


Asthma is a chronic inflammatory disease which is very prevalent throughout the world, and climatic factors, especially air humidity, have been considered fundamental to its development. This study aims to evaluate the relationship between the climate factor and the severity of asthma episodes in the semiarid region, comparing it to the coast and an intermediate climate region, considering the use of medication as an intervening factor.
Materials and methodsEcological study in cities with different climatic conditions (semiarid, intermediate region and Coast). Prevailing data was obtained from the International Study of Asthma and Allergies in Childhood (ISAAC) protocol. We evaluated the temperature, humidity and use of drugs for asthma/100,000 inhabitants.
ResultsThe prevalence of asthma was lower in the semiarid (14%; 95%CI=12.1–15.7) than the intermediate region (19.1%; 95%CI=17.7–20.6) and coast (17.9%; 95%CI=16.6–19.2). Episodes of severe asthma attacks were surprisingly higher in semiarid (10.4%; 95%CI=8.9–11.9) when compared to coast (4.1%; 95%CI=3.4–4.9) and intermediate region (5.0%; 95%CI=4.3–5.8). In the semiarid region, the humidity was lower and the temperature higher than the other cities evaluated. The dispensing of medications was lower in the semiarid region.
ConclusionsTemperature and humidity may have contributed to a lower prevalence and greater severity of asthma in the semiarid region. The dispensing of medications was lower in the semiarid region, indicating that access to both relief and control drugs was lower in this city. The possibility of lack of health care in the semiarid region can also be another explanatory factor associated.
Asthma is a chronic inflammatory disease of the airways common in childhood,1 which is very prevalent throughout the world, and climatic factors, especially air humidity, have been considered fundamental to its development, given the low prevalence found in desert regions compared to places where humidity and rainfall are higher, as in tropical regions.2–8
This feature may be related to the incidence of house dust mites that have reduced survival in low humidity locations, since they are a major determinant of allergic sensitization.4–11 In this case, in the dry climate regions, other agents could be responsible for the onset of asthma such as pollens, air pollution, small sensitizing particles present in soils, animal epithelia and the use of humidifiers in homes.4,9,10
A study carried out in the semiarid region of Pernambuco (Petrolina, PE), documented the prevalence of active asthma lower than that of other centers in the same state, as well as the Brazilian average,12 however, the prevalence of severe attacks episodes was surprising.2,12 It is possible that in the hot dry weather the patients have a more severe phenotype of the disease, but on the other hand, this fact may indicate a possible lack of recognition and control of the disease. Is the lower prevalence of asthma, as well as the greater severity observed in the semiarid region due to environmental conditions or the non-recognition and control of the disease? Thus, the objective of this research was to conduct an ecological study to investigate the relationship between climate and/or humidity factors and episodes of severe asthma attacks in the semiarid, comparing it to the coastal and an intermediate climate region of Pernambuco, including the use of medication in each city to verify the influence of access to treatment.
Materials and methodsAn ecological study in which the units of analysis were the cities of Petrolina, Caruaru and Recife, all in the state of Pernambuco, Brazil. In these units, the temperature, humidity and consumption of asthma medications (inhaled short-acting beta2 agonists, inhaled steroids and the long-acting agonist beta2 agonist and inhaled steroid) were evaluated. This research was approved by the Ethics Committee on Human Research of Universidade de Pernambuco (protocol: 459.304).
Recife is a Brazilian city located on the coast of the Northeast Region, capital of the state of Pernambuco (PE), and with about 1,538,000 inhabitants.13 It is the largest urban conurbation in the northeast and the sixth in Brazil. Recife has a humid tropical climate,14 typical of the northeastern east coast, with average monthly temperatures always above 18°C, low thermal amplitudes and abundant precipitation throughout the year. The city of Petrolina is in the region of the Brazilian semiarid zone (named “sertão”), and is located in Submédio São Francisco and has about 337,683 inhabitants.13 The climate is classified as hot semiarid,14 characterized by high temperatures (>22°C) and scarce rainfall in winter (<250mm), with average air humidity around 58%. Caruaru is located in the Greater Agreste region in Pernambuco and the micro-region of Ipojuca Valley, with about 351,686 inhabitants.13 It has hot dry summers and mild rainy winters. The annual rainfall is 764mm and the air humidity is relatively high, with an annual average of 75%. Thus, we have represented three cities of different mesoregions with a warm climate, but with different levels of humidity.
The starting point for this ecological study was the prevalence of asthma in adolescents of 13 and 14 years old, observed in Petrolina,12 Recife2 and Caruaru.2 These surveys used the ISAAC questionnaire, translated and validated for Brazil for the ages of 13–14,2 conducted in the years 2003/2004 and 2014. This questionnaire has three modules (asthma, rhinitis and eczema) with up to eight questions each, and is self-applicable and easy to understand. The authors considered for classification of asthma prevalence or active asthma those who answered “yes” to the question “In the last 12 months, have you had wheezing?”. For the diagnosis of asthma, the authors considered those who answered “yes” to the question “Have you ever had asthma in your life?”. This question evaluates asthma diagnosed by a physician and for the diagnosis of a history of severe attacks of the disease, those adolescents classified as having active asthma who reported chest wheezing that was strong to the point of affecting speech. This questionnaire does not contain questions regarding the consumption of medicines, and the severity of the crisis may indicate the demand for urgent care.
The use of asthma medications was obtained through a database. The drugs analyzed were inhaled short acting beta 2 agonists (short beta 2), inhaled steroid (IS) and the association of long-acting beta2 agonist with inhaled steroid (IS+LABA). The amount of medication for the cities analyzed was standardized for medicine box/1000 inhabitants. (This data refers to all medications consumed for asthma in the cities provided by Marketing Respiratory Franchise – Rio de Janeiro, Brazil. It is the most reliable drug consumption data for asthma and it enables the evaluation of the efficacy of the medicines available for this disease.)
Relative humidity and temperature data were obtained through the National Institute of Meteorology (INMET)15 database from June 2014 to May 2016. A search was performed considering the year/month of occurrences in the cities evaluated using the Meteorological Database for Teaching and Research (BDMEP) and/or by analyzing the graphs provided by the automatic stations available on the Institute's own website.15
Statistical analysisThe data were processed and analyzed using the Statistical Package for the Social Sciences (SPSS), version 20.0 and GraphPad Instat (GraphPad Inc., San Diego, USA, Release 3.06, 2003). To test the data normality assumption, the Kolmogorov–Smirnov test was applied. Mean and standard deviation (SD) were used to present continuous variables, while categorical data were presented using absolute and relative frequencies. Bilateral values of p were calculated, and the significance level adopted was 5%.
The 95% confidence interval (95%CI) was calculated from the total number of individuals surveyed by the total number of the disease obtained in previous research. The comparison between the means was performed through analysis of variance (one-way ANOVA) with Tukey post-test, when necessary.
ResultsThe city located in the semiarid was configured as the one with the lowest prevalence of asthma among the analyzed cities. Although presenting a lower prevalence, the semiarid group surprised with greater disease severity, being more than twice the prevalence of all cities evaluated here and the Brazilian average (Table 1). The medical diagnosis of asthma showed no difference between the regions.
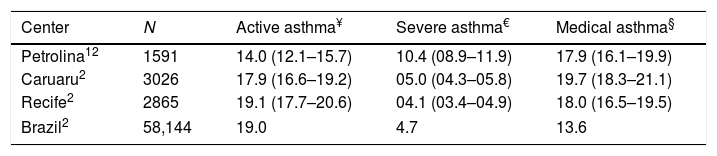
Prevalence of asthma and related symptoms in adolescents (13–14 years old) from different centers, determined by the protocol of the International Study of Asthma and Allergies in Childhood (ISAAC).
| Center | N | Active asthma¥ | Severe asthma€ | Medical asthma§ |
|---|---|---|---|---|
| Petrolina12 | 1591 | 14.0 (12.1–15.7) | 10.4 (08.9–11.9) | 17.9 (16.1–19.9) |
| Caruaru2 | 3026 | 17.9 (16.6–19.2) | 05.0 (04.3–05.8) | 19.7 (18.3–21.1) |
| Recife2 | 2865 | 19.1 (17.7–20.6) | 04.1 (03.4–04.9) | 18.0 (16.5–19.5) |
| Brazil2 | 58,144 | 19.0 | 4.7 | 13.6 |
The numbers were expressed as: ratio (95% confidence interval). ¥ - active asthma = wheezing in the last year; € - severe asthma = severe wheezing that may prevent you from saying two consecutive words in the last 12 months; § - medical asthma = asthma diagnosed by a physician.
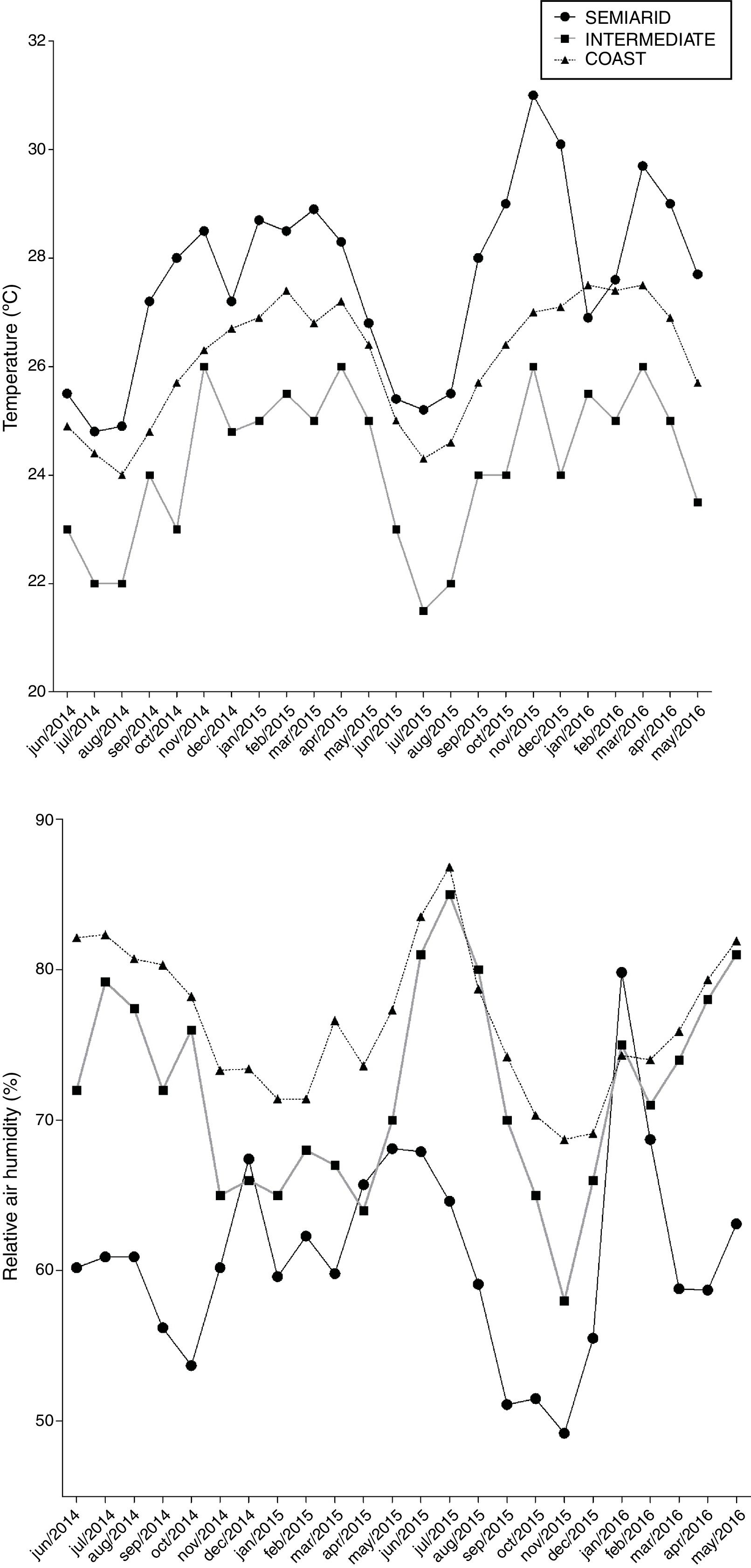
Relative air humidity (%) and temperature (°C) were different in the three cities (Fig. 1). The semiarid had the lowest humidity followed by intermediate climate and coast (51.0±6.7 vs. 71.9±6.8 vs. 76.5±4.9, p<0.001, respectively) and was the city with the highest temperature followed by coast and intermediate climate (27.6±1.7 vs. 26.1±1.1 vs. 24.2±1.4, p<0.001).
.")
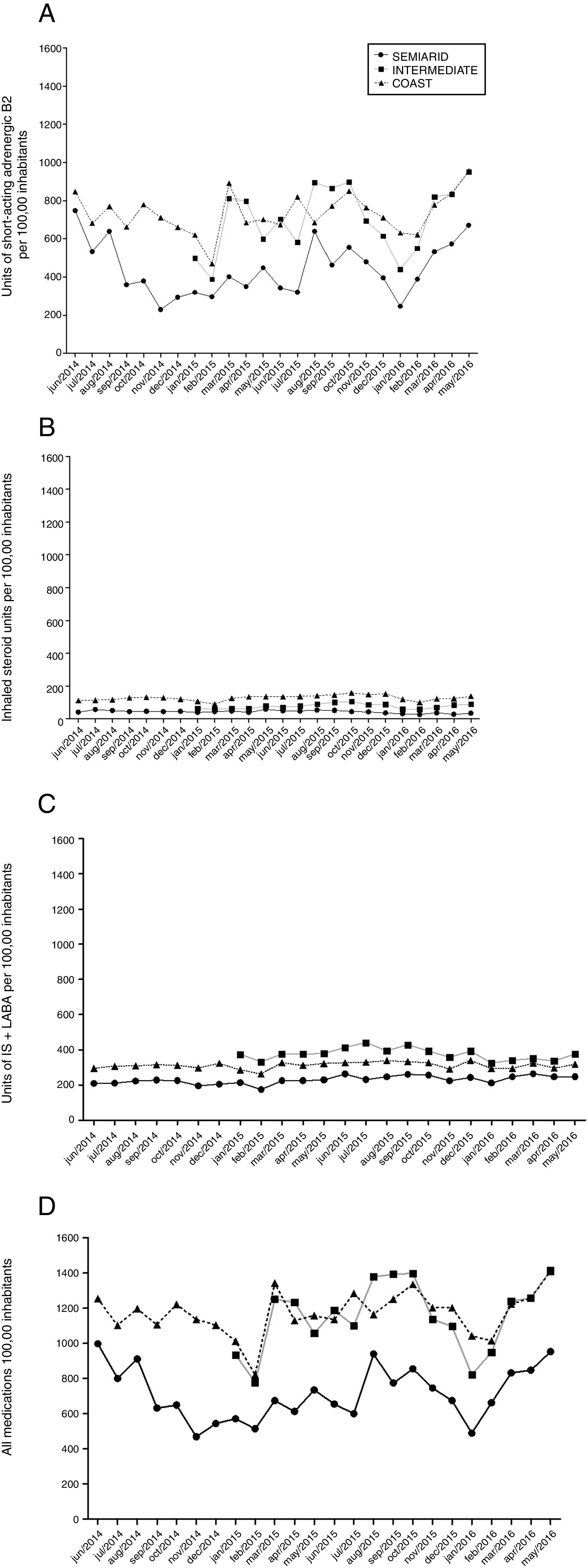
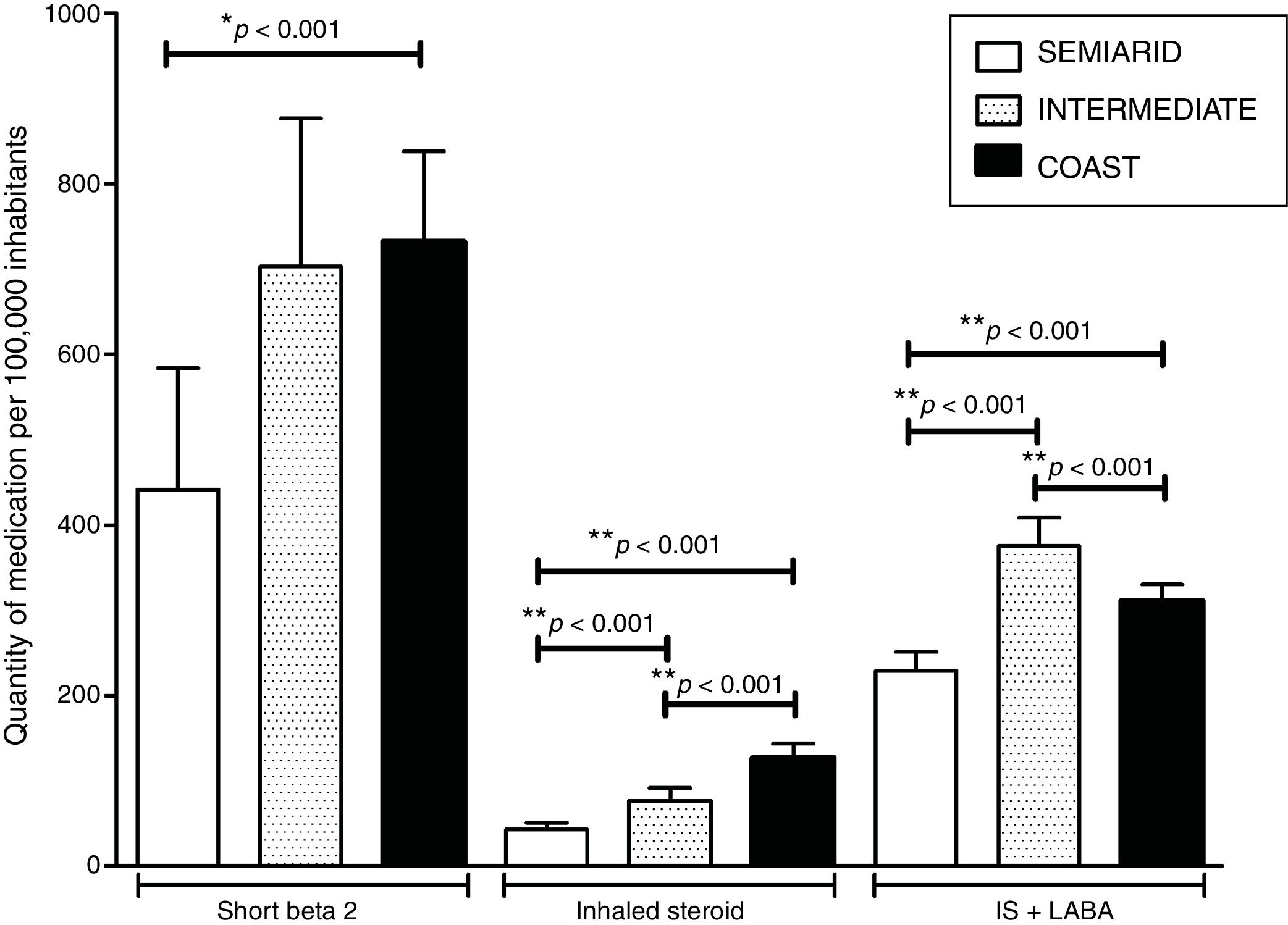
The consumption of medicine box/100,000 inhabitants (medicine box) in the cities of Petrolina, Caruaru and Recife according to the months of 2014, 2015 and 2016 are shown in Fig. 2 (short beta 2, IS, IS+LABA and all together). Fig. 3 shows that semiarid was the city that consumed less asthma medications compared to intermediate climate and coast in relation to the short beta 2 (441.7±142.2 vs. 702.5±173.6 and 732.2±105.7, p<0.001, respectively) for IS (42.8±8.4 vs. 76.5±15.3 and 127.1±16.5, p<0.001, respectively) and IS+LABA (228.9±16.5 vs. 375.5±33.3 and 311.3±18.9, p<0.001, respectively). With respect to IS sales, the coast was the city with the highest volume and intermediate climate with the highest number of IS+LABA.
 Short acting beta 2 agonists, (B) IS=inhaled steroid, (C) IS+LABA=association of beta 2 agonist with long-acting inhaled steroid, and (D) All medications together.")
Medicine boxes sold according to the months of 2014, 2015 and 2016 in the semiarid, in the intermediate and on the coastal regions.
(A) Short acting beta 2 agonists, (B) IS=inhaled steroid, (C) IS+LABA=association of beta 2 agonist with long-acting inhaled steroid, and (D) All medications together.
. **Statistical difference between all cities in the Inhaled Steroid and IS+LABA groups (p<0.001). ANOVA one-way test and Tukey post test.")
Mean and standard deviation of the medicine boxes sold in the period evaluated for asthma in the semiarid, in the intermediate and on the coast.
*Statistical difference between semiarid and other cities in the short beta 2 group (p<0.001). **Statistical difference between all cities in the Inhaled Steroid and IS+LABA groups (p<0.001). ANOVA one-way test and Tukey post test.
In this ecological study, the temperature and humidity were different between the cities of Petrolina (semiarid), Caruaru (intermediate climate) and Recife (coast). In addition, the consumption of medications/1000 inhabitants (short B2, isolated steroid and isolated steroid+LABA) was lower in Petrolina, indicating that access to both relief and control drugs was lower in this semiarid region. The results found in this research suggest that the greater severity of asthma observed in this city, in addition to the previously reported climatic factor,12 may indicate a lack of health care among adolescents with asthma in the semiarid region.
There is scientific evidence6,10,16 that dry climate hampers the survival of mites, which are one of the main sensitizing agents in respiratory allergies, since they require hydration obtained from the humidity of the air to survive becoming sensitive to the loss of water when the relative humidity of the air drops below 65% and lethal when below 55%. Thus, whilst the lowest prevalence of asthma in the semiarid zone (14%) was expected compared to the intermediate climate region (17.9%) and the coast (19.1%), the number of cases of severe asthma attacks episodes (more than double of the other cities) surprised us and the hypothesis that the dry climate could favor this finding needed more elucidation.
Epidemiological studies conducted in countries with major climatic variations during the year reported the driest season as the most prevalent for exercise-induced bronchospasm (EIB)17,18 and important research has described the onset of asthma after exercise with patients breathing dry air.19–21 The explanation for these findings may be related to the hyperventilation caused by physical exercise that results in the dehydration of the mucosa of the lower airways, especially in the periciliary fluid, generating an osmotic gradient in relation to epithelial cells that respond rapidly by transferring water. Dry sites may present an increase in this dehydration and consequently greater stimulus for a response to either epithelial cells, inflammatory cells or nerve fibers, releasing mediators capable of resulting in bronchospasm.21,22
Lack of access to or inappropriate use of anti-inflammatory drugs has a potential effect on the severity of the disease. By using standardized and globally recognized questionnaires,2 the studies carried out in the cities evaluated did not have access to medication consumption by adolescents. However, the observation of a greater severity of asthma in Petrolina reported in a previous study,12 when compared to other cities in the same region and with higher prevalence rates, reinforces the assertion that the higher frequency of episodes of severe asthma attacks in Petrolina may be due to the fact that patients do not have access to medicines in an appropriate way.
Although there are not many asthma education programs in Brazil, the provision of medications for the preventive treatment of asthma has been accompanied by encouraging results, with reduced morbidity and mortality rates due to asthma.23 A program developed to treat and follow-up patients with severe asthma in the northeast region of Brazil23 showed that the supply of inhaled corticosteroids was associated with a reduction in the number of hospitalizations and emergency care, reflecting the great impact of adequate management of symptoms of the asthmatic patient. Indirectly, these data corroborate the relationship between lack of treatment and greater severity of the disease allied to the climate.
In general, there is confusion with the question about wheezing in the chest so strong as to affect speech (severe asthma attacks), because it evaluates severe asthma episodes and not severe asthma itself. The fact that the number of medications sold/100,000 inhabitants in the semiarid region is always below the other cities evaluated reinforces the idea that these patients are not being adequately treated and adds, besides the influence of the climate, another question, about the presentation of episodes of severe asthma requiring emergency care and hospitalization.7,24–26 The cities located in geographic areas with high relative humidity would be related to increased atopic sensitization but could present forms with less intense crises.
This reinforces the Global Strategy for Asthma Management and Prevention (GINA)1 alert, regarding the global difficulty in controlling the disease. The Brazilian government provides free medication for asthma, with the potential for reducing symptoms and thus the spending on the health of the population. However, it seems that there is insufficient take-up, especially in the semiarid zone. Another possibility is that the reach of these programs is inadequate in small urban centers in the Brazilian interior.
A study developed in the northeastern region of the country,27 alerted to socioenvironmental conditions and geographical variability in the prevalence of asthma. In our study, the evaluated regions are in similar latitudes (Petrolina=−09°23′55″, Caruaru=−08°17′00″ and Recife=−08°03′14″), however, as already reported, they present very different climatic conditions of air temperature and humidity. In contrast to the previous group,27 the human development index (HDI) in these municipalities (Petrolina=0.697, Caruaru=0.677 and Recife=0.772)28 did not seem to influence the prevalence found. This research understands that despite the evidence verified by the previously mentioned authors,27 the humidity factor was a differential issue in the prevalence of asthma in the present study. In addition, information regarding the severity of asthma present in the ISAAC may generate important evidence in epidemiological studies regarding the lack of control of the disease. The findings related to Petrolina guide us to the importance of including new urban centers that use the ISAAC protocol in Brazil and the Northeast, since most of these centers are located especially in the coastal region.
A possible limitation of this study was the temporal gap between the surveys that used the ISAAC,2,12 however, the prevalence of asthma in the country has had small changes in recent years29 no more current research with these characteristics was found and a possible level of variation that did not invalidate the conjectures based on the findings found, except for an environmental disaster, it is unlikely that significant climate change occurred in this period. However, changes in the prevalence of the disease are dependent on different variables and need to be better studied, such as specific health policies for asthma, allowing better access to health services, medicines and specialized care that may have been implemented in the cities studied in this period. Another limitation to be considered is that ISAAC is validated for the ages of 13–14 years30 and epidemiological diagnosis of asthma, and thus, the value of this questionnaire in the assessment of severity is also epidemiological and refers to severe acute exacerbation and not the classification of the disease in the intercritical period. This is a fragility of the questionnaire, but it does not invalidate the hypothesis of the study.
It is important to highlight other factors involved in an assessment of this type of research, such as air pollution, exposure to infections, among other possible modifiers of asthma severity. Therefore, it is not possible to specify the relationship of each variable alone, climate and medication, with the severity of asthma, because that would be a reductionist approach. However, the evaluation of climatic factors together with the sale of medications allowed a greater clarification of the surprising report of episodes of history of severe attacks of the asthma in the region and with this, the possibility of directing public policies to solve this problem.
Thus, even with the questions and difficulties of interpretations inherent in investigations involving secondary databases that make definitive conclusions difficult, the study opens important perspectives and assumptions regarding the higher prevalence of severe attacks of asthma in the semiarid zone. In the semiarid region, the consumption of medicines for asthma for both relief and prevention is very low proportionally to the other two cities studied.
ConclusionsThe consumption of short beta 2, isolated steroid and IS+LABA was lower in the semiarid region, indicating that access to both relief and control drugs were lower in this city of the semiarid zone. Thus, in addition to climatic factors of temperature and humidity, the low consumption of medications suggests that there is a probable lack of health care among adolescents with asthma. Would this happen in other parts of the interior of Brazil and the world?
Conflict of interestThe authors report no conflicts of interest.
The authors are grateful to the National Council for Scientific and Technological Development – CNPq and Coordination for the Improvement of Higher Education Personnel (CAPES) for their research assistance and also to GSK for having made the drug database available. The authors would like to thank Chris Storey for help in reviewing our use of the English language.
