









We treated 12 patients with bilateral xanthelasmas using an ultra-pulse CO2 laser. They were all extirpated, with no differences between the upper and lower eyelids. There were no cases of ectropion or bleeding. All the patients expressed a high level of satisfaction.
DiscussionThe use of the laser CO2 is a good therapeutic option for treating xanthelasmas especially those located in the lower eyelid, and in young people. It is a safe treatment for delicate periorbital regions, with a low risk of visible scars, and fewer recurrences. The technique can be performed outside the operating room avoiding the anxiety that is created by surgical intervention.
Se trataron a 12 pacientes con xantelasmas bilaterales mediante láser CO2 ultrapulsado. Todos fueron extirpados, sin diferencias entre el párpado superior e inferior. No hubo ectropión, ni sangrado. Todos los pacientes expresaron un gran nivel de satisfacción.
DiscusiónLa utilización del láser CO2 es una opción terapéutica buena para tratar xantelasmas, especialmente los localizados en párpado inferior y en gente joven. Es un tratamiento seguro para regiones delicadas de la periórbita: el riesgo de cicatrices visibles es bajo y hay menos recurrencias. La técnica se puede realizar sin quirófano, evitando con ello la ansiedad que se crea con una intervención quirúrgica.
Xanthelasma is a form of flat xanthoma which appears over the eyelids. It is the most disseminated form of xanthoma,1 forming slightly elevated yellow plates (cholesterol deposits) with clear limits of soft consistency, variable size and number, in small ducts or extended. They have a preference to establish at the level of the internal third of the eyelids, usually bilaterally and more frequently in females,1 with preference increasing with age. Xanthelasma is found in 20% of people affected by familial hypercholesterolemia and half exhibit dyslipidemia with alteration of apoprotein E or increased LDL.
The most usual treatment is surgical resection which, in the case of upper eyelids, produces positive esthetic results but in the lower ones there is a risk of ectropion. Recurrence is frequent, which places a limit on additional resections. For this reason, other approaches for treating the lesions are attempted, including trichloracetic acid peeling, CO2 laser or erbium: YAG. At present, CO2 laser is the gold standard for ablative laser types.2
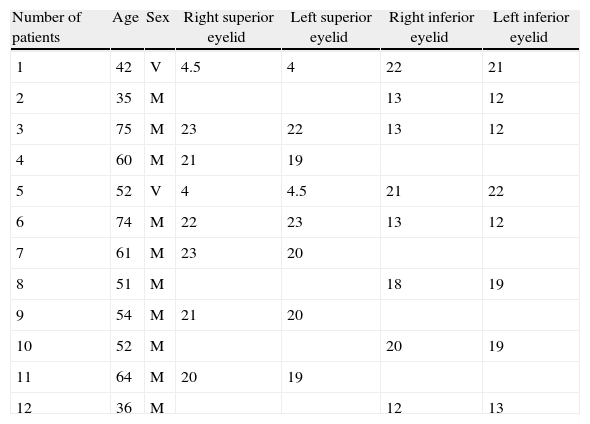
Surgical techniqueBetween October 2009 and April 2010, twelve patients were treated, 10 females and 2 males of ages between 35 and 75, a mean of 54.6. Two patients had high cholesterol levels. All the xanthelasma were bilateral, 4 were superior, 4 inferior and 4 superior and inferior. None had been treated previously. The size of the lesions is indicated in Table 1.
Size of lesions (mm) prior to treatment.
| Number of patients | Age | Sex | Right superior eyelid | Left superior eyelid | Right inferior eyelid | Left inferior eyelid |
| 1 | 42 | V | 4.5 | 4 | 22 | 21 |
| 2 | 35 | M | 13 | 12 | ||
| 3 | 75 | M | 23 | 22 | 13 | 12 |
| 4 | 60 | M | 21 | 19 | ||
| 5 | 52 | V | 4 | 4.5 | 21 | 22 |
| 6 | 74 | M | 22 | 23 | 13 | 12 |
| 7 | 61 | M | 23 | 20 | ||
| 8 | 51 | M | 18 | 19 | ||
| 9 | 54 | M | 21 | 20 | ||
| 10 | 52 | M | 20 | 19 | ||
| 11 | 64 | M | 20 | 19 | ||
| 12 | 36 | M | 12 | 13 |
The lesions were treated with ultrapulsating CO2 laser with previous application of intralesional anesthesia with epinephrine. The utilized device was «UltraPulse SurgiTouch» (Lumenis, Yokneam, Israel) with a power of 20W and an energy of 100mJ. The laser pulses were applied to the xanthelasma, and repeated in bursts over the lesion until it disappeared. After the laser treatment, the area was washed with chlorhexidin 0.05% and bacitracine cream was applied. After one week, the sores were removed with physiological solution, avoiding exposure to the sun in the treated area (Figs. 1–4). After one month the lesion was examined and all the patients were reviewed after 6 months and one year to identify side effects or recurrences. All the xanthelasma were extirpated without appreciating differences between the upper and lower eyelids.




One patient exhibited palpebral edema which remitted after 3 days with cold compresses and nonsteroid anti-inflammatory drugs. Another patient exhibited slight erithema which remitted after one month. In this series, only one dark-skinned male patient exhibited slight post-laser hypopigmentation (Figs. 5 and 6). This side effect depends on the pigmentation of the skin without affecting the size of the treated lesion.


One upper xanthelasma required 3 sessions and a further two required to sessions. No ectropion or bleeding in the lower eyelid appeared. All patients expressed a high level of satisfaction.3
DiscussionPalpebral xanthelasma is a benign lesion traditionally treated with surgical excision. However, there are alternatives to this treatment such as cauterization with trichloracetic acid, liquid nitrogen organic and inorganic acids, but all these options involve the risk of side effects.
Several publications3,4 have described the effectiveness of CO2 laser both in continuous and ultra-pulsation mode for the ablation of palpebral xanthelasma. At present ablation lasers are a good technique as they ensure minimum discomfort and fast recovery.2
Indications for the application of CO2 laser have progressively increased to include more dermatological benign lesions. However, the continuous mode caused high xanthelasma recurrence rates. With the appearance of the ultra-pulsation mode the thermal damage is restricted to the target area and the transmission of heat to adjacent healthy tissue is minimized together with texture changes in the irradiated skin. At this stage there are no standardized criteria for parameters to be applied.
The most frequently reported side effect is post-surgery hypopigmentation after the utilization of this laser.4 This is related to the pigmentation of the skin and increases with dark-skinned individuals.
The advantages of this method are that it ensures full control of the ablation of skin layers and therefore can be repeated in the case of recurrence. In addition, it is a safe treatment for delicate periorbital regions and, in contrast with continuous laser beam where the penetration depth is more difficult to control,5 the risk of leaving visible scars is low and the recurrence rate is also lower. Several authors have defined ultra-pulsation CO2 laser as an excellent therapeutic option even though, as in this report, their statistical information does not include a considerable number of patients.
The use of said CO2 laser is a good treatment for xanthelasma, mainly in young people due to the risk of frequent relapses and extirpations. It is also good for inferior xanthelasma to avoid residual ectropion which could appear in medium or large size xanthelasma. It can be treated as soon as diagnosed, it is fast, it does not require an operating room and therefore it excludes the anxiety which full-scale surgery can cause in some patients.
Conflict of interestsNo conflict of interests has been declared by the authors.
Please cite this article as: Delgado Navarro C, Lanuza García A, Llorca Cardeñosa A, Bañón-Navarro R, Corchero Martin G. Aplicación de láser CO2 para el tratamiento de xantelasmas palpebrales. Arch Soc Esp Oftalmol. 2013;88:320–322.
