


To describe potential regional variations in therapies for severe asthma exacerbations in Chilean children and estimate the associated health expenditures.
MethodsObservational prospective cohort study in 14 hospitals over a one-year period. Children five years of age or older were eligible for inclusion. Days with oxygen supply and pharmacological treatments received were recorded from the clinical chart. A basic asthma hospitalization basket was defined in order to estimate the average hospitalization cost for a single patient. Six months after discharge, new visits to the Emergency Room (ER), use of systemic corticosteroids and adherence to the controller treatment were evaluated.
Results396 patients were enrolled. Patients from the public health system and from the north zone received significantly more days of oxygen, systemic corticosteroids and antibiotics. Great heterogeneity in antibiotic use among the participating hospitals was found, from 0 to 92.3% (ICC 0.34, 95% CI 0.16–0.52). The use of aminophylline, magnesium sulfate and ketamine varied from 0 to 36.4% between the different Pediatric Intensive Care Units (ICC 0.353, 95% CI 0.010–0.608). The average cost per inpatient was of $1910 USD. 290 patients (73.2%) completed the follow-up six months after discharge. 76 patients (26.2%) were not receiving any controller treatment and nearly a fourth had new ER visits and use of systemic corticosteroids due to new asthma exacerbations.
ConclusionsConsiderable practice variation in asthma exacerbations treatment was found among the participating hospitals, highlighting the poor outcome of many patients after hospital discharge, with an important health cost.
Asthma hospitalizations represent a serious adverse outcome for patients and their families. They are also related to important healthcare expenses, roughly equivalent to two billion dollars a year in developed countries such as the United States.1 A recently published study in Chile showed a significant increase in asthma hospitalization rates in 5–15-year-old children, from 3.8 per 10,000 inhabitants in 2001 to 7.8 per 10,000 in 2014.2 Most children hospitalized for asthma in Chile are younger than 12 years of age and almost 50% of them do not have an established diagnosis of asthma, and thus do not receive any controller treatment.3 There is a lack of information on treatment regimens used to manage pediatric asthma exacerbations in the different hospitals throughout the country and the associated health costs. The aim of this study was to describe potential regional variations in therapies and outcomes for severe asthma exacerbations in Chilean children, and to estimate the health expenditures associated with them.
MethodsThis was a prospective cohort study including 14 tertiary hospitals throughout Chile, eight in the capital, Santiago, and six in other regions of the country. Every child five years of age or older who was hospitalized with an asthma exacerbation between August 16th, 2015 and August 16th, 2016 was eligible for inclusion in the study. Asthma exacerbations were defined as acute episodes of increased shortness of breath, wheezing, chest tightness or a combination of these symptoms that require the use of rescue bronchodilators and systemic corticosteroids.
In each center, members of the research team identified eligible patients in hospital admission records on a daily basis from Monday to Friday. Patients were enrolled during the first 72h of admission, after obtaining written informed consent from the parents, and from the child if he/she was over 12 years of age. Prior to discharge, researchers gathered information on the length of stay, days with oxygen supply, pharmacological treatments received, isolated infectious agents and the presence of any complication from the clinical chart.
To estimate the average hospitalization costs for a single patient we defined a basic asthma hospitalization basket which included the costs of ward bed days, Intensive Care Unit bed days, medications and laboratory testing. The costs of each of these items were obtained from a price reference list published in a 2011 study by the Pontificia Universidad Católica de Chile on the expenditures of health care services.4 Prices were adjusted for inflation as of December 1st, 2016 and converted to U.S. dollars. The total value of the hospitalization basket was obtained from the sum of the quantity-frequency-price multiplication for every single service, supply or medication included in the basket.
Six months after discharge, patients received a phone call from the researchers to evaluate their clinical outcome, inquiring on new visits to the Emergency Room, new hospitalizations for asthma exacerbations, use of systemic corticosteroids, reported adherence to the controller treatment and attendance to medical checkups with a specialist in pediatric respiratory diseases.
To evaluate if there were any differences in asthma exacerbation treatments among the different centers, we made a comparison between public and private hospitals and between hospitals in different geographical regions. In Chile, the public health system covers the health expenditures of almost 80% of the population, including people of lower and middle income, while the private system covers the 20% of highest income.5 The public system has serious deficits in terms of infrastructure, equipment, supplies and medical staff, in particular specialists, compared to the private system. For the geographical comparison, hospitals were grouped into three different zones: north, central and south. These three zones differ in terms of climate, urban development, population density and medical infrastructure. The north zone has a desert or semi-arid climate and contains 11.8% of the population, the central zone has a Mediterranean climate and contains 60.5% of the population, while the south zone has a rainy temperate climate and contains 27.8% of the population. Health infrastructure is concentrated in the central zone, followed by the south and north zones. Asthma hospitalization rates for the selected ages were compared by geographical area and expressed per 10,000 inhabitants. The study was approved by the ethics committee of each participating center.
Statistical analysisCategorical variables were described through frequencies and percentages, and were compared across groups using Fisher's exact test. In order to compare hospitalizations between geographical zones, frequencies were transformed to rates to account for the heterogeneity of the zones’ demographical densities. The exposed population was defined as the number of 5–15-year old inhabitants, obtained from the demographic projections of the Chilean National Institute of Statistics.6 Length of stay, mechanical ventilation and use of medications and other treatments were described through the median and interquartile range and were compared using the Wilcoxon test and the Kruskal–Wallis test. The heterogeneity of therapies across medical centers was evaluated using the intraclass correlation coefficient (ICC). A significance level of 5% was used. The data was analyzed using Stata version 14.0.
ResultsDuring the study period 424 children with asthma exacerbations were hospitalized, 28 of whom could not be enrolled due to lack of consent or because they were admitted during the weekend and could not be investigated in time by the research team, resulting in a final sample size of 396 patients.
The hospitalization characteristics are presented in Table 1. Most patients belonged to the public health system and were living in the central zone. The rate of asthma hospitalization was significantly higher in the central zone than in the north and south zones (p<0.001). The median length of stay was four days (range 3–6). Patients treated in the public health system were hospitalized for one additional day compared to patients in the private health system, and patients in the north region were hospitalized for two more days compared to patients of the central and south zones (Tables 2 and 3).
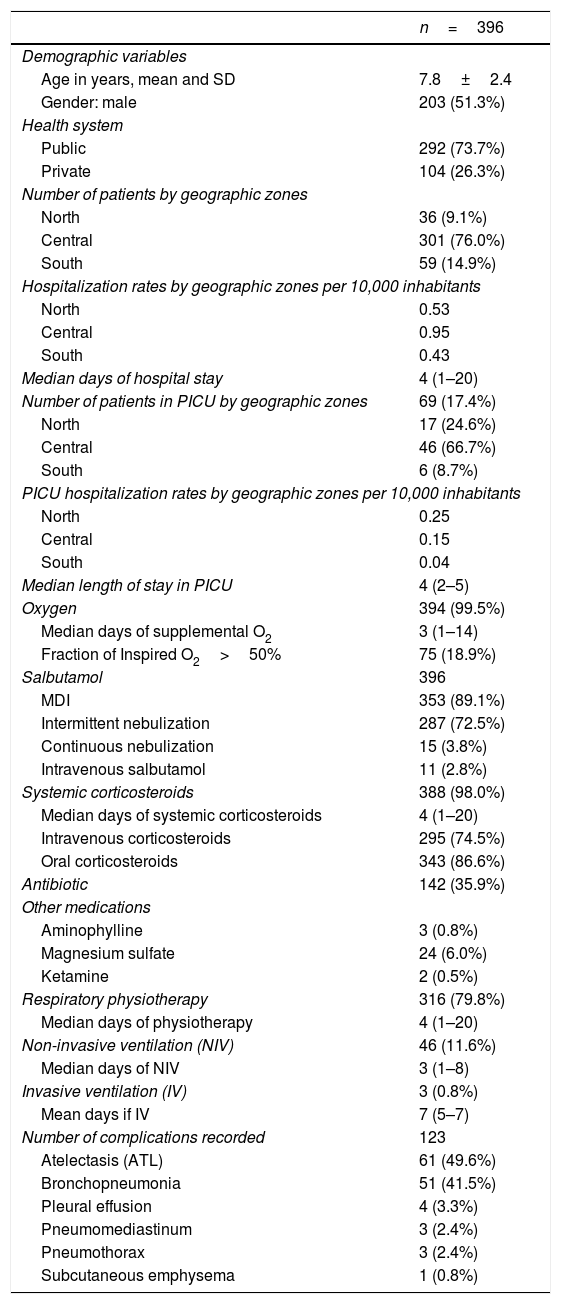
Hospitalized patients with asthma exacerbation.
| n=396 | |
|---|---|
| Demographic variables | |
| Age in years, mean and SD | 7.8±2.4 |
| Gender: male | 203 (51.3%) |
| Health system | |
| Public | 292 (73.7%) |
| Private | 104 (26.3%) |
| Number of patients by geographic zones | |
| North | 36 (9.1%) |
| Central | 301 (76.0%) |
| South | 59 (14.9%) |
| Hospitalization rates by geographic zones per 10,000 inhabitants | |
| North | 0.53 |
| Central | 0.95 |
| South | 0.43 |
| Median days of hospital stay | 4 (1–20) |
| Number of patients in PICU by geographic zones | 69 (17.4%) |
| North | 17 (24.6%) |
| Central | 46 (66.7%) |
| South | 6 (8.7%) |
| PICU hospitalization rates by geographic zones per 10,000 inhabitants | |
| North | 0.25 |
| Central | 0.15 |
| South | 0.04 |
| Median length of stay in PICU | 4 (2–5) |
| Oxygen | 394 (99.5%) |
| Median days of supplemental O2 | 3 (1–14) |
| Fraction of Inspired O2>50% | 75 (18.9%) |
| Salbutamol | 396 |
| MDI | 353 (89.1%) |
| Intermittent nebulization | 287 (72.5%) |
| Continuous nebulization | 15 (3.8%) |
| Intravenous salbutamol | 11 (2.8%) |
| Systemic corticosteroids | 388 (98.0%) |
| Median days of systemic corticosteroids | 4 (1–20) |
| Intravenous corticosteroids | 295 (74.5%) |
| Oral corticosteroids | 343 (86.6%) |
| Antibiotic | 142 (35.9%) |
| Other medications | |
| Aminophylline | 3 (0.8%) |
| Magnesium sulfate | 24 (6.0%) |
| Ketamine | 2 (0.5%) |
| Respiratory physiotherapy | 316 (79.8%) |
| Median days of physiotherapy | 4 (1–20) |
| Non-invasive ventilation (NIV) | 46 (11.6%) |
| Median days of NIV | 3 (1–8) |
| Invasive ventilation (IV) | 3 (0.8%) |
| Mean days if IV | 7 (5–7) |
| Number of complications recorded | 123 |
| Atelectasis (ATL) | 61 (49.6%) |
| Bronchopneumonia | 51 (41.5%) |
| Pleural effusion | 4 (3.3%) |
| Pneumomediastinum | 3 (2.4%) |
| Pneumothorax | 3 (2.4%) |
| Subcutaneous emphysema | 1 (0.8%) |
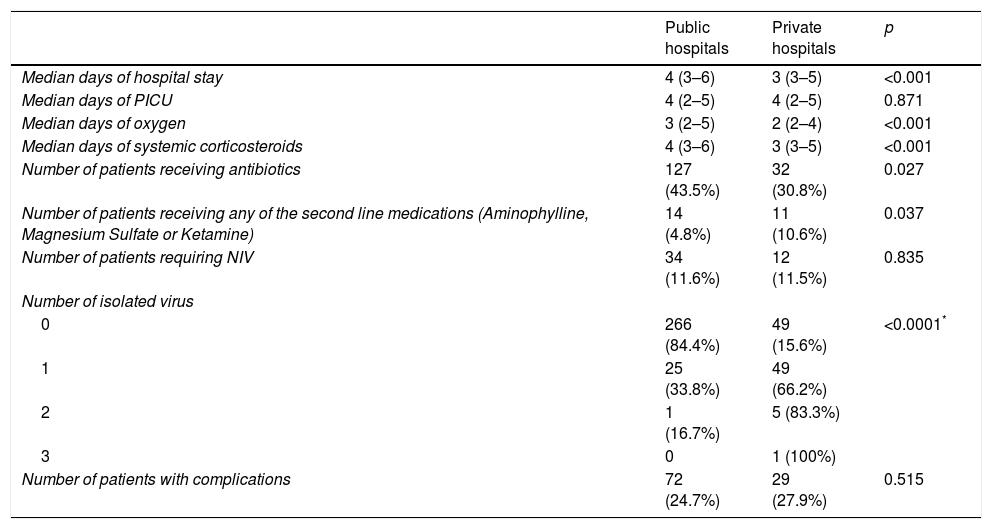
Asthma exacerbation in the public and private health systems.
| Public hospitals | Private hospitals | p | |
|---|---|---|---|
| Median days of hospital stay | 4 (3–6) | 3 (3–5) | <0.001 |
| Median days of PICU | 4 (2–5) | 4 (2–5) | 0.871 |
| Median days of oxygen | 3 (2–5) | 2 (2–4) | <0.001 |
| Median days of systemic corticosteroids | 4 (3–6) | 3 (3–5) | <0.001 |
| Number of patients receiving antibiotics | 127 (43.5%) | 32 (30.8%) | 0.027 |
| Number of patients receiving any of the second line medications (Aminophylline, Magnesium Sulfate or Ketamine) | 14 (4.8%) | 11 (10.6%) | 0.037 |
| Number of patients requiring NIV | 34 (11.6%) | 12 (11.5%) | 0.835 |
| Number of isolated virus | |||
| 0 | 266 (84.4%) | 49 (15.6%) | <0.0001* |
| 1 | 25 (33.8%) | 49 (66.2%) | |
| 2 | 1 (16.7%) | 5 (83.3%) | |
| 3 | 0 | 1 (100%) | |
| Number of patients with complications | 72 (24.7%) | 29 (27.9%) | 0.515 |
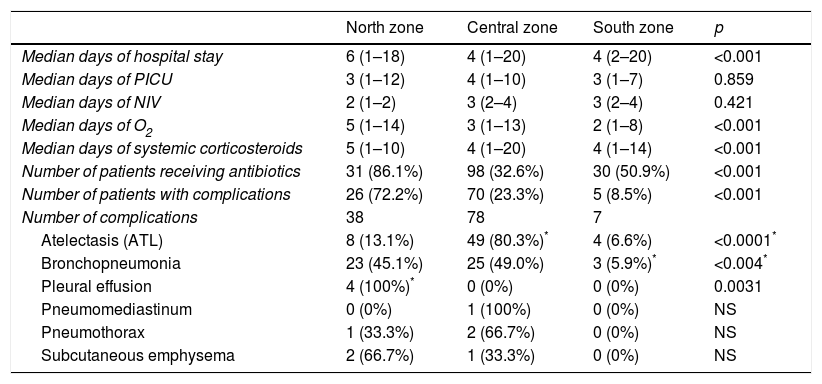
Asthma exacerbation in hospitals from different geographic zones.
| North zone | Central zone | South zone | p | |
|---|---|---|---|---|
| Median days of hospital stay | 6 (1–18) | 4 (1–20) | 4 (2–20) | <0.001 |
| Median days of PICU | 3 (1–12) | 4 (1–10) | 3 (1–7) | 0.859 |
| Median days of NIV | 2 (1–2) | 3 (2–4) | 3 (2–4) | 0.421 |
| Median days of O2 | 5 (1–14) | 3 (1–13) | 2 (1–8) | <0.001 |
| Median days of systemic corticosteroids | 5 (1–10) | 4 (1–20) | 4 (1–14) | <0.001 |
| Number of patients receiving antibiotics | 31 (86.1%) | 98 (32.6%) | 30 (50.9%) | <0.001 |
| Number of patients with complications | 26 (72.2%) | 70 (23.3%) | 5 (8.5%) | <0.001 |
| Number of complications | 38 | 78 | 7 | |
| Atelectasis (ATL) | 8 (13.1%) | 49 (80.3%)* | 4 (6.6%) | <0.0001* |
| Bronchopneumonia | 23 (45.1%) | 25 (49.0%) | 3 (5.9%)* | <0.004* |
| Pleural effusion | 4 (100%)* | 0 (0%) | 0 (0%) | 0.0031 |
| Pneumomediastinum | 0 (0%) | 1 (100%) | 0 (0%) | NS |
| Pneumothorax | 1 (33.3%) | 2 (66.7%) | 0 (0%) | NS |
| Subcutaneous emphysema | 2 (66.7%) | 1 (33.3%) | 0 (0%) | NS |
NS: non-significant.
69 patients (17.4%) required initial management in the Pediatric Intensive Care Unit (PICU). The median length of hospital stay in these patients was four days, comparable to those not requiring initial PICU treatment (p=0.110). The north zone showed a significantly higher PICU admission rate compared to the central and south zones (p=0.005).
TherapySupplemental oxygenAlmost all hospitalized patients received supplemental oxygen, with a median of three days and a mean fraction of inspired oxygen of 28%. Patients treated in the public health system and in the north zone received more days of oxygen compared to those treated in the private health system and in the central and south zones (Tables 2 and 3).
Pharmacological treatmentsSalbutamol. By our definition of asthma exacerbations, all hospitalized patients received salbutamol, most frequently using a metered-dose inhaler (MDI), followed by intermittent nebulizations (Table 1). Most patients received a median of two days of nebulized salbutamol followed by two days of salbutamol by MDI.
Intravenous salbutamol was used in seven medical centers, five of which were in the Metropolitan Region (central zone). The median days of hospital stay in patients receiving intravenous salbutamol was three, compared to four in patients only receiving salbutamol by inhalation (p=0.0047). Similarly, patients treated with intravenous salbutamol received systemic corticosteroids for a median of three days, compared to four days in patients not being treated with intravenous salbutamol (p=0.0167).
Systemic corticosteroids. Three hundred and eighty-eight (98%) patients received treatment with systemic corticosteroids with a median of four days (Table 1). Most patients first received intravenous corticosteroids for a median of two days, followed by three days of oral corticosteroids. Eight patients (2%) received only one dose of systemic corticosteroids in the emergency room without continuing its administration during hospitalization. Patients treated in the public health system and in the north zone received significantly more days of systemic corticosteroids compared with the private health system and with the central and south zones (Tables 2 and 3).
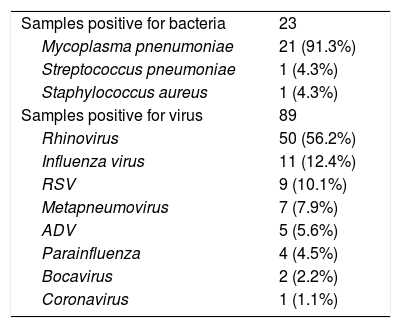
Antibiotics. One hundred and forty-two patients (35.9%) received antibiotics during their hospitalization (Table 1). In 49.8% of cases the prescription of antibiotics was either due to clinical suspicion or detection of Mycoplasma pneumonia, while in 36.8% of cases these drugs were prescribed because of the diagnosis of bronchopneumonia. Significantly more antibiotics were prescribed in the public health system and the north zone compared to the private health system and the central and south zones (Tables 2 and 3). Among the participating hospitals, heterogeneity was found in the use of antibiotics, from 0 to 92.3% (ICC 0.34, 95% CI 0.16–0.52).
Other medications used in PICU. Sixty-nine patients (17.4%) were hospitalized in the PICU, three of whom (4.3%) received aminophylline, 24 (34.8%) magnesium sulfate, and two (2.9%) ketamine (Table 1). The use of these medications varied from 0 to 36.4% between the different PICUs (ICC 0.353, 95% CI 0.010–0.608), being significantly greater in public than in private hospitals (Table 2). 25 patients were prescribed at least one of these three medications, 18 of whom (72%) simultaneously received ventilator support (p<0.0001).
Other proceduresAlmost 80% of patients received chest physiotherapy for a mean of three days. Non-invasive ventilation (NIV) was used in 46 patients (11.6%), without significant differences in its use between the public and private health systems (Table 2).
Complications and hospitalization costsA total of 82.6% patients with bacterial infections presented complications, compared to 33% observed in those without bacterial infections (p<0.001) (Table 4). The presence of any complication increased the length of stay by a mean of 1.62 days (p<0.001). There was no mortality in this study. The average cost per inpatient was of $1910 USD .
Asthma exacerbations. Infectious agents isolated.
| Samples positive for bacteria | 23 |
| Mycoplasma pnenumoniae | 21 (91.3%) |
| Streptococcus pneumoniae | 1 (4.3%) |
| Staphylococcus aureus | 1 (4.3%) |
| Samples positive for virus | 89 |
| Rhinovirus | 50 (56.2%) |
| Influenza virus | 11 (12.4%) |
| RSV | 9 (10.1%) |
| Metapneumovirus | 7 (7.9%) |
| ADV | 5 (5.6%) |
| Parainfluenza | 4 (4.5%) |
| Bocavirus | 2 (2.2%) |
| Coronavirus | 1 (1.1%) |
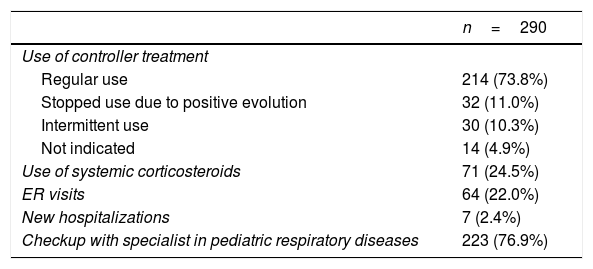
Two hundred and ninety patients (73.2%) completed the follow-up survey six months after discharge. Parents of 76 of these patients (26.2%) reported not giving their children any controller treatment. Nearly a fourth of these patients had had new ER visits and use of systemic corticosteroids due to new asthma exacerbations (Table 5).
Asthma exacerbations. Follow up six months after discharge.
| n=290 | |
|---|---|
| Use of controller treatment | |
| Regular use | 214 (73.8%) |
| Stopped use due to positive evolution | 32 (11.0%) |
| Intermittent use | 30 (10.3%) |
| Not indicated | 14 (4.9%) |
| Use of systemic corticosteroids | 71 (24.5%) |
| ER visits | 64 (22.0%) |
| New hospitalizations | 7 (2.4%) |
| Checkup with specialist in pediatric respiratory diseases | 223 (76.9%) |
This study showed important differences in asthma exacerbation treatment among the different participating centers. In the public health system, patients had an increased length of stay, more days with oxygen supply, and a greater use of systemic corticosteroids and antibiotics compared to the private health system. The same differences were observed comparing treatments by region. The north zone presented longer hospital stays, more days with oxygen supply, and a greater use of systemic corticosteroids and antibiotics compared to the central and south zones.
From a global standpoint, our results presented a higher percentage of antibiotic use (35.9%) in comparison to other series (15.7%).7 Only 49 of the 142 patients (34.5%) who received antibiotics had a recorded diagnosis of bronchopneumonia by chest X-ray or the presence of any bacteria by culture or serology. This suggests an overuse of antibiotics. A Cochrane review on the effectiveness of antimicrobials for asthma exacerbations concludes that their effect is difficult to evaluate due to the scarce number of available clinical trials.8 A recently published case control study showed no additional benefit of empirical use of antibiotics in children with an asthma exacerbation.9 Due to lack of scientific evidence on the use of antibiotics for asthma exacerbations, GINA guidelines recommend reserving its indication only for patients with clear symptoms of a lung infection, such as fever, purulent sputum and chest X-rays consistent with bronchopneumonia.10
Some 17.4% of patients required treatment in the PICU, an intermediate value between the 8% reported by an American study and the 20.3% reported in a Saudi study.11,12 The higher percentage found in this series in comparison with the American one could be due to a greater severity of exacerbations in our patients or to a lower threshold for PICU admittance and care. Our patients required a median PICU length of stay of four days, significantly higher than the median of one day found in another international series.11,13 This difference could be interpreted again as a higher severity in our patients, but the total length of stay of these patients was not longer in comparison with the patients that no required PICU treatment. This suggests that many patients treated in PICU were discharged directly from this Unit without later going to the pediatric ward. A great heterogeneity in the treatment of asthma exacerbations in PICU was also found. The use of medications, such as aminophylline, magnesium sulfate and ketamine differed considerably between PICUs, as was observed in an American study.11 Among the 7125 patients hospitalized in different PICUs in the USA, the use of aminophylline varied between 0 and 59%, magnesium sulfate between 9 and 46% and ketamine between 1 and 67%.11 The use of these medications was more common in patients requiring ventilator support, as we observed in our patients. On the other hand, the use of intravenous salbutamol in our study was considerably less common (15.9%) than in the American series (30.1%).11 Interestingly, these 11 patients who received intravenous salbutamol had a shorter length of stay and less use of systemic corticosteroids compared to children prescribed only inhaled salbutamol. Because the scientific evidence on the use on intravenous salbutamol is scarce and controversial,14,15 the potential benefit of early intravenous salbutamol in these patients should be evaluated through further randomized clinical trials.
In the present study, NIV was used frequently in PICU patients, 66.6% versus the 3% reported in an American study and the 36% reported in a Saudi study.1,11,12 Despite the potential beneficial effects attributed to NIV, there is no consensus in the literature on its use in clinical practice. A 2016 Cochrane review concluded that the available evidence at the time was insufficient to evaluate the effect of NIV on asthma exacerbations in children and that better designed studies with larger samples size are required.16 Anecdotal evidence suggests that NIV in asthma exacerbations may help to avoid or delay endotracheal intubation in children with severe exacerbations, with impending respiratory failure. Endotracheal intubation and invasive mechanical ventilation in these patients is associated with important morbidity such as barotrauma, hemodynamic instability, infections and an increased length of stay.17,18 In our study, invasive ventilation was used in only in 4.3% of cases, which is lower than the 14.4% in the American series.11 This could be related to the increased use of NIV in our patients. Despite the absence of good evidence in the literature regarding the treatment of asthmatics in the intensive care unit, it would be desirable to have greater treatment standardization between units, for example through guidelines specifically designed for the treatment of this kind of patients.
The important practice variations observed in asthma exacerbations treatment in this study could be due to differences in patients’ characteristics among the different participating hospitals or more likely, due to variations between doctors and their prescribing patterns and preferences between hospitals. This should be discouraged because this behavior increases costs and reduces quality of care.19
With regard to the viral agents isolated, important disparities were found between the private and the public health system. The former has better resources, including the availability of polymerase chain reaction testing for viral detection, while the latter relies only on using immunofluorescence techniques for a restricted number of viral agents. Despite this finding, it is important to emphasize that there is no scientific evidence that knowing the causative virus of an asthma exacerbation leads to improvement in outcome. For that reason, international guidelines recommend refraining from performing any microbiological testing or using antibiotics in children with asthma exacerbations.10,20,21
The mean hospitalization cost per patient calculated in this study was $1919 USD. Taking into account that on average 1800 children are hospitalized for asthma exacerbation yearly in Chile,22 the annual health costs for hospital treatment of asthmatic children in Chile amounts to $3,438,000 USD a year. This estimate does not take indirect costs into account, such as missed school days in patients and missed work days in their parents.
Despite the impact of the initial hospitalization, more than one in four patients remain without taking their controller therapy six month after discharge, requiring new visits to the Emergency Room and repeated use of systemic corticosteroids. We propose the initiation of a nationwide asthma program for hospitalized patients to reduce post-hospitalization morbidity and re-admissions. Such a program should include not only the medication, but also educational activities for patients and parents, emphasizing the importance of the adherence to daily controller treatment and providing the necessary tools for self-management, along with close follow up to avoid new exacerbations, lung function deterioration and increased risk of dying from asthma.23,24 Such programs have been successfully applied both in Latin America and elsewhere. In Belo Horizonte, Brazil, for example, implementation of such an asthma education and management program was associated with a 79% reduction in asthma hospitalizations, and in a nationwide program in Finland, asthma emergency visits decreased by 86% and hospitalizations by 88%.25,26
In conclusion, we found considerable practice variation in asthma exacerbations treatments among the participating hospitals, with excessive use of microbiological testing, chest X-rays and antibiotic use, highlighting the poor outcome of many patients after hospital discharge, with an important health cost. If we use some resources to implement a nationwide asthma program for this selected group of patients including controller treatment, education for patients and caregivers and close follow up, we could achieve better asthma control and outcomes for these children in a more cost-effective manner.
Conflict of interestThe authors have no conflict of interest to declare.
Ethical disclosureConfidentiality of dataThe authors declare that no experiments were performed on humans or animals for this investigation.
Protection of human subjects and animals in researchThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
