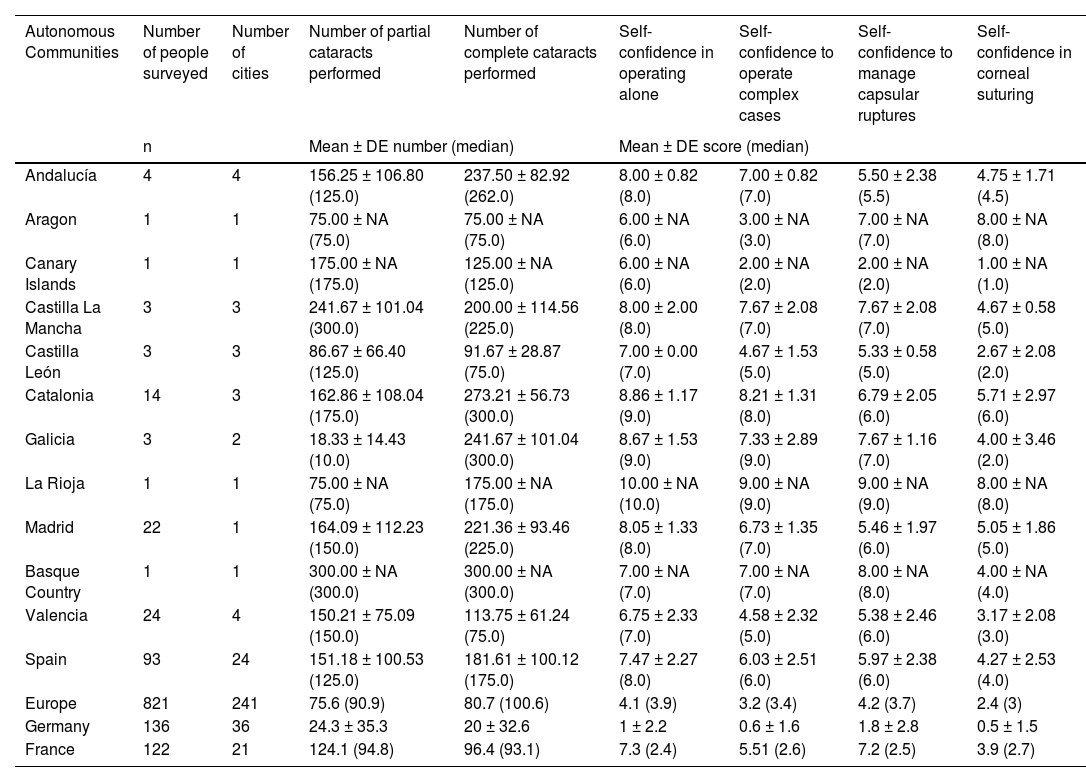
Surgical experience and confidence intervals in cataract surgery.
| Autonomous Communities | Number of people surveyed | Number of cities | Number of partial cataracts performed | Number of complete cataracts performed | Self-confidence in operating alone | Self-confidence to operate complex cases | Self-confidence to manage capsular ruptures | Self-confidence in corneal suturing |
|---|---|---|---|---|---|---|---|---|
| n | Mean ± DE number (median) | Mean ± DE score (median) | ||||||
| Andalucía | 4 | 4 | 156.25 ± 106.80 (125.0) | 237.50 ± 82.92 (262.0) | 8.00 ± 0.82 (8.0) | 7.00 ± 0.82 (7.0) | 5.50 ± 2.38 (5.5) | 4.75 ± 1.71 (4.5) |
| Aragon | 1 | 1 | 75.00 ± NA (75.0) | 75.00 ± NA (75.0) | 6.00 ± NA (6.0) | 3.00 ± NA (3.0) | 7.00 ± NA (7.0) | 8.00 ± NA (8.0) |
| Canary Islands | 1 | 1 | 175.00 ± NA (175.0) | 125.00 ± NA (125.0) | 6.00 ± NA (6.0) | 2.00 ± NA (2.0) | 2.00 ± NA (2.0) | 1.00 ± NA (1.0) |
| Castilla La Mancha | 3 | 3 | 241.67 ± 101.04 (300.0) | 200.00 ± 114.56 (225.0) | 8.00 ± 2.00 (8.0) | 7.67 ± 2.08 (7.0) | 7.67 ± 2.08 (7.0) | 4.67 ± 0.58 (5.0) |
| Castilla León | 3 | 3 | 86.67 ± 66.40 (125.0) | 91.67 ± 28.87 (75.0) | 7.00 ± 0.00 (7.0) | 4.67 ± 1.53 (5.0) | 5.33 ± 0.58 (5.0) | 2.67 ± 2.08 (2.0) |
| Catalonia | 14 | 3 | 162.86 ± 108.04 (175.0) | 273.21 ± 56.73 (300.0) | 8.86 ± 1.17 (9.0) | 8.21 ± 1.31 (8.0) | 6.79 ± 2.05 (6.0) | 5.71 ± 2.97 (6.0) |
| Galicia | 3 | 2 | 18.33 ± 14.43 (10.0) | 241.67 ± 101.04 (300.0) | 8.67 ± 1.53 (9.0) | 7.33 ± 2.89 (9.0) | 7.67 ± 1.16 (7.0) | 4.00 ± 3.46 (2.0) |
| La Rioja | 1 | 1 | 75.00 ± NA (75.0) | 175.00 ± NA (175.0) | 10.00 ± NA (10.0) | 9.00 ± NA (9.0) | 9.00 ± NA (9.0) | 8.00 ± NA (8.0) |
| Madrid | 22 | 1 | 164.09 ± 112.23 (150.0) | 221.36 ± 93.46 (225.0) | 8.05 ± 1.33 (8.0) | 6.73 ± 1.35 (7.0) | 5.46 ± 1.97 (6.0) | 5.05 ± 1.86 (5.0) |
| Basque Country | 1 | 1 | 300.00 ± NA (300.0) | 300.00 ± NA (300.0) | 7.00 ± NA (7.0) | 7.00 ± NA (7.0) | 8.00 ± NA (8.0) | 4.00 ± NA (4.0) |
| Valencia | 24 | 4 | 150.21 ± 75.09 (150.0) | 113.75 ± 61.24 (75.0) | 6.75 ± 2.33 (7.0) | 4.58 ± 2.32 (5.0) | 5.38 ± 2.46 (6.0) | 3.17 ± 2.08 (3.0) |
| Spain | 93 | 24 | 151.18 ± 100.53 (125.0) | 181.61 ± 100.12 (175.0) | 7.47 ± 2.27 (8.0) | 6.03 ± 2.51 (6.0) | 5.97 ± 2.38 (6.0) | 4.27 ± 2.53 (4.0) |
| Europe | 821 | 241 | 75.6 (90.9) | 80.7 (100.6) | 4.1 (3.9) | 3.2 (3.4) | 4.2 (3.7) | 2.4 (3) |
| Germany | 136 | 36 | 24.3 ± 35.3 | 20 ± 32.6 | 1 ± 2.2 | 0.6 ± 1.6 | 1.8 ± 2.8 | 0.5 ± 1.5 |
| France | 122 | 21 | 124.1 (94.8) | 96.4 (93.1) | 7.3 (2.4) | 5.51 (2.6) | 7.2 (2.5) | 3.9 (2.7) |
This table provides a detailed representation of the number of cataracts performed in each participating autonomous community as well as the results of the self-confidence scores. It can be seen that the more populated autonomous communities are more represented in our sample, with the exception of Andalusia. The mean number of partial and complete operations referred was, respectively, 151.2 and 181.6, much higher than the European average of 80.7, which ranks Spain among the five most training countries in cataract surgery during residency in Europe. Moreover, these results show a relatively high self-confidence in performing uncomplicated cataract surgery (mean score: 7.5), which contrasts sharply with low scores in self-confidence in performing complex surgery (1.3), in the management of complications (2.2) and in performing corneal sutures (1.3). In this aspect, Spaniards are below the European average (2.4–4.2). There were no significant differences between the different autonomous regions.
In the study of regional differences, we will focus on the autonomic subsamples with the highest number of responses. Regarding the number of cataracts performed alone, participants from Castilla-León and Valencia stated significantly less than those from Catalonia and Madrid (p < 0.001). Following these results, we observed lower confidence in operating cataracts and performing corneal sutures in the Valencian Community (p = 0.001) and higher in Catalonia (p = 0.008). Also, confidence in coping with difficult cases was lower in Castilla–León and Valencia (p = 0.001).
All respondents considered the importance of a surgical training fellowship to be 6.8 ± 2.8 (out of 10).
The lower part of the table compares the overall results of the countries with the highest number of participants, which are Germany and France, and Spain; it also compares them with those of Europe as a whole, demonstrating Spain's excellent position.
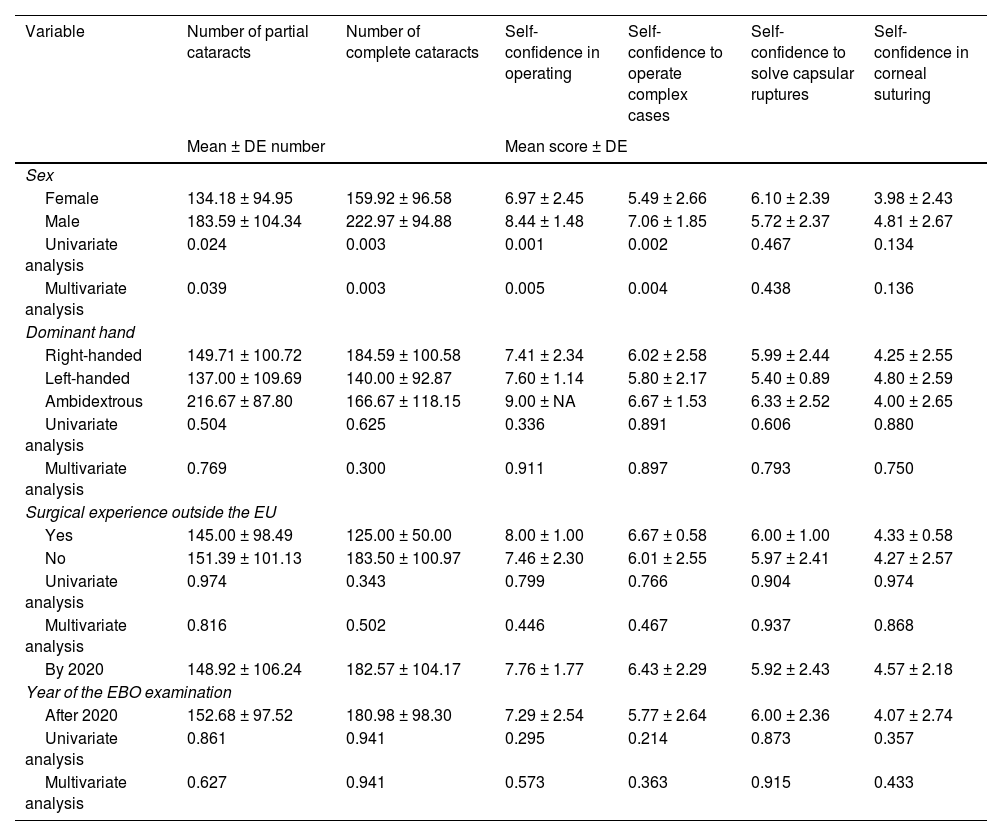
Table 3 summarizes a subgroup analysis according to sex, dominant hand, eventual surgical experience abroad outside the EU and the year in which they passed the EBO exam. Significant difference between sexes is observed in the number of incomplete (−27.3%, p = 0.003) or complete (−28.3%, p = 0.03), who are confident in performing surgery alone (−1.5, p = 0.005), as well as in operating complex cases (−1.6, p = 0.004), in both univariate and multivariate analysis.
Subgroup analysis according to participant characteristics and their influence on the number of surgeries performed and confidence indices.
| Variable | Number of partial cataracts | Number of complete cataracts | Self-confidence in operating | Self-confidence to operate complex cases | Self-confidence to solve capsular ruptures | Self-confidence in corneal suturing |
|---|---|---|---|---|---|---|
| Mean ± DE number | Mean score ± DE | |||||
| Sex | ||||||
| Female | 134.18 ± 94.95 | 159.92 ± 96.58 | 6.97 ± 2.45 | 5.49 ± 2.66 | 6.10 ± 2.39 | 3.98 ± 2.43 |
| Male | 183.59 ± 104.34 | 222.97 ± 94.88 | 8.44 ± 1.48 | 7.06 ± 1.85 | 5.72 ± 2.37 | 4.81 ± 2.67 |
| Univariate analysis | 0.024 | 0.003 | 0.001 | 0.002 | 0.467 | 0.134 |
| Multivariate analysis | 0.039 | 0.003 | 0.005 | 0.004 | 0.438 | 0.136 |
| Dominant hand | ||||||
| Right-handed | 149.71 ± 100.72 | 184.59 ± 100.58 | 7.41 ± 2.34 | 6.02 ± 2.58 | 5.99 ± 2.44 | 4.25 ± 2.55 |
| Left-handed | 137.00 ± 109.69 | 140.00 ± 92.87 | 7.60 ± 1.14 | 5.80 ± 2.17 | 5.40 ± 0.89 | 4.80 ± 2.59 |
| Ambidextrous | 216.67 ± 87.80 | 166.67 ± 118.15 | 9.00 ± NA | 6.67 ± 1.53 | 6.33 ± 2.52 | 4.00 ± 2.65 |
| Univariate analysis | 0.504 | 0.625 | 0.336 | 0.891 | 0.606 | 0.880 |
| Multivariate analysis | 0.769 | 0.300 | 0.911 | 0.897 | 0.793 | 0.750 |
| Surgical experience outside the EU | ||||||
| Yes | 145.00 ± 98.49 | 125.00 ± 50.00 | 8.00 ± 1.00 | 6.67 ± 0.58 | 6.00 ± 1.00 | 4.33 ± 0.58 |
| No | 151.39 ± 101.13 | 183.50 ± 100.97 | 7.46 ± 2.30 | 6.01 ± 2.55 | 5.97 ± 2.41 | 4.27 ± 2.57 |
| Univariate analysis | 0.974 | 0.343 | 0.799 | 0.766 | 0.904 | 0.974 |
| Multivariate analysis | 0.816 | 0.502 | 0.446 | 0.467 | 0.937 | 0.868 |
| By 2020 | 148.92 ± 106.24 | 182.57 ± 104.17 | 7.76 ± 1.77 | 6.43 ± 2.29 | 5.92 ± 2.43 | 4.57 ± 2.18 |
| Year of the EBO examination | ||||||
| After 2020 | 152.68 ± 97.52 | 180.98 ± 98.30 | 7.29 ± 2.54 | 5.77 ± 2.64 | 6.00 ± 2.36 | 4.07 ± 2.74 |
| Univariate analysis | 0.861 | 0.941 | 0.295 | 0.214 | 0.873 | 0.357 |
| Multivariate analysis | 0.627 | 0.941 | 0.573 | 0.363 | 0.915 | 0.433 |
This table shows a detailed analysis of the different variables collected and their predictive significance with regard to the frequency of procedures performed and the self-confidence indexes as objective variables. A net and significant difference between sexes is found for the number of partial or complete surgeries performed, which is also found for self-confidence to operate alone. including complex cases, both in the univariate and multivariate analysis.
The purpose of this study is to determine differences in cataract surgical training and to analyze their influence on the practical experience and self-confidence of ophthalmologists with recently completed training in the Spanish sample within a larger European cohort.
It is interesting to note that this sample is highly representative. In fact, Spanish ophthalmologists constitute the third largest group of candidates for the EBO exam.4 This is also reflected in the results of this survey. Three of the most populated autonomous regions5 are the three geographic areas with the largest number of participants in our study and from them we draw conclusions by region. A marked exception is Andalusia which, being the community with the largest number of inhabitants,5 is only the fourth in number of participants, far behind the first three. A plausible explanation could be that there are proportionally fewer ophthalmology MIR positions in Andalusia than in the Valencian, Madrid and Catalan communities.
The typical participant is female, in her thirties and right-handed, which perfectly reflects the image of a young female ophthalmologist, having completed her residency between 2018 and 2022. The representativeness of our sample could not be statistically supported because the sample was too small. The duration of the residency of four years makes Spain a country of short training in relation to the European average (France: 6 years; Germany: 5 years or more), so there is uniformity, since the duration of the MIR in Spain is regulated by law. In fact, it contrasts with other countries of study such as Germany, where residency can range from five to ten years.
The majority of respondents passed the EBO exam between 2021 and 2022, corresponding to the post-COVID period, which led to differences in the mode of examination with the possibility of taking the exam away from home.6 It could be inferred that this situation would have contributed to a greater interest in taking the exam.
It is also interesting to note that while 25% of the European respondents did not perform cataract surgery on patients during their training, all the Spanish participants reported having performed cataract surgery. Spanish residents were therefore among the five countries with the highest number of patients undergoing cataract surgery during their residency training, with a number of complete surgeries at the end of the MIR (223) almost three times higher than the European average (80.7) and ahead of France and Germany.2 Self-confidence in uncomplicated cataract surgery was also among the most remarkable in Europe as a whole, clearly evidencing a significant correlation (ρ 0.67, p < 0.01) between number of surgeries and self-confidence in performing uncomplicated cataract surgery. The latter correlation was already seen in the European cohort.2 The regional study confirms these results; indeed, participants from communities with a higher number of surgeries had greater self-confidence in performing uncomplicated cataract surgery and corneal sutures. However, it is relevant that this greater self-confidence was not found in the perception of confidence in operating on complex cases or in resolving complications. Of great interest in our study was the significantly positive role in confidence in resolving complications such as capsular rupture due to the training sessions. We will elaborate further on this issue.
Another important aspect is that in the European cohort there are two country trends: countries in which all residents learn to operate during their residency, as in France and Portugal, and countries in which surgical training is done after their residency, as in Germany or Denmark. These two models, which can be defined as structural as they have no regional variabilities even in federal countries like Germany, we identify as "surgery for all" in the first case (France, Portugal, among others) and surgeons "for high volume", in which only some learn to operate after residency.2
Spain is a clear exponent of the "surgery for all" model, with no regional disparity whatsoever. Perhaps one explanation for Spain's participation in this model could be that the shorter duration of residency has contributed to a contraction/intensification of the number of interventions.
With regard to one of the main missions of the EBO, concerning the improvement and harmonization of ophthalmologic education and training among European countries for the benefit of all citizens,7 it would be interesting to evaluate the two models: low number of "high volume surgeons" in relation to surgical training for all, based on objective criteria such as complication rate or duration of the intervention. The latter would make it possible to formulate better guidelines for European training requirements (ETR: European Training Requirements).
Considering the surgical steps most frequently performed at the beginning of training, similarity is found with the European cohort: surgery is learned in stages, starting at the beginning (incisions) and the end of the operation (lens implantation and viscoelastic removal).8,9 It is interesting to note that the incisions, the main elements required for a surgery without complications, are performed from the beginning of the learning process.
Both at the beginning and at the end of the residency, certain steps are perceived as particularly complex. Here we once again find results comparable with the European cohort; these are capsulorhexis and core fracture.10,11 At the end of the residency, although both maneuvers are always defined as difficult by a large number of residents, the latter is divided by three. The latter must be interpreted in relation to the large number of surgeries performed. The German sample also shows a progression, but less significant (−47%).
It is interesting to note that, unlike in other European samples such as Germany, Spaniards do not seek further training in countries outside the EU.
One of the most interesting results is the parsimonious confidence score for the performance of complex surgeries, resolution of complications and corneal sutures which is, despite the number of surgeries, much higher than the European average.2 There is in this statistically significant correlation between the number of surgeries and confidence scores, 0.68 (p < 0.01), 0.21 (p = 0.045) and 0.49 (p < 0.01), respectively. These results are interpreted in relation to the median score on the importance of post-residency training (7.0) which corresponds to the European median (7.7). A first explanation would lie in the number of surgeries required to reach sufficient level of competence (proficiency), established at a threshold of 250.12 The Spaniards would still be below this figure.
Another data point is that the detailed analysis of self-confidence highlighted a significant difference (8 versus 6) in the resolution of capsular rupture in those who had performed a significant number (>30) of training sessions on animal eyes (p = 0.0027).
Although self-confidence in the solution of a capsular rupture is supposed to be related to the number of operations performed, it is striking that the French participants, who have performed fewer surgeries, are more confident in solving this complication than the Spaniards. More complete information on the type of cataracts operated on by both groups could have revealed some explanation for this circumstance, and perhaps a partial explanation could lie in the greater number of sessions on virtual reality simulators reported by the French participants. Indeed, these devices also allow the simulation of complications and, therefore, the genesis of greater self-confidence in their resolution. Accordingly, Spain should encourage the use of virtual reality simulators among its residents.
Our results show a gap that could be filled with SBME (Simulation Based Medical Education). This is pre-patient training that represents the first step of a staircase learning system. It is articulated around different methods often associated; theoretical courses, wetlabs, drylabs and VRS. This training aims to reproduce real conditions, increases learning opportunities and places feedback at the heart of the acquisitions.13 Several studies have shown benefits for residents, patients and trainers. SBME effectively eases the learning curve, reduces operative time from the beginning of training, lowers the trainer's mental workload and decreases the number of complications. A study by Dean et al.,14 in 2020 on VRS, corroborated the previous results with a 70% reduction in the rate of capsular rupture in residents who had undergone pre-patient training.15,16 SMBE also allows for better resource allocation and more equitable access to surgical training.17
Unfortunately, our data clearly show that women have more limited access to surgical training in our country, but these figures are not unique to Spain, as seen in the results of the European sample and in a recent review of the literature18 which highlights that the "surgery for all" model does not seem to have the egalitarian effect of access to the operating room that it is supposed to have. Women report a significantly lower number of about one third of partial and complete operations than their male colleagues. Considering the correlation between the number of operations and self-confidence, it is not surprising that it is lower in women. The figures are homogeneous geographically and over time; they thus reveal a structural deficit. It should be emphasized that this problem is not specific to ophthalmology, but to all surgical specialties,19 which indicates the absolute need for a change in the training culture of ophthalmologists, taking into account that the number and proportion of female ophthalmologists will continue to increase. This change may go through measurement to identify an imbalance.
More tutoring or more flexibility in training courses would improve the implementation of better training pathways. The implementation of these measures would imply a long-term institutional involvement. The SBME also has a role to play in ensuring better access for a more personalized progression.
This study has some limitations. It is important to remember that we do not have a representative sample of Spanish residents but rather a group of volunteers who, in turn, are drawn from another selected sample, namely the participants of the EBO examination. On the other hand, the survey is retrospective and self-reported, leaving room for much subjectivity and the classic potential biases of this form of data collection such as memorization bias, social desirability bias, information bias, confirmation bias, or even nonresponse bias. Questions on the type of training center could have been missed; one could also argue not having asked about the desire and willingness to undergo training in surgery. These complementary questions would perhaps have facilitated a more reliable interpretation of the results.
ConclusionsThe study of surgical training in Europe identified a continent divided into two training models: surgical training for all versus high volume surgeons. On the other hand, the study of the Spanish sample places a homogeneous contingent that classifies, without any doubt, Spain in the "surgery for all" model with a number of cataracts completed by specialists in training almost three times higher than the European average. Although a significant unfavorable difference is noted in the reported number of cataracts operated on during residency by women, an opportunity towards a more equitable evolution is indicated. The SMBE could help to support this evolution.
FundingThis research has not received any grant or funding.
Conflicts of interestThe authors declare that they have no financial or proprietary interest in the material or methods cited.
The authors would like to thank the anonymous survey participants for their cooperation.
